-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2017; 6(1): 1-5
doi:10.5923/j.otolaryn.20170601.01

Otitis Media in Infants - Is It Related to Improper Breast Feeding Techniques?
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLChaithra Shivakumara Swamy, Anil Kumar Ramabhadraiah, Borligegowda Viswanatha
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

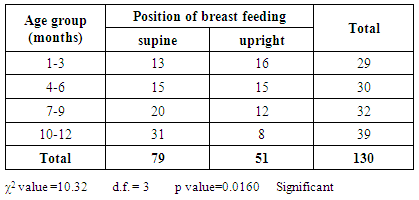
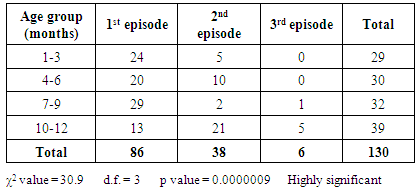
Background: Acute otitis media is the commonest illness of childhood. Feeding the child in supine position promotes reflux of milk and nasopharyngeal flora into middle ear via eustachian tube leading to otitis media. Aim of the study: To analyse the occurrence of acute otitis media in infants with improper breast feeding posture and also to study the bacterial profile in the study subjects. Materials and methods: 130 breast fed infants satisfying the inclusion criteria were included in the study. Study was conducted over a period of one year during February 2016 to January 2017. Detailed history, clinical examination including otoscopy was done. Aural swabs were sent for culture and sensitivity. Data was analysed by using chi square test. Results: Out of 130 infants, 79 were fed in supine position and 51 infants were fed in upright position. There was a significant association (p value=0.016) between incidence of ASOM and feeding in supine position. The incidence and frequency of otitis media among infants was higher with increase in age (highly significant with p value=0.0000009). The commonest age group affected was 10-12 months. 109(83.84%) infants had unilateral ASOM and 21(16.15%) had bilateral ASOM (not statistically significant). Haemophilus influenza was the commonest pathogen isolated from the aural swab cultures of study subjects. Conclusion: Prevalence of ASOM among infants increases with age. Improper breast feeding techniques like supine feeding is significantly associated with occurrence of acute otitis media in infants.
Keywords: Acute otitis media, Infants, Breast feeding
Cite this paper: Chaithra Shivakumara Swamy, Anil Kumar Ramabhadraiah, Borligegowda Viswanatha, Otitis Media in Infants - Is It Related to Improper Breast Feeding Techniques?, Research in Otolaryngology, Vol. 6 No. 1, 2017, pp. 1-5. doi: 10.5923/j.otolaryn.20170601.01.
1. Introduction
- Acute otitis media (AOM) is one of the commonest illnesses of childhood. AOM may be defined clinic-pathologically as inflammation of the middle ear cleft of rapid onset and infective origin, associated with a middle ear effusion and a varied collection of clinical symptoms and signs. It is synonymous with acute suppurative otitis media (ASOM). It normally develops behind an intact tympanic membrane, but may include acute infections arising in the presence of ventilation tubes or existing tympanic membrane perforations [1].Otitis media is in general a childhood disease, but occurs in adolescents and adults. In most children it resolves with anatomic and physiologic changes with growth. Until the condition has resolved, it may affect balance, hearing, and speech and language development and cause poor school performance. This disease affects not only the child but the whole family, from an economic as well as a societal Standpoint [2]. Varying prevalence rates of otitis media have been documented from various parts of the world [3-5]. Infants and young children are at highest risk of developing otitis media, with peak prevalence between 6 and 36 months of age. Two out of three children will have at least one episode of otitis media before their third birthday [6]. Bacteria have remained the most important etiological agents in suppurative or discharging otitis media [7-9].Various risk factors attributing to the etiology of otitis media are Eustachian tube anatomy in infants, upper respiratory infections (bacteria, viruses), pacifier use, position of feeding, genetic predisposition, allergy, parental smoking, parental education level, day care attendance etc [10-13]. The increased incidence of Otitis media in infants and young children may be attributed to the structural and functional immaturity of the Eustachian tube, and an immature immune system [14, 15]. The Eustachian tube in the infant is shorter, wider, and more horizontal than in the adult, which accounts for the high rate of otitis media in infants and children. AOM generally is characterized by rapid onset of signs and symptoms of inflammation in the middle ear accompanied by middle ear effusion. Signs of inflammation include bulging or fullness of the tympanic membrane (TM), erythema of the TM, and acute perforation of the TM with otorrhea [2]. Symptoms include rapid onset of otalgia, hearing loss, otorrhoea, fever, excessive crying, irritability, coryzal symptoms, vomiting, poor feeding, ear-pulling and clumsiness [1, 2].In the present study we have included breastfed infants with otorrhoea as study subjects. The objectives of our study were to analyse the occurrence of acute suppurative otitis media in infants with improper breastfeeding posture and also to study the bacterial profile in the study subjects.
2. Materials and Methods
- Infants with history of ear discharge (otorrhoea) visiting to the outpatient department of Sri Venkateshwara ENT Institute, Department of Otolaryngology, Bangalore Medical College and Research Institute within the period of 1 year from February 2016 to January 2017 were included in this study. Prior informed written consent was taken from the parents. 130 infants satisfying the inclusion criteria were included in the study. Infants who are not breastfed and those with cleft lip, cleft palate, craniofacial abnormalities and other co-morbidities were excluded from the study. Detailed history with regard to otorrhoea, frequency of occurrence of otorrhoea (no. of episodes), position of the infant while breast feeding (supine or upright), burping after feeding and the mother’s knowledge regarding breast feeding was recorded. A thorough ENT examination including otoscopic examination was done. Pus from the discharging ear was sent for culture and sensitivity. Collected data were then tabulated under categories such as age, sex, position of feeding, frequency of otitis media, laterality of otitis media and microorganisms isolated form culture swab. The data was statistically analyzed by chi square test.
3. Results
- A total of 130 breast fed infants were included in the study. Out of 130 infants there 72(55.38%) were male and 58(44.61%) female. Prevalence was more among males than females which was not statistically significant. (Figure 1)
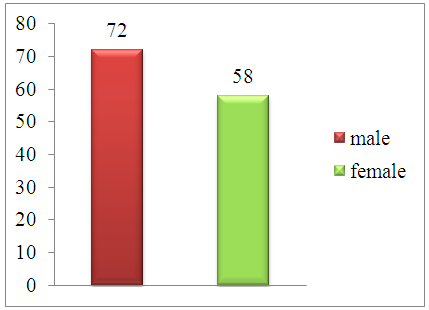 | Figure 1. Gender wise distribution of infants |
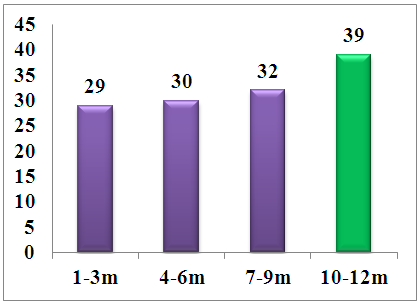 | Figure 2. Age wise distribution of ASOM cases |
|
|
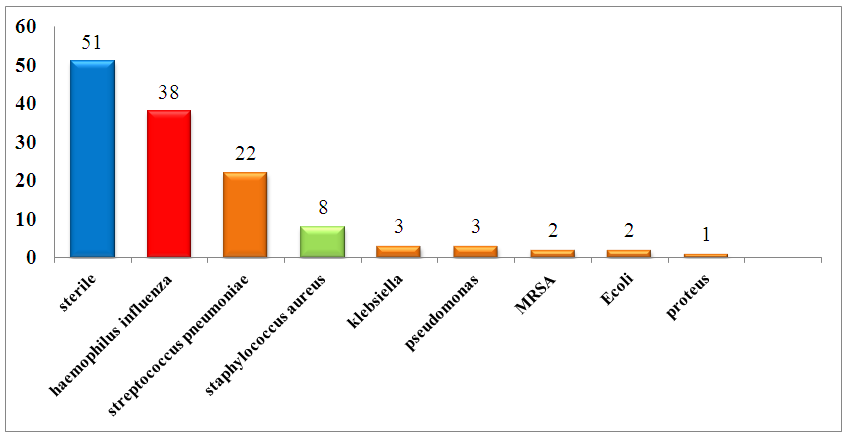 | Figure 3. Culture and sensitivity report of aural swabs of study subjects |
4. Discussion
- Acute otitis media is mainly an infection of early childhood [16]. Its incidence appears highest in the first year of life, more specifically the second six months of life in most studies, and gradually reduces with increasing age. This progression was shown by Strangerup and Tos who reported an incidence of a first episode of AOM in 22 percent in the first year of life, 15 percent in year two and 10 percent in year three, falling to 2 percent by year eight. Incidences of over 60 percent are stated in some reports of infants up to age of one Year. In the first two years of life, AOM occurs bilaterally in 80 percent of cases. After six years of age, it is unilateral in 86 percent [1].A prospective study done by Anniansson G et al showed that by one year of age, 85 of 400 (21%) children experienced 111 episodes of Acute Otitis Media (AOM). Of these 111 episodes, 7(6%) occurred by 2 months of age, 35 (32%) before 7 months and the remaining 69 (62%) episodes before 12 months of age [17]. Three potential routes of spread of infection are described: the Eustachian tube, tympanic membrane perforations or grommets, and haematogenous route. Of which Eustachian tube is considered to be the commonest route of spread of infection. In infants the Eustachian tube is short, straight and widely patent. Eustachian tube normally opens while swallowing, yawning etc. It is considered to be the main route by which the nasopharyngeal secretions and organisms reach the middle ear. Negative pressure in the middle ear may facilitate the movement of bacteria up to Eustachian tube [1]. Breast feeding the baby in supine (horizontal) or near so position facilitates the reflux of milk into middle ear, with carriage of respiratory flora into the middle ear space there by leading to otitis media [18, 19].In our present study the incidence of otitis media was more in infant fed in supine position as compared to those fed in upright position. This was statistically significant with a p value = 0.0160. There are similar studies inferring that incidence of otitis media is related to faulty feeding positions. Sangeetha et al in their study of the prevalence of otitis media and early childhood caries and their association with faulty breastfeeding technique, it was observed that 82.5% (p=.001) children experienced coexistence of OM and ECC who were fed in the combined feeding position (i.e.supine and head elevated). Of the 120 children enrolled in the study significant percentage, (25%) of children with Otitis media were fed in supine position [18]. A study done by Tully. S. B et al showed that, out of 90 children aged 7-24 months, there were abnormal tympanograms noted in 34(59.6%) of 57 infants fed in supine position while it was only 5 (15%) of 33 infants fed in semi upright position [20].Study by Fransciscus J W Timmermans on chronic granulomatous otitis media in bottle fed inuit children, 315 children were examined. 285 (238 Inuit children and 47 Caucasian children) out of 315 children were included in the study, 76 out of 238 children had otitis media. Clinical observations in their study suggests that formation of foreign body granuloma in the middle ear could be a result of entry of milk into middle ear due to high negative intraoral pressure during bottle feeding in supine position [21]. In various other studies it was observed that a significant number of children who werefed in supine feeding position were more prone to develop otitis media [22-25]. Both bacterial and viral infections are implicated in AOM. These infections may occur in isolation or combination. Streptococcus pneumonia, Haemophilus influenza and Moraxella catarrhalis are the most common bacteria causing acute otitis media [1]. In our study Haemophilus influenza was found to be the commonest pathogen isolated.
5. Conclusions
- 1. Prevalence of ASOM among infants increases with age. 2. Improper breast feeding techniques like supine feeding is significantly associated with occurrence of acute otitis media in infants.3. Parental education regarding proper breast feeding techniques during antenatal visits and immediate postnatal period will considerably reduce the incidence of otitis media in infants.