-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(6): 85-88
doi:10.5923/j.otolaryn.20140306.01
Keratinizing Dentigerous Cyst: A Case Report and Review of Literature
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSuvarna Gowda1, Borligegowda Viswanatha2, Pramod Junjanna1
1Moksha dental clinic, Bangalore, India
2Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India
Correspondence to: Suvarna Gowda, Moksha dental clinic, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
A fifty five year old female patient presented to us with history of right sided cheek swelling since six months. Computerised tomography scan showed a well defined cystic lesion within the right maxillary sinus measuring approximately 2x3 cm, pushing the medial and anterolateral walls into right nasal cavity and cheek respectively. A diagnosis of dentigerous cyst was arrived at and patient advised surgery. But patient refused to undergo surgery. One month later, she presented to us again, but this time she had additional symptoms of pain in the swelling, foul smelling nasal discharge, white masses falling from the right side of nose and facial pain. Repeat CT scan showed a well defined heterogeneous noncontrast enhancing cystic mass (4x3 cm) involving the right maxillary sinus and rupturing into the right nasal cavity eroding the medial wall of maxilla. She underwent enucleation and complete clearance of the cyst under general anaesthesia by Caldwell-Luc’s approach. Histopathological examination of the debris proved the presence of keratin.Keratinizing dentigerous cyst which, to the best of our knowledge, has been reported only twice in the literature in 1971 and 2014. This is the third case of Keratinizing dentigerous cyst to be reported in world literature and the first of its kind arising from a supernumerary tooth.
Keywords: Keratinizing, Dentigerous Cyst
Cite this paper: Suvarna Gowda, Borligegowda Viswanatha, Pramod Junjanna, Keratinizing Dentigerous Cyst: A Case Report and Review of Literature, Research in Otolaryngology, Vol. 3 No. 6, 2014, pp. 85-88. doi: 10.5923/j.otolaryn.20140306.01.
1. Introduction
- Odontogenic cysts were first described by Gorlin and co-workers in 1962. The dentigerous cyst (Latin: Dens = tooth, gerere = to bear) is the second most common odontogenic cyst of epithelial origin accounting for 15% of all true cysts in the jaw. Also known as follicular cyst, a dentigerous cyst develops when a follicle is separated from the crown of a developing tooth. As a result of this, fluid accumulates between the reduced enamel epithelium and tooth crown forming a cystic cavity that surrounds the crown of an unerupted tooth on the cementoenamel junction [1-4]. It occurs most commonly in the mandible (70%). Maxilla is involved only in 30% of the cases [3]. The sites of involvement in decreasing order are the mandibular third molars, maxillary canines and mandibular premolars followed by supernumerary teeth and central incisors [5]. Dentigerous cyst around supernumerary teeth accounts for 5% of all dentigerous cysts and mostly involves a mesiodens in the anterior maxilla [4]. We report an unusual histological variant of odontogenic cyst, the Keratinizing dentigerous cyst arising from supernumerary teeth in a 55 year old female who refused treatment on her first visit and came back to us a month later with a more progressive disease.
2. Case Report
- A 55 year old female presented to us with history of right sided cheek swelling since 6 months [figure-1]. The swelling was insidious in onset and gradually progressive causing facial asymmetry. It was not associated with pain, nasal mass, nasal discharge, headache or palatal swelling. On examination, there was a swelling over anterolateral wall of maxilla which was bony hard in consistency, non tender and not yielding on pressure.
 | Figure 1. Photograph showing swelling in the right cheek |
 | Figure 2. Photograph showing the right lateral wall of nose which is pushed medially |
 | Figure 3. X-ray paranasal sinus showing cystic swelling & supernumerary tooth in the right maxillary sinus |
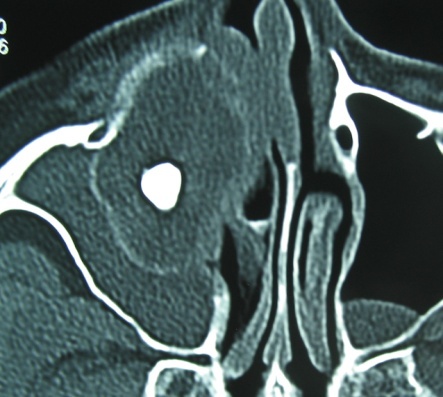
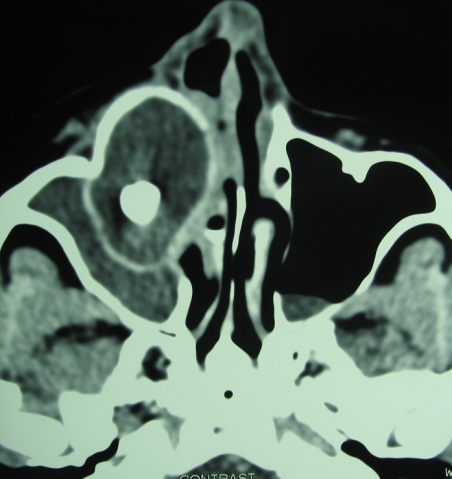 | Figure 4. CT scan showing cystic swelling & supernumerary tooth in the right maxillary sinus |
 | Figure 5. Photograph showing fistulous tract opening above the crown of right 1st molar |
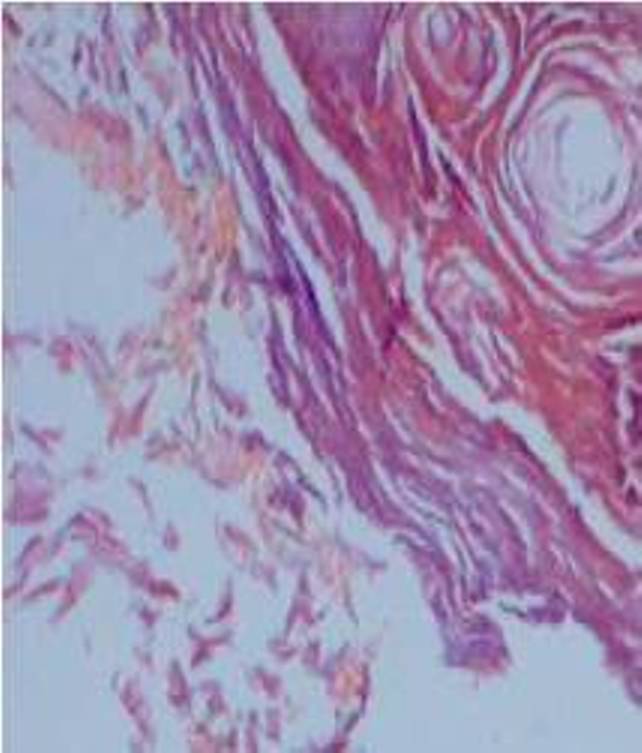 | Figure 6. Microphotograph showing lamellar sheets of keratin |
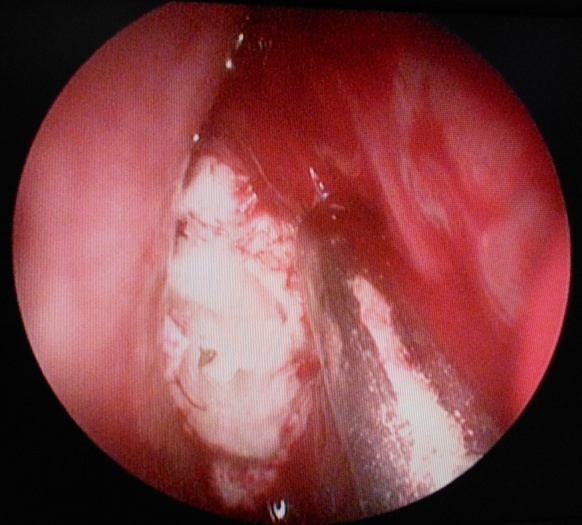 | Figure 7. Diagnostic nasal endoscopy showing whitish mass coming out of the right middle meatus |
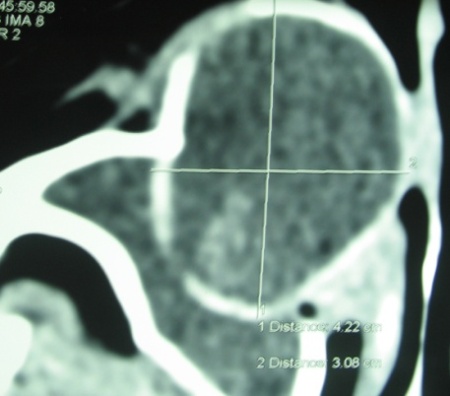 | Figure 8. CT scan showing 4X3 cms cystic swelling in the right maxillary sinus |
 | Figure 9. CT scan showing cystic swelling which has ruptured into the right nasal cavity |
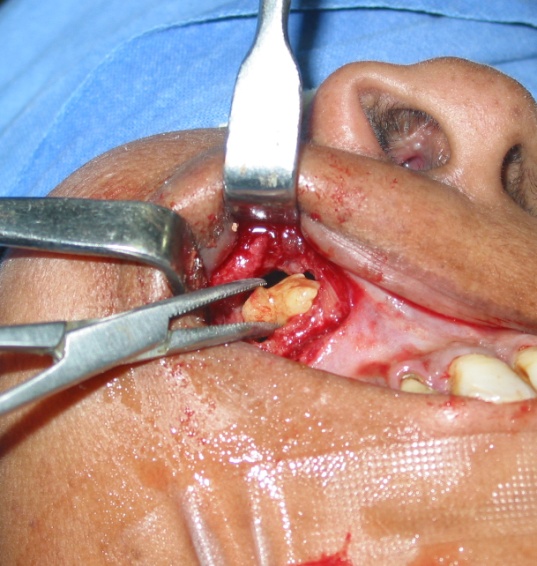 | Figure 10. Intra operative photograph showing teeth inside the cyst removed by Caldwell-Luc approach |
3. Discussion
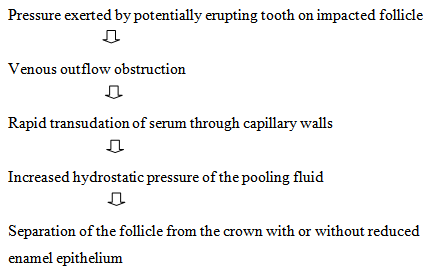
- Odontogenic cyst is most commonly seen between 10 to 30 years of age and may remain asymptomatic throughout life. In such cases it is usually diagnosed incidentally on skull or tooth radiograph. In others, it may present with the classical symptoms of sinus disease [3]. If left untreated, the natural history of the disease is to grow in size with increasing accumulation of fluid. It can destroy the walls of the maxilla in its process and encroach onto the orbits [6]. The cyst may cause pathological fracture or get secondarily infected [2]. Rare incidences of malignant transformation into squamous cell carcinoma, mucoepidermoid carcinoma or an ameloblastoma have also been reported in literature [3]. It is usually associated with the crown of a permanent tooth, deciduous teeth are rarely involved.Gold in 1963 introduced the terms keratinizing and calcifying odontogenic cysts. Dentigerous cyst has been defined as one which is attached at the cement-enamel junction and encloses the crown of an unerupted tooth. Keratinizing dentigerous cyst which, to the best of our knowledge, has been reported only twice in the literature in 1971 and 2014 [7, 8]. This is the third case of Keratinizing dentigerous cyst to be reported in world literature and the first of its kind arising from a supernumerary tooth.Philipsen in 1956 suggested the term Odontogenic Keratocyst (OKC) for all Odontogenic cysts, regardless of type, showing keratinization of the epithelium. More recently, an OKC is defined by other characteristics of the epithelium such as basal palisading, hyperchromatism of nuclei and cell thickness of the epithelium and not merely the presence of keratinization. The term “keratinizing odontogenic cyst” has been suggested for any cyst, regardless of the type, that shows keratinisation [8]. Our patient did not show any evidence of OKC on histopathology. There was no recurrence clinically and radiologically even after 6 months of follow up.The significance of keratinization in odontogenic cysts is not fully known. Keratinization is the final product of epithelial cell differentiation. However, dentigerous cysts, thought to arise from reduced enamel epithelium, are products of end cells, i.e. cells that have completed synthesis (enamel formation). It is possible that the dentigerous cyst is a primordial variant, arising from more primitive cells of the developing enamel organ [8].Pathogenesis of Dentigerous cyst [5]
 Radiographically, it appears as a well-defined unilocular radiolucency with sclerotic margins involving the crown of an unerupted tooth. When infected, the region of cortical bone may be absent. Root resorption and displacement of adjacent teeth are common features associated with this pathology [2]. Dentigerous cysts arising from supernumerary teeth are uncommon and can also arise from an ectopically placed tooth [5].The management depends on the age of the patient, site and extension of the cyst. Various treatment modalities have been proposed. Basic surgical procedure includes marsupialisation or enucleation. The modified procedures include a combination of both, use of Carnoy’s solution following enucleation, and use of bone grafts to fill the cystic cavity. The recurrence rate of dentigerous cyst is very low as when compared to other jaw cysts [1].Cysts that are small and close to osteomeatal complex can be removed endosopically. For all others especially those with lateral and posterior extensions, the best approach is Caldwell-Luc or a combined approach [3]. The large residual bony cavities may be obliterated with bone grafts.Numerous graft materials such as autografts, allogenic, xenografts and platelet rich plasma are available. The surgical defect of the cystic cavity in our case was 4 cm × 3 cm; relying on spontaneous bone regeneration no bone graft was used. The differential diagnosis of dentigerous cyst includes ameloblastoma, odontogenic keratocyst, odontogenic fibroma, odontogenic myxoma, cementomas and Pindborg tumour. Early recognition of the entity and removal is necessary as they may rarely have the potential to develop odontogenic tumours like ameloblastoma and malignancy like squamous cell carcinoma and mucoepidermoid carcinoma [5].
Radiographically, it appears as a well-defined unilocular radiolucency with sclerotic margins involving the crown of an unerupted tooth. When infected, the region of cortical bone may be absent. Root resorption and displacement of adjacent teeth are common features associated with this pathology [2]. Dentigerous cysts arising from supernumerary teeth are uncommon and can also arise from an ectopically placed tooth [5].The management depends on the age of the patient, site and extension of the cyst. Various treatment modalities have been proposed. Basic surgical procedure includes marsupialisation or enucleation. The modified procedures include a combination of both, use of Carnoy’s solution following enucleation, and use of bone grafts to fill the cystic cavity. The recurrence rate of dentigerous cyst is very low as when compared to other jaw cysts [1].Cysts that are small and close to osteomeatal complex can be removed endosopically. For all others especially those with lateral and posterior extensions, the best approach is Caldwell-Luc or a combined approach [3]. The large residual bony cavities may be obliterated with bone grafts.Numerous graft materials such as autografts, allogenic, xenografts and platelet rich plasma are available. The surgical defect of the cystic cavity in our case was 4 cm × 3 cm; relying on spontaneous bone regeneration no bone graft was used. The differential diagnosis of dentigerous cyst includes ameloblastoma, odontogenic keratocyst, odontogenic fibroma, odontogenic myxoma, cementomas and Pindborg tumour. Early recognition of the entity and removal is necessary as they may rarely have the potential to develop odontogenic tumours like ameloblastoma and malignancy like squamous cell carcinoma and mucoepidermoid carcinoma [5]. 4. Conclusions
- Keratinizing dentigerous cyst is an unusual histological variant of odontogenic cyst and very rarely arises from supernumerary tooth. Early recognition and intervention plays a key role in its management due to its malignant potential as does long term follow up for any recurrences. Aesthetic restoration also has to be considered in its management as it involves a prominent part of the face.Keratinizing dentigerous cyst which, to the best of our knowledge, has been reported only twice in the literature in 1971 and 2014. This is the third case of Keratinizing dentigerous cyst to be reported in world literature and the first of its kind arising from a supernumerary tooth.