-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2015; 4(3): 38-39
doi:10.5923/j.otolaryn.20150403.02
Pilonidal Sinus of External Auditory Canal: A Rare Entity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBorlingegowda Viswanatha, Mylanahalli Doddarangaiah Prakash, Maliyappanahalli Siddappa Vijayashree, Ravikumar Rasika, Gopinathan Sangeetha
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
A 10year old boy presented with features of chronic otitis media of right ear with a red polypoidal mass in the right external auditory canal and with history of bleeding from the same ear. On examination a reddish polypoidal mass was seen arising from the antero-superior quadrant of external auditory canal near the bony-cartilaginous junction and filling the external auditory canal. CT scan showed a soft tissue mass filling the right external auditory canal suggestive of aural polyp. Under General Anaesthesia, the mass was found to be arising from antero-superior quadrant of external auditory canal and on removal of the mass normal tympanic membrane was seen. Histopathological examination of the specimen showed features suggestive of pilonidal sinus.
Keywords: Pilonidal sinus, External auditory canal
Cite this paper: Borlingegowda Viswanatha, Mylanahalli Doddarangaiah Prakash, Maliyappanahalli Siddappa Vijayashree, Ravikumar Rasika, Gopinathan Sangeetha, Pilonidal Sinus of External Auditory Canal: A Rare Entity, Research in Otolaryngology, Vol. 4 No. 3, 2015, pp. 38-39. doi: 10.5923/j.otolaryn.20150403.02.
1. Introduction
- A Pilonidal sinus (Latin for 'nest of hair') is an abnormal epithelium-lined tract filled with hair that opens to the skin surface, most commonly in the natal cleft. It is proposed to be caused by shed or sheared hairs penetrating the skin and inciting an inflammatory reaction and sinus development, with intermittent negative pressure drawing in more hair and perpetuating the cycle. Common annual incidence is 26 per 100,000, with male predilection and mean age of presentation is 20 years. [1] The phrase 'pilonidal' was first used by R M Hodges in 1880 [2]. Even though it is most common in the sacrococcygeal area some rare sites has been reported like inter digital area, abdomen, scalp, neck, penis, groin, axilla and external ear [3].
2. Case Report
- A 10 year old boy presented with complaints of right ear discharge since 2 months. Initially the discharge was purulent and scanty and 1 week after the onset it became blood stained and foul smelling. It was associated with decreased hearing which started 1 month after the onset of discharge. The hearing loss was gradual in onset and progressive in nature. The patient did not have similar complaints in the past.On examination, after clearing the blood stained foul smelling discharge off the right external auditory canal, a reddish polypoidal mass was seen arising from the antero-superior quadrant of external auditory canal near the bony-cartilaginous junction and filling the external auditory canal. The mass was freely probed posteriorly and inferiorly, was soft in consistency, sensitive to touch and bled on touch. Tuning fork tests showed mild conductive hearing loss. Pure tone audiometry reported conductive hearing loss of 30 decibels. CT scan showed a soft tissue mass arising from the antero-superior quadrant of external auditory canal extending upto the tympanic membrane, with intact tympanic membrane and middle ear suggestive of aural polyp [Figure 1].
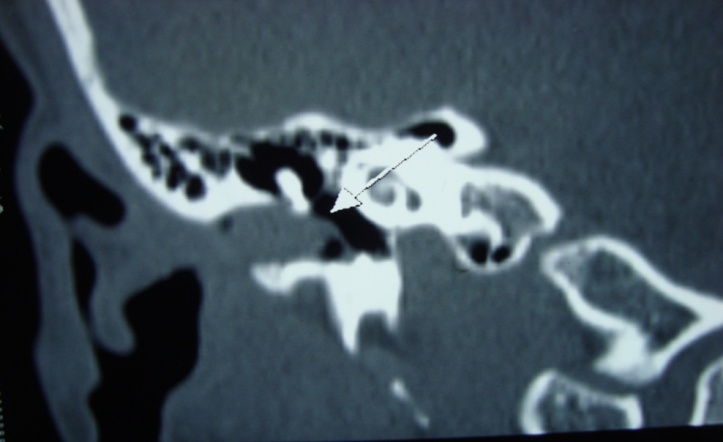 | Figure 1. CT scan picture of temporal bone coronal section showing a soft tissue mass (white arrow) in the external auditory canal with intact tympanic membrane and middle ear |
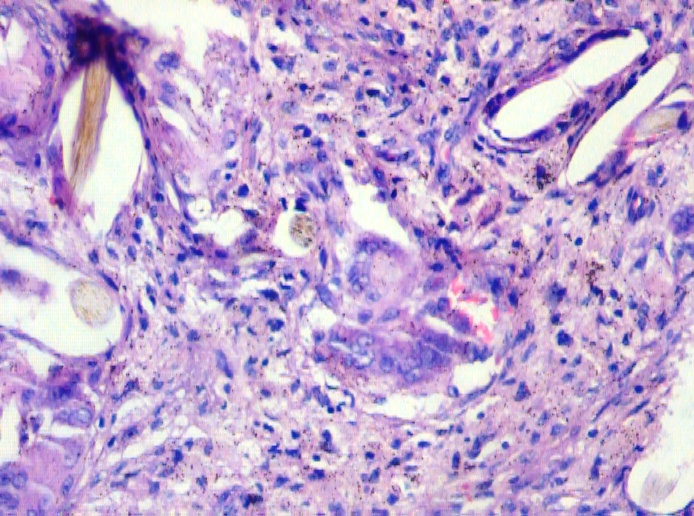 | Figure 2. Microphotograph showing hair shaft (black arrow), keratin debris and cholesterol granuloma with surrounding inflammatory cells and granulation tissue |
3. Discussion
- A pilonidal sinus arises from chronic inflammation and pressure involving a hair-bearing region. A tract develops connecting the skin surface with collection of hairs, cell debris and keratinizing epithelial tissue. It is more common in the sacrococcygeal area because the pre-requisites of hair-bearing skin, maceration and pressure are most readily found [4]. It is otherwise known as JEEP BOTTOM or JEEP RIDERS DISEASE because of its widespread prevalence among soldier's of Second World War who had to travel long journeys in war jeeps [1]. A variant of pilonidal sinus is the digital sinus of the barber or animal trimmer where foreign hairs are driven into interdigital web space, stimulating a granulomatous response [4]. Rarely squamous cell carcinoma can arise from a chronic pilonidal sinus. [5, 6, 7]In many instances, a pilonidal sinus is asymptomatic. A secondary infection with pain, swelling, erythema and drainage of pus is the most common cause for seeking medical advice. Clinically it can be diagnosed by its typical location, appearance and on probing through one of the tracts pus will be drained out [8]. The main finding in histopathological examination is fibrosis and often granulomatous inflammation. Keratinizing epithelial wall, hairs and perhaps a duct or sinus opening into the skin surface may be visualised [4]. Treatment is surgical. Patients with mild-moderate disease can be managed by simple techniques like Bascom 1 procedure, done under sedation and local anaesthesia as a day care procedure, followed by patient’s self care post operatively. It has little morbidity as non surgical treatment. Other procedures include Munro Z-plasty, Karydakis procedure and its Kitchen and Bascom 2 modifications and En bloc excision of cyst. [1, 9]
4. Conclusions
- Pilonidal sinus of external auditory canal is a rarest entity. To the best of our knowledge only one case of pilonidal sinus in the ear has been reported so far, which was arising from ear lobule and just behind the tragus. This is the first case to be reported in the deeper part of external auditory canal.