-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2016; 5(2): 21-27
doi:10.5923/j.otolaryn.20160502.01

Effect of Mobile Phone Use on Auditory Function
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPrem G. Nair 1, Dibina Shaji 2, Haritha Chandrahasan 1, Haritha Unnikrishnan 1
1Department of Speech Pathology and Audiology, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham University, Kochi, India
2Institute of Speech and Hearing, Marthoma College of Special Education, Kerala University of Health Sciences, Kasaragod, India
Correspondence to: Prem G. Nair , Department of Speech Pathology and Audiology, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham University, Kochi, India.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Mobile phone possession and usage have dramatically increased all over the world. The present study was done to characterize audiological profile of individuals who used mobile phones extensively and to correlate audiological test results with duration of mobile phone use. The study consisted of two groups of subjects: The clinical group comprised of 30 subjects who were using mobile phones for two or more hours per day for two years or more within the age range of 15-55 years (mean age: 28.6 years). It was decided to select very limited mobile phone users as comparison group (less than six months of overall mobile phone use and duration of less than 20 minutes per day). The group consisted of 30 age-matched (mean age: 24.6 years) normal hearing subjects. Audiological assessment consisted of puretone and speech audiometry, immittance audiometry and Distortion Product Otoacoustic Emissions (DPOAE). From the study, it was understood that long term mobile phone exposure adversely affects the auditory function. There were statistically significant mean differences in puretone average, all frequency average, high frequency average, Speech Reception Threshold, Speech Discrimination Score, Acoustic Reflex Threshold-Sensation Level and DPOAE values of clinical group when compared with comparison group (clinical group had poor scores). The dominant mobile phone used ear demonstrated poor scores on audiological tests. Further, auditory function seemed to deteriorate with increasing years and hours of mobile phone use. The present study clearly revealed hazardous effects of mobile phone use on auditory function. The risk and extent of damage would be greater in case of extensive usage. The knowledge on adverse effects of mobile phones on hearing is important to spread awareness among people for judicious use of the device.
Keywords: Mobile phone, Puretone audiometry, Speech audiometry, Distortion Product Otoacoustic Emissions
Cite this paper: Prem G. Nair , Dibina Shaji , Haritha Chandrahasan , Haritha Unnikrishnan , Effect of Mobile Phone Use on Auditory Function, Research in Otolaryngology, Vol. 5 No. 2, 2016, pp. 21-27. doi: 10.5923/j.otolaryn.20160502.01.
Article Outline
1. Introduction
- Mobile phone possession and usage have dramatically increased all over the world. Mobile phones are low power radio devices that transmit and receive radio frequency radiation. It is important to find out the effects and possible health hazards as a result of exposure to radio frequency fields from mobile phones. Review of literature revealed that there could be thermal and non-thermal effects of mobile phone use. Thermal effects could occur in the pinna, internal ear, surface of head and even in the brain. The fluid filled structures of inner ear are more susceptible to heating effect. Normal brain functions may be affected with continuous mobile phone use. Non-thermal effects include alterations in bio-cycles, cellular metabolism and can lead to auditory disturbances [1].Of all anatomical structures the ear is closest to mobile phone, which may lead to relatively high hazardous effect on ear compared to other parts of the body. This can in turn cause potential adverse effects on auditory function. Al-Abduljawad [2] had reported high degree of hearing loss with long-term use of the mobile phones. Panda et al [3] have reported that long-term and intensive mobile phone use may cause damage to cochlea as well as the auditory cortex. Cochlear outer hair cell damage was evidenced by Distortion Product Otoacoustic Emission (DPOAE) findings. With more than three years of Code Division Multiple Access mobile phone use, integrity of primary auditory cortex within the temporal bone seems to be influenced as evidenced by Na amplitude in Middle Latency Response. Panda et al [4] have reported that users with auditory complaints during mobile phone use demonstrated absent DPOAE and abnormalities in auditory brainstem response. Although researchers have attempted to study the effects of mobile phone use on auditory function, comprehensive audiological work-up on the same aspect is limited. Further, effect of long duration use of mobile phone on auditory function has not been thoroughly assessed. Such studies in the Indian context are also rare. Keeping these aspects in mind, the present study was formulated with an objective to comprehensively view this problem from a wider audiological perspective and to unravel more details on the auditory pathophysiology involved. Further, knowledge on adverse effects of mobile phones on hearing is also important to spread awareness among people. This could help people to use mobile phones more judiciously.
2. Methods
- The study consisted of two groups of subjects: The clinical group comprised of 30 subjects ((17 males and 13 females) who were using mobile phones for two or more hours per day for two years or more within the age range of 15-55 years (mean age: 28.6 years). Due to extensive mobile phone use among public, we were unable to find mobile non-users who were matching with the age range of clinical group. Hence, we selected very limited mobile phone users as comparison group (less than six months of overall mobile phone use and duration of less than 20 minutes per day). The group consisted of 30 age-matched (age range: 15-55 years; mean age: 24.6 years) normal hearing subjects (i.e., with puretone thresholds of 25 decibel-dB or below at octave frequencies from 250 Hertz-Hz - 8000 Hz, including 6000 Hz). The comparison group comprised of students and staff from Mar Thoma college of special education, Institute of Speech and Hearing, Kasaragod. The staff of Vodafone private limited company, staff from Chemmannur finance and students from Kasaragod Government College were included in the clinical group. Informed consent was obtained from all subjects. The study was conducted at Mar Thoma College of Special Education, Institute of Speech and Hearing, Kasaragod, Kerala, India and the ethics committee of the institute has approved the study (Ethical committee approval number: Ref:-Letter No. PG/Dissertation/4212/2013-dated 25/07/2013). Subjects with otological/neurological / psychiatric disorders, history of hearing problems, diabetes mellitus, hyperlipidemia, arterial hypertension, central or peripheral nerve diseases, congenital hearing disorders, exposure to noise and those using any ototoxic medications were excluded from the study. The study was completed within a period of one year. To assess effect of duration of mobile phone usage on auditory function, the subjects were grouped into four categories: Subjects who were using mobile phone not more than 20 minutes/day (group A); Subjects who were using mobile phone for 2-3 hours/day (group B); Subjects who were using mobile phone for 3-4 hours/day (group C) and Subjects who were using mobile phone for more than 4 hours/day (group D). The normal hearing comparison group subjects constituted group A (n=30 subjects). Fifty percent of clinical group subjects constituted group B (n=15 subjects), 16.3% constituted group C (n=5 subjects) and remaining 33.33% belonged to group D (n=10 subjects).Audiological assessment consisted of puretone audiometry including high frequency audiometry, speech audiometry-Speech Reception Threshold (SRT) and Speech Discrimination Score (SDS), immittance audiometry (tympanometry, acoustic reflex threshold-ART) and DPOAE. Grason Stadler Incorporates (GSI) - 61 clinical audiometer, GSI-TympStar immittance audiometer and GSI- Audera equipment were employed for the study.The thresholds were obtained using puretone at frequencies 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz, 6000 Hz, 8000 Hz and also extended high frequencies such as 10 kilo Hertz (kHz), 12.5 kHz, 16 kHz and 20 kHz using modified Hughson and Westlake procedure [5]. All these measurements were carried out in a sound treated room with ambient noise levels within the permissible limit as recommended by American National Standards Institute [6]. Calibrated two channel diagnostic audiometer GSI-61 with circumaural earphones was used for extended high frequency audiometry. SRT and SDS were obtained using standard measures.Tympanogram type, ipsilateral and contralateral ARTs were obtained. The values obtained on acoustic reflex test were expressed in terms of sensation level (SL) of ART which refers to the number of decibels of ART above the listener’s hearing threshold. The signal to noise ratio (SNR) of DPOAEs were obtained for comparison and clinical groups for the frequencies 598 Hz, 691 Hz, 785 Hz, 902 Hz, 1031 Hz, 1184 Hz, 1371 Hz, 1594 Hz, 1816 Hz, 2098 Hz, 2402 Hz, 2754 Hz, 3152 Hz, 3621 Hz, 4184 Hz, 4816 Hz, 5496 Hz, 6340 Hz and 7277 Hz. Stimuli consisted of series of two puretones at two frequencies (that is f1, f2 [f2>f1]) and two intensity levels (that is L1, L2). A ratio of 1.22 between f1 and f2 was used to elicit DPOAE. The intensity level of f1 and f2 were 65 decibel (dB) Sound Pressure Level (SPL) (L1) and 55 dB SPL (L2) respectively.Statistical comparisons of audiological data were made with respect to clinical versus comparison group, between right and left ear in the clinical group and based on duration of mobile phone usage. To compare the results of clinical versus comparison group and between right and left ear in the clinical group, independent t test was used. For the comparison among sub-groups based on duration of mobile phone usage, one way Analysis of Variance (ANOVA) and Post hoc multiple analysis test was used. Acoustic reflexometric results were not considered for comparison among sub-groups based on duration of mobile phone usage.
3. Results
3.1. Puretone and Speech Audiometry
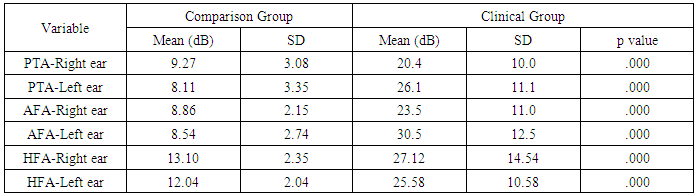
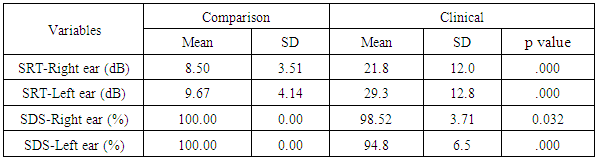
- The PTA of three frequencies viz., 500 Hz, 1 kHz and 2 kHz tested by air conduction, AFA - puretone average of all frequencies viz., 250 Hz, 500 Hz, 1 kHz, 2 kHz, 4 kHz, 6 kHz, 8 kHz, 10 kHz, 12.5 kHz, 16 kHz and 20 kHz tested by air conduction and HFA-puretone average of frequencies viz., 4 kHz, 6 kHz, 8 kHz, 10 kHz, 12.5 kHz, 16 kHz and 20 kHz tested by air conduction were computed for 30 right ears and 30 left ears separately in the comparison group. The PTA, AFA and HFA were computed in clinical group also. The mean differences in PTA, AFA and HFA between clinical and comparison groups were found to be statistically significant (p<0.05) using independent t-test (Table 1).
|
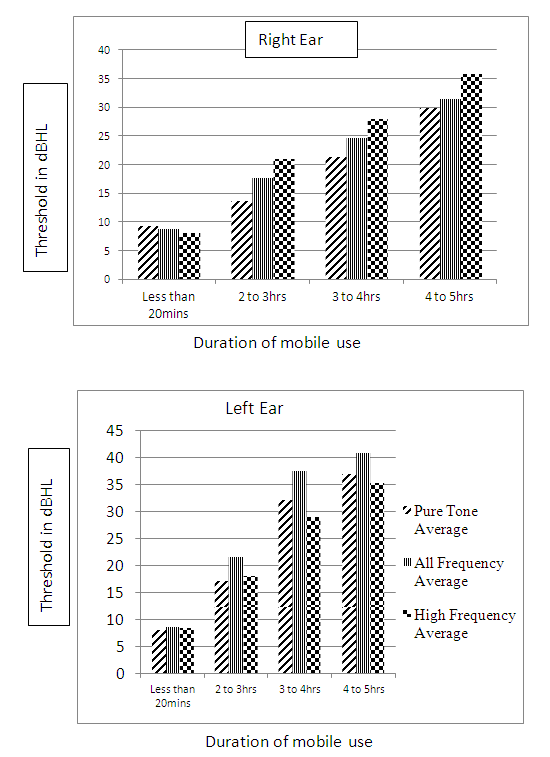 | Figure 1. Comparison of duration of mobile phone usage and mean PTA, AFA and HFA in right and left ears |
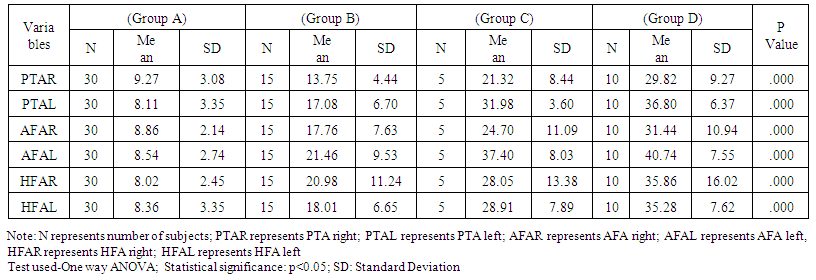 | Table 2. Comparison of PTA, AFA and HFA between Subgroups Based on the Extent of Mobile Phone Usage |
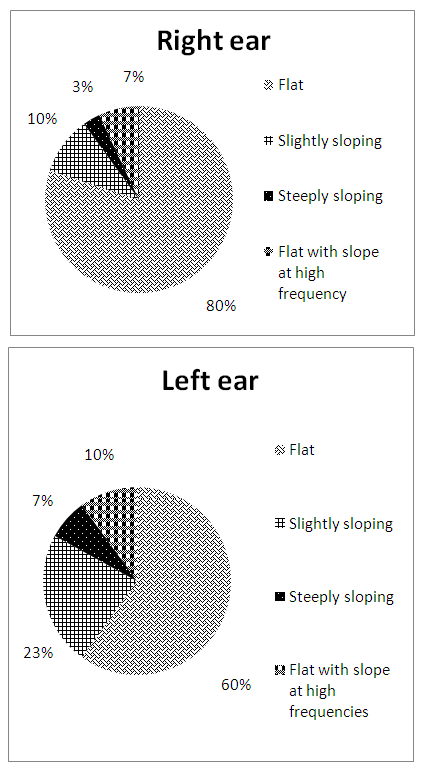 | Figure 2. Audiogram configurations in right and left ear |
|
|
3.2. Acoustic Reflex Threshold (ART)
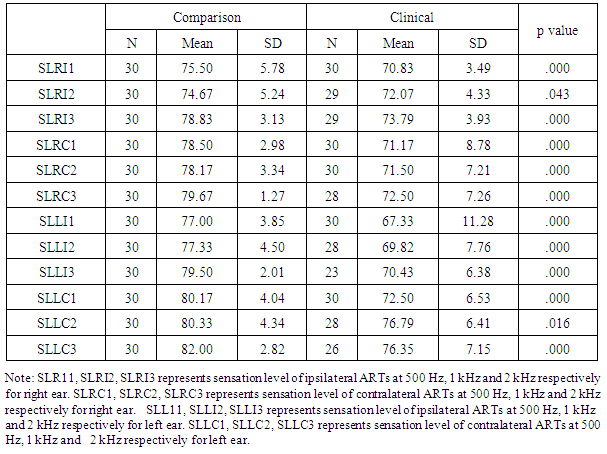
- Independent t test was utilized to analyze the difference between the means of ART (SL) values obtained on ipsilateral and contralateral stimulation for the comparison group and the clinical group and it was found to be statistically significant at p<0.005 (Table 5) with better scores in clinical group.
|
3.3. Distortion Product Otoacoustic Emissions (DPOAE)
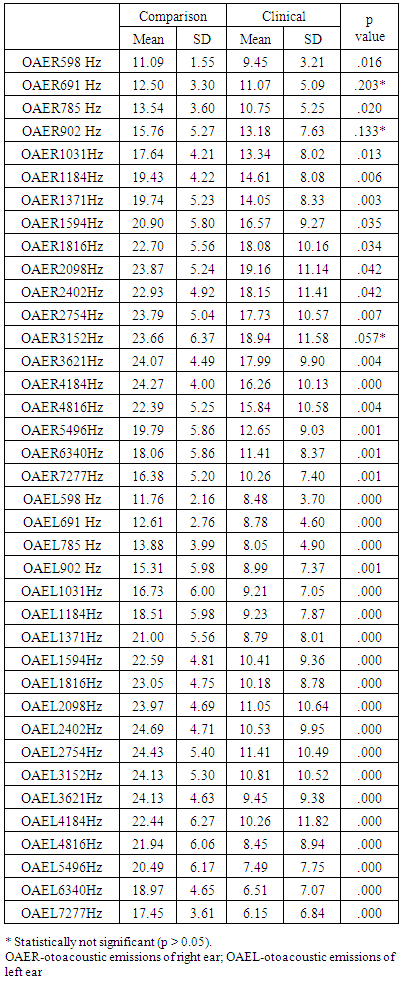
- The mean difference in signal to noise ratio (SNR) of DPOAE between comparison group and clinical group were analyzed by using independent t test. The mean difference was found to be statistically significant at majority of test frequencies (p<0.05) (Table 6). The DPOAE SNR values were also compared between right and left ears in the clinical group and found to be significantly different at majority of test frequencies (p<0.05) with poor scores in left ear.
|
4. Discussion
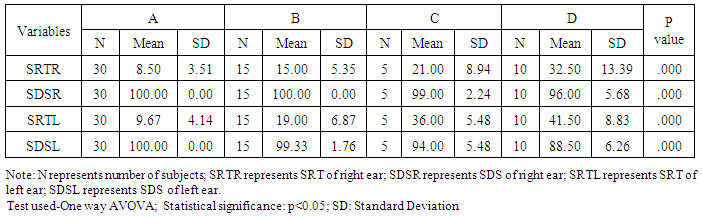
- Flat type of audiogram was observed in more subjects in the clinical group (80% in right ear and 60% in left ear). Approximately 56% of them with flat configuration had normal hearing sensitivity and 43% had mild hearing impairment. In the present study, the puretone hearing sensitivity was poor in clinical group as evidenced by PTA, AFA and HFA indices. Similar findings, especially poor high frequency hearing in mobile phone users have been reported by Prajapati et al [7]. This could probably be attributed to the thermal and non-thermal effects of mobile phone use. Approximately 47% of subjects under clinical group of this study were using mobile phones in their left ear. Thirty percent of subjects were using mobile phones in right ear and 23% had no ear preference. Hearing loss was more marked in left ear as compared to right ear (evidenced by PTA and AFA). Similar findings were reported by Velayutham et al [8]. In their study, the left ear was preferred for phone use by 63% of subjects, 22% preferred right ear and 15% had no preference. Their study showed that high frequency hearing loss was more evident in the predominantly mobile phone used ear when compared to the other ear. Prajapati et al [7] have also reported similar findings. Similarly, a study done by Kerekhanjanarong et al [9] reported that the hearing threshold of the dominant mobile phone used ears was worse than the non-dominant ears based on assessment of eight subjects who used phone more than 60 minutes per day. Hence, with prolonged mobile phone use, ear differences tend to arise in terms of auditory function. PTA, AFA and HFA were compared between the subgroups. The puretone thresholds were better in group A and poorer in group D. Group C thresholds were better than group D and poorer than group B. Group B thresholds were poorer than group A thresholds. All these values exhibited statistically significant difference among them. Hence, it was evident that hearing sensitivity deteriorates with long-term mobile phone use. These findings were in agreement with a study by Oktay and Dasdag [10] who reported that individuals with approximately two hours per day of mobile phone use had higher thresholds than moderate users (10-20 minutes/day) or control group (no mobile phone use). The SRT was poorer in clinical group. This could be attributed to poor puretone hearing sensitivity. SDS was also poor in clinical group. Similar findings were reported by Panda et al [3]. They conducted study on 125 long-term mobile phone users and reported higher speech frequency thresholds when compared with control group. Similar to puretone audiometric findings, dominant mobile phone used ear (left ear) showed poor performance on speech audiometric tests when compared with non-dominant ear (right ear) indicating possible influence of mobile phone use in left ear. The mean difference of SRT and SDS between the subgroups (A, B, C and D) was found to be significant with Group D having worst scores. This could be attributed to the fact that increase in exposure to mobile phones can cause worsening of puretone hearing sensitivity along with reduction in speech reception and discrimination scores.Comparison of ART (SL) values between comparison group and clinical group for ipsilateral and contralateral stimulation revealed significant difference with clinical group having better scores. This could be an indication of a trend towards probable cochlear involvement in clinical group as revealed by early acoustic reflexes than comparison group. The Signal to Noise Ratio (SNR) of DPOAE was significantly poorer in clinical group compared to comparison group. Similar findings have been reported by Panda et al [3]. The inner ear is in the closest proximity to the mobile phone during use which may lead to impaired cochlear outer hair cell function. Similar to puretone and speech audiometric findings, DPOAE amplitudes were significantly poorer in the dominant mobile phone used ear, i.e., left ear when compared with right ear, providing probable evidence regarding impact of mobile phone use on cochlear outer hair cells.The mean differences of amplitude of DPOAE between the subgroups (A, B, C and D) were statistically significant. The DPOAEs in groups B, C and D were reduced. Hence, the amplitude of DPOAE seems to decrease with increase in duration of mobile phone use. Panda et al [4] observed high-frequency loss and absent DPOAEs with an increase in the duration of mobile phone use in 112 subjects (long-term mobile phone users for more than one year). Hence, cochlear outer hair cell function seems to get impaired with long-term mobile phone use.The study has some limitations: More number of subjects could have been included for proper validation. Comparison of clinical group would have been ideally done with non-mobile phone users.
5. Conclusions
- This study aimed to characterize audiological profile of individuals who used mobile phones extensively and to correlate audiological test results with duration of mobile phone use. The results indicated that auditory function is significantly impaired in the clinical group as evidenced by findings obtained in puretone, speech and immittance audiometry as well as DPOAE. Further, the impact on dominant mobile phone used ear was clearly evident. Undoubtedly, the audiological test results were comparatively poorer in long duration users when compared to short duration users of mobile phone. Hence, based on the study, it is recommended to use mobile phones very judiciously. It should be used only for essential purposes. The devices should have low Specific Absorption Rate (SAR) values and preferably with hands-free accessories. Wherever possible, loudspeaker option should be utilized in mobile phone. The knowledge on adverse effects of mobile phones on hearing is important to spread awareness among people. Further, large sample size studies on impact of mobile phone use on central auditory processing is recommended to strengthen our knowledge on deleterious effects of long term and intensive mobile phone use on hearing.