-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(6): 89-91
doi:10.5923/j.otolaryn.20140306.02
An Interesting Case of Button Battery Causing Septal Perforation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJapneet Kaur, Rasika Ravikumar, Borligegowda Viswanatha, Maliyappanahalli Siddappa Vijayashree
Otorhinolaryngology department, Bangalore medical college & Research institute, Bangalore, India
Correspondence to: Borligegowda Viswanatha, Otorhinolaryngology department, Bangalore medical college & Research institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Button batteries presenting as foreign bodies in the nasal cavity are rarely seen but common in paediatric age group. They are hazardous due to the extensive nature of damage caused by them. In this article we discuss the case of a child with impacted button battery in the nasal cavity. A 5 year old boy presented with bilateral foul smelling nasal discharge since 3 weeks. It was purulent, yellowish green, non blood stained. The child also complained of bifrontal headache which was dull aching in nature. Radiograph showed evidence of a button battery in the left nostril. The foreign body was removed endoscopically and it was found that there was a perforation in the nasal septum. Early recognition and management is the key to prevention of complications due to foreign bodies.
Keywords: Foreign body nose, Button battery, Septal perforation
Cite this paper: Japneet Kaur, Rasika Ravikumar, Borligegowda Viswanatha, Maliyappanahalli Siddappa Vijayashree, An Interesting Case of Button Battery Causing Septal Perforation, Research in Otolaryngology, Vol. 3 No. 6, 2014, pp. 89-91. doi: 10.5923/j.otolaryn.20140306.02.
1. Introduction
- Button batteries are increasingly being used in many electrical devices like toys, watches, calculators etc. They are composed of alkaline contents. Due to their small size, these batteries can be very easily inserted by small children in the nose. Button battery found as a foreign body in the nasal cavity is rare and it is most commonly discovered in children between the ages of 2 to 5 years [1]. A nasal button battery is an otorhinolaryngological emergency. Button batteries can lead to severe damage, necrosis, and perforation of the nasal septum, intranasal synechiae, and nasal deformity [2]. Button batteries should ideally be removed by an otorhinolaryngologist in a controlled setting under general anaesthesia if they cannot be removed in the outpatient department.We hereby report this case to advocate that button battery in the nasal cavity is a serious condition and early diagnosis and management is the key to prevention of grave complications like septal perforation , nasal synechiae etc.
2. Case Report
- 5 year old child presented to our Otorhinolaryngology department with foul smelling bilateral nasal discharge since 3weeks. Discharge was purulent, yellowish and non blood stained. The child also complained of bifrontal headache which was dull aching in nature and suggestive of rhinosinusitis. On anterior rhinoscopy examination there was yellowish green mucopurulent foul smelling discharge seen in both the nasal cavities. Radiograph of nose and paranasal sinuses (Water’s view and lateral view) showed a small round metallic object in the left nostril (figure-1) and there were features suggestive of bilateral maxillary sinusitis. X-ray lateral view of nasal cavity was taken to know its position in the nasal cavity [figure-2].
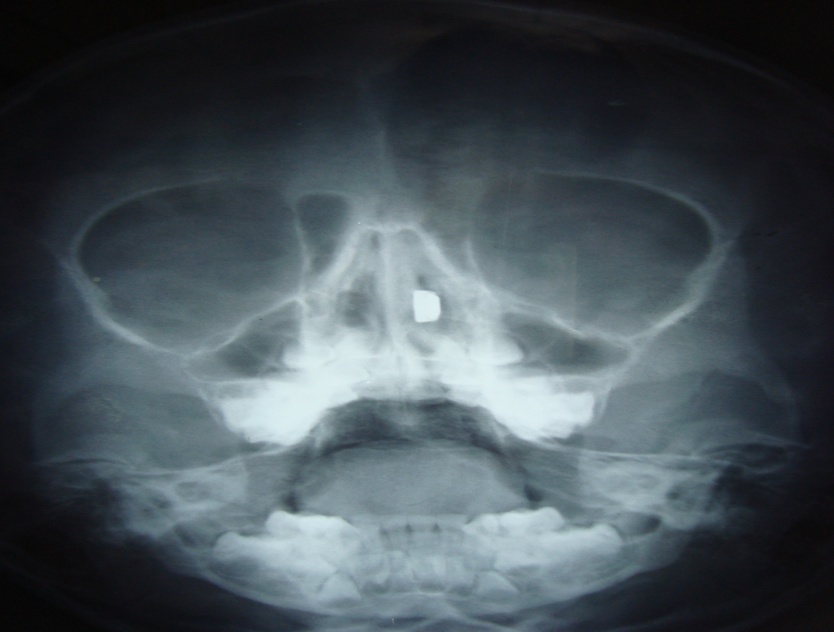 | Figure 1. X-ray paranasal sinuses showing button battery in the left nasal cavity |
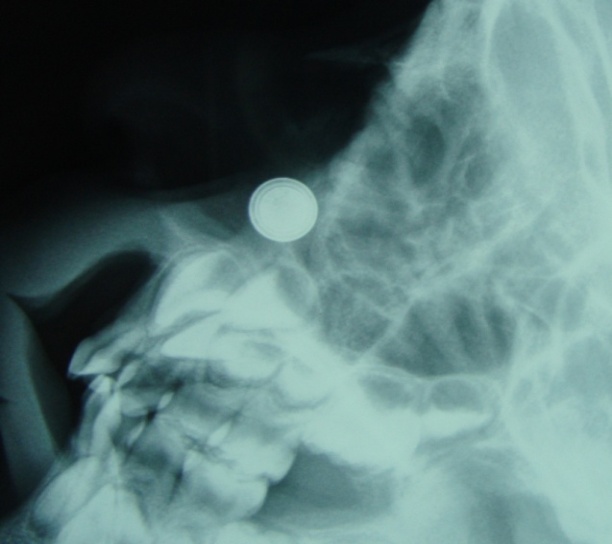 | Figure 2. X-ray nose lateral view showing radio opaque round button battery |
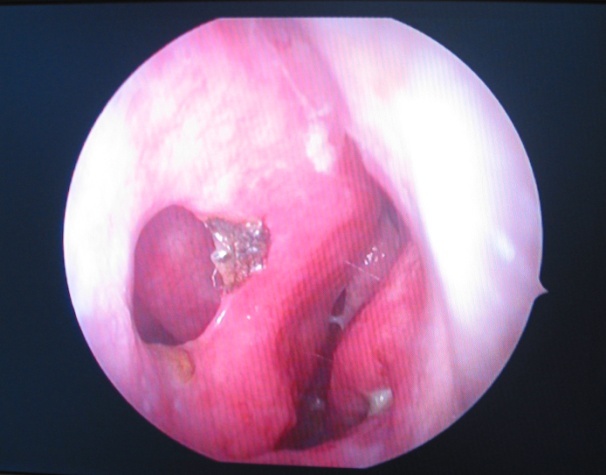 | Figure 3. Endoscopic view of left nasal cavity showing septal perforation |
3. Discussion
- The impact of button battery depends on the duration it remains in situ, the site at which the battery is lodged, size of the battery, its power, its age (whether new or old, as older batteries cause lesser damage due to diminished contents), and the possibility of heavy-metal absorption [3].Increase in the duration between insertion of button battery in the nose and removal can lead to devastating complications like septal perforation, necrosis of nasal mucosa, nasal synechiae etc . Most common site of leakage from the button battery is the seal [4].In our case the button battery had eroded and the chemicals released in turn eroded the nasal septum leading to septal perforation because of which the patient had bilateral foul smelling nasal discharge.It is important to differentiate button cells from coins as the latter are considered benign and may be responsible for unnecessary delay in the management of impacted batteries [5]. Impacted button batteries are an emergency and should be handled at the earliest. Button batteries can be easily visualised in the plain X-ray lateral view of nose as radio opaque round objects.Button cells have a characteristic appearance on radiography: they have a bilaminar structure; so they appear as a double ring or halo (double density) on anteroposterior view and a step-off at the separation between the anode and cathode on lateral view [6-8]. Small button batteries may be difficult to differentiate from buttons or coins. However in case of long standing impacted batteries presenting with nasal discharge and suspicion of septal perforation, diagnostic nasal endoscopy should be done to visualise the site of perforation and the impacted battery. The most significant mechanism is the generation of hydroxide ions at the negative pole of the battery caused by the current created through the adjacent tissue. Human tissue basically acts to ‘connect the circuit’ around the two poles of the battery. Anode pole is associated with more damage. Due to erosion of the battery, alkaline fluids are released from the battery which leads to liquefactive necrosis and erosion of the nasal mucosa which in our case had led to nasal septal perforation. A tissue pH of >10 can occur rapidly, driven by the voltage of the battery, but this is a powered alkaline burn. The higher the voltage, the faster this process occurs [1].The amount of nasal secretion and size of nose are also important factors deciding the extent of damage [9]. Button batteries can cause damage by the following ways [4, 10]:a. Electrical burns due to generation of electric current b. Chemical burns due to leakage of alkaline contentsc. Toxicity due to absorption of chemical contentsd. Liquefactive necrosis due to leakage of alkaline contents e. Pressure necrosis due to impacted foreign bodyImpaction of nasal button battery can lead to mucosal, turbinate and nasal septal ulceration in 3-6 hours. Inferior turbinate necrosis has occurred in 24 hours [11].After identifying the foreign body it should be removed immediately in outpatient/ emergency department. If removal is not possible in the outpatient department as children can be uncooperative, it should be removed under general anaesthesia.In case of anteriorly impacted foreign bodies, apart from manual removal, positive pressure techniques like an ambu bag can be employed. Botma et al have described a technique called “parent kiss”. Mainly used for very small children, in this manoeuvre the care giver mostly the parent blows into the open mouth of the child while occluding the contralateral nostril. This technique is quite effective and less traumatic to the child [4, 12].After removal of the impacted button battery copious irrigation with saline solution should be done in order to remove any alkaline precipitates leaked out of the battery [13]. Intranasal stents can be placed to prevent adhesion and synechaie formation due to severe necrosis. Differential diagnosis of unilateral periorbital pain, headache, swelling over the nose should always include an impacted foreign body in the nose including a button battery [5].Regular follow up is essential to assess any long term complications like septal perforation, nasal synechiae, mucosal ulceration and necrosis etc.Since this condition is more common in children, parents should be educated about its potential hazards. Devices using such batteries should be kept out of reach from small children.
4. Conclusions
- Button battery in the nasal cavity is a hazardous condition as it can cause extensive tissue damage and complications. Thus any patient with button battery in nose needs immediate medical attention. Detailed history and examination should be done, followed by radiological investigations in case of posteriorly located objects.