-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2015; 4(2): 29-33
doi:10.5923/j.otolaryn.20150402.03
Tracheostomy: Our Experience
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLR. K. Datta, B. Viswanatha, P. J. Puneet, Merin Bobby, T. L. N. Kumari
ENT department, Bangalore medical college & research institute, Bangalore, India
Correspondence to: B. Viswanatha, ENT department, Bangalore medical college & research institute, Bangalore, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Tracheostomy remains a very important lifesaving surgical procedure worldwide and particularly in developing countries where patients present late in upper airway obstruction. The aim of this study is to describe our own experiences with tracheostomy, outlining the common indications and outcome of tracheostomized patients in our setting. Fifty consecutive cases comprising of varying age groups with different indications were included in this study. The data of operated patients were collected and analysed.
Keywords: Tracheostomy, Airway obstruction
Cite this paper: R. K. Datta, B. Viswanatha, P. J. Puneet, Merin Bobby, T. L. N. Kumari, Tracheostomy: Our Experience, Research in Otolaryngology, Vol. 4 No. 2, 2015, pp. 29-33. doi: 10.5923/j.otolaryn.20150402.03.
1. Introduction
- Tracheostomy is a lifesaving procedure which has stood the test of time [1]. Before the birth of Christ, until the early part of the nineteenth century, the procedure was considered hazardous and was rarely performed [2, 3]. Only during past three decades, the operation has assumed its rightful place as a safe, simple procedure with wide range of usefulness. Today the tracheostomy has extended the collaboration of otolaryngologists with all phases of medicine and Surgery [3]. In recent years there has been a considerable shift in emphasis regarding the indications for tracheostomy with recognition of the more physiologic and functional indications in addition to those of a strictly obstructive nature. Tracheostomy is being performed with ease, with better knowledge of anatomy and by adopting the classical technique advocated by Jackson during the early years after 1900 [1].In the modern era of the operation, Jackson and others have stressed the importance of a clear airway following tracheostomy, and have recognized that the tracheostomy is not the objective in treatment, but only aims at securing proper ventilation [4]. During recent years, the complications and deaths due to trancheostomy are reduced because of refinement of techniques and better post-operative care. But still the problems like difficult decannulation are not solved.Tracheostomy may be elective or emergency. In the former there is enough time for preparation and done in a well planned way under ideal operating conditions. Tracheostomy may be either temporary or permanent.The purpose of this study is,Ø To study the evolution and different aspects of tracheostomy, a valuable procedure with a wide range of applicability and usefulness in many fields of medicine and surgery. Ø To present an analysis of indications, symptoms, technique, management and complications encountered in tracheostomized patients.Tracheostomy is an incision into the trachea (windpipe) to form a temporary or permanent opening. The opening or hole is called stoma [5, 6].§ Sometimes the terms tracheotomy and tracheostomy are used interchangeably.§ The tracheal opening is made either in the second, third, fourth or fifth tracheal ring and a tube is inserted through the opening to allow passage of air which also helps in removal of secretions.Role of Tracheostomy:In addition to its role of bypassing an upper airway obstruction, its other functions Include:§ It reduces the amount of dead space in the respiratory tract. The normal tidal volume is about 500 ml; the dead space is about 200ml. Half of this dead space is in the nose, throat and pharynx. The decrease in dead space may vary from 10% to 50% depending upon the individual’s physiological dead space. This apparently small amount of air becomes of crucial importance when the respiratory function is impaired and the tidal volume is reduced [2].§ It reduces the resistance to the airflow as it bypasses an incompetent larynx and pharynx and the effect of glottic narrowing. The working load of respiration is thus reduced. This will result in increased total compliance and more effective alveolar ventilation, provided the tracheostomy stoma is large enough [3, 6].§ It bypasses the pool of saliva in the pharynx and in case of ineffective laryngeal reflexes, a cuffed tube protects the air passage against aspirations.§ Permits deglutition without reflex apnoea which is an important factor in the respiratory disease patient [2].§ Permits removal of crust and secretions blocked airway causes increased capillary permeability, which further increases anoxia. Tracheostomy with aspiration of secretions and exudates promotes ventilation of the lungs [7].§ It provides pathway to deliver medications and humidification to the tracheo bronchial tree.§ It provides simple, convenient and reliable pathway for the administration of artificial respiration as in poliomyelitis, respiratory muscle paralyses, etc with impaired respiratory mechanism till the spontaneous respiration is resumed [6, 7].§ It provides a pathway to deliver medication and humidification to the tracheobronchial tree, with or without intermittent positive pressure breathing.Provides a simple route for administration of anaesthesia. A high flow of oxygen and light planes of anaesthesia are maintained. Patient recovery will be uneventful and will be able to take nourishment almost immediately as the hazards of aspiration are greatly reduced with tracheostomy. This method can be adopted for both initial and follow-up of surgical management of patients with burns, maxillo facial injuries, head injuries, and head and neck tumours.The Advantages of tracheostomy:• Anatomical dead space is reduced by approximately 50% [7].• The work of breathing is reduced.• Instead of breathing through the nose and mouth, the patient now breathes through the tracheostomy tube.• Alveolar ventilation is increased.• Level of sedation needed for patient comfort is decreased.• Patient able to talk and eat with tracheostomy tube in place (unlike in endotracheal intubation).The disadvantages of tracheostomy:• Mainly the normal speech has to be compromised and others like loss of heat & moisture exchange performed in the upper respiratory tract [7, 8].• Desiccation of tracheal epithelium, loss of ciliated cells and metaplasia of squamous epithelium [9].• Presence of foreign body in the trachea stimulates mucous production, where no cilia are present their mucociliary stream is arrested [10, 11].• Mucus causes drying resulting in crust formation and tube block particularly in small calibre tube used in children [8].
2. Materials and Methods
- In this study, 50 cases of tracheostomy were studied. These are consecutive cases comprising of varying age groups with different indications. The data was collected from the patients who had undergone either elective or emergency tracheostomy.Selected patients were subjected to investigations, pre-operatively and post-operatively for: − X-Ray Soft Tissue Neck, lateral view,− X-Ray Chest PA view. − Routine blood and urine investigations.All the selected patients who underwent standard tracheostomy procedure were given intensive care for the first 48 hours post-operatively. Problems encountered during surgery were documented in the operative notes. The immediate post-operative problems were seen in post-operative ward. Intermediate and late post-operative complications were assessed when patient came for regular follow up.Regular follow-up of the patients was done for both elective and emergency tracheostomy. Follow-up was done twice a week for first month. Once a week for second month. Monthly twice in the third month and finally whenever patient has any problems, he/she was asked to come for follow up [10].
3. Results and Discussions
- In a study by Crysdale et.al. [9] in 1976-1985 and Zetonni & Manoukian in 1993, where 319 and 44 cases were taken up respectively. In Crysdale et.al. study, 222 cases (70%) were of airway obstruction, 65 cases (20%) were of tracheobronchial toilet and 32 cases (10%) were of continued assisted ventilation. In Zetonni & Manoukian, 25 cases (57%) were of airway obstruction.In the present study 50 patients who underwent tracheostomy in two years period. In this group 44 cases (88%) were of airway obstruction, 5 cases (10%) were of laryngeal trauma and 1 Case was (2%) of Gillian Barrie syndrome [G.B. Syndrome]. The study also revealed the age incidence varying from 5 years to 75 years. In this study there were 40 males (80%) and 10 females (20%), with a ratio of 4:1 [figure.1].
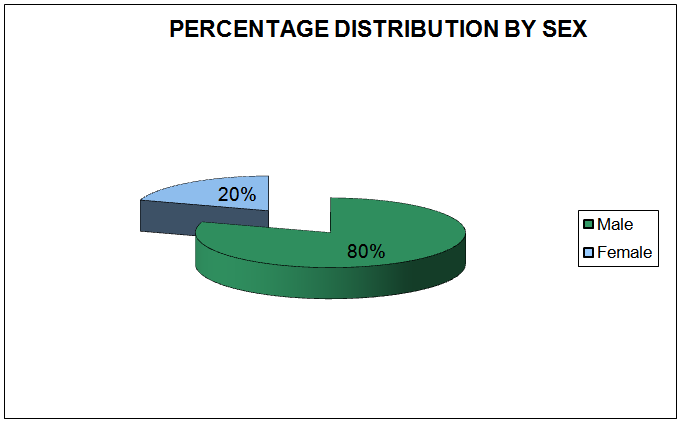 | Figure 1. Showing gender distribution of patients |
|
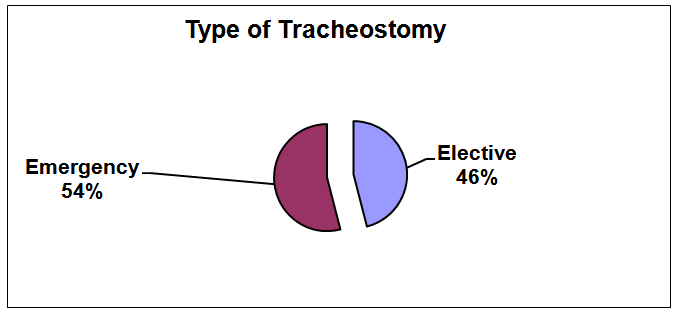 | Figure 2. Showing types of tracheostomy |
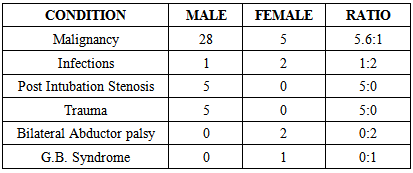
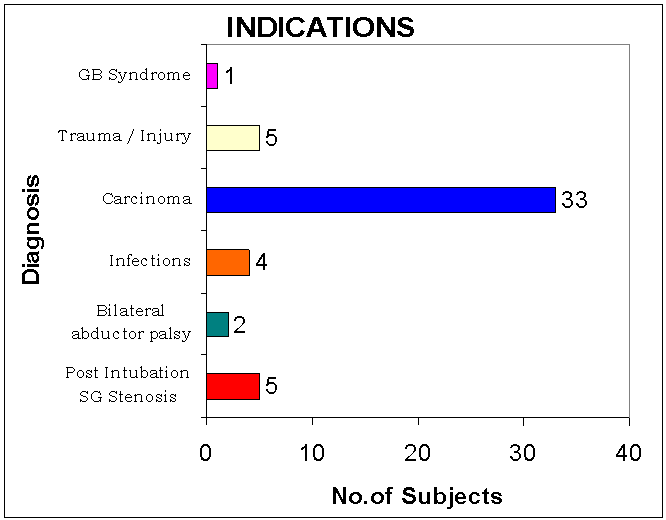 | Figure 3. Showing indications for tracheostomy |
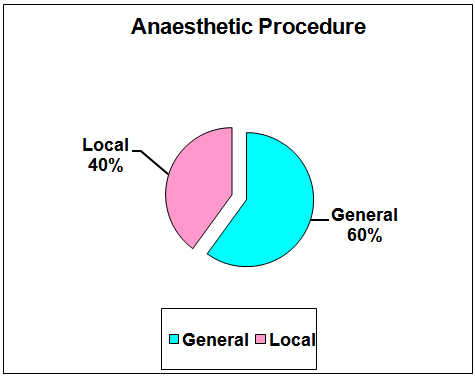 | Figure 4. Showing types of anaesthesia used for tracheostomy |
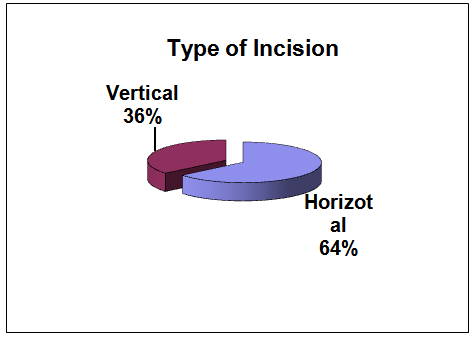 | Figure 5. Showing type of incision used for tracheostomy |
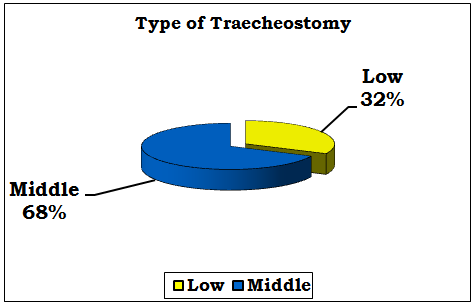 | Figure 6. Showing type of tracheostomy |
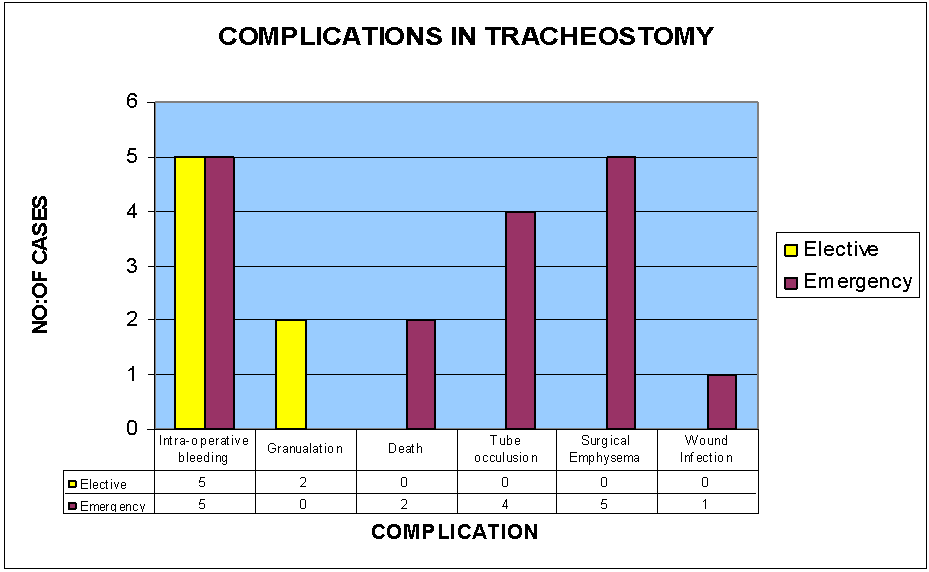 | Figure 7. Showing complications of tracheostomy |
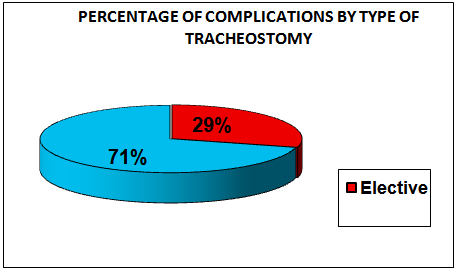 | Figure 8. Showing percentage of complications of tracheostomy |
4. Conclusions
- This study also confirms the low mortality and morbidity when the best post-operative nursing care is instituted. This is evidenced by low post operative morbidity in present study, which again emphasizes the need for meticulous post-operative tracheostomy care. Finally even today tracheostomy remains as a life saving procedure.