-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(5): 70-72
doi:10.5923/j.otolaryn.20140305.02
External Ear Canal Osteoma with Canal Cholesteatoma; a Rare Association
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMylanahalli Doddarangaiah Prakash, Borlingegowda Viswanatha, Maruvala Shreeharsha, Sandhya Patil
Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Osteomas of temporal bone are rare, slow growing benign tumours and they are reported in all parts of temporal bone. A complication of ear canal osteoma is ear canal cholesteatoma. A twenty-one year old male patient presented with history of right earache, decreased hearing on right side for the past 3 months. Ear examination showed hard bony mass filling the ear canal and tympanic membrane was not visualised. Tuning fork tests showed conductive hearing loss in the right ear. Computerised axial tomography of temporal bone showed a pedunculated bony mass arising from posterior wall of right ear canal with a soft tissue mass filling the medial part of ear canal. Through the post aural route, bony mass and soft tissue mass in the ear canal was removed and canaloplasty was done. Histopathological examination of bony mass showed features of an osteoma and soft tissue mass in the ear canal showed features of cholesteatoma.
Keywords: Osteoma, Ear canal cholesteatoma
Cite this paper: Mylanahalli Doddarangaiah Prakash, Borlingegowda Viswanatha, Maruvala Shreeharsha, Sandhya Patil, External Ear Canal Osteoma with Canal Cholesteatoma; a Rare Association, Research in Otolaryngology, Vol. 3 No. 5, 2014, pp. 70-72. doi: 10.5923/j.otolaryn.20140305.02.
1. Introduction
- Osteomas are slow growing benign tumours rarely involving parts of the temporal bone. External ear canal [EC] is commonest site of involvement in the temporal bone with an estimated incidence of 0.5% of total otologic surgery [1]. EC cholesteatoma is similarly a rare entity seen in about 0.1-0.5% amongst new patients [2]. The association of ear canal osteoma with canal cholesteatoma is rare and only few cases have been reported in the literature.
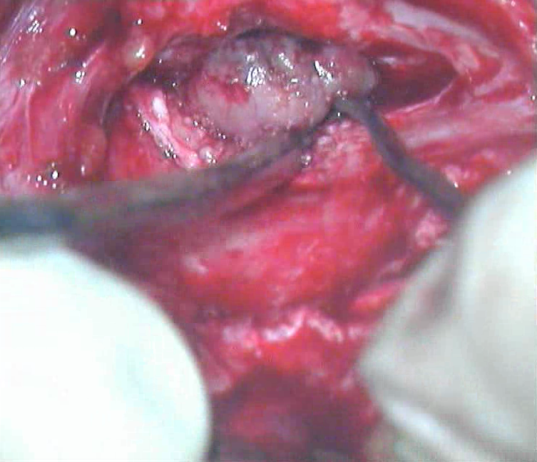
 | Figure 1. Preoperative picture of osteoma |
2. Case Report
- A twenty-one year old male patient presented to otolaryngology department with complaints of ear ache, decreased hearing on right side for the past 3 months. On ear examination an oval mass was present in the right ear EC and it was filling whole of EC, just lateral to the level of isthmus [Figure 1].
 | Figure 2. Intraoperative photograph showing pedunculated bony mass arising from the posterior canal wall |
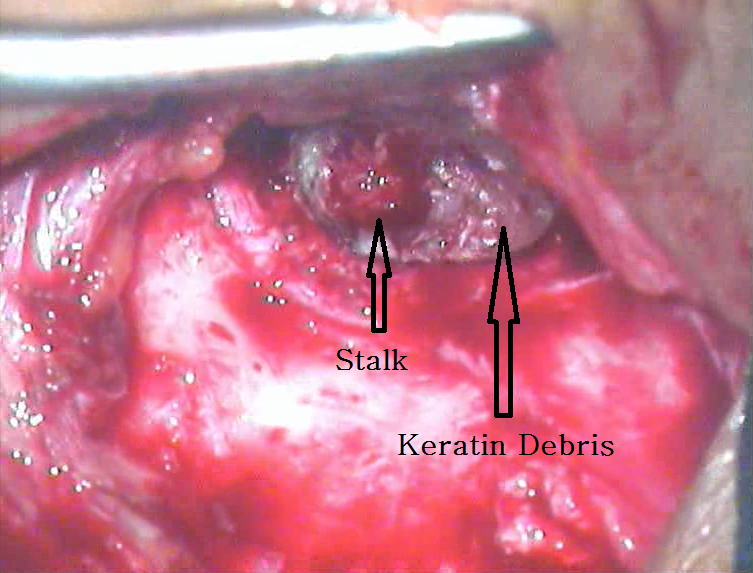 | Figure 3. Intraoperative photograph showing osteoma stalk and keratin debris below |
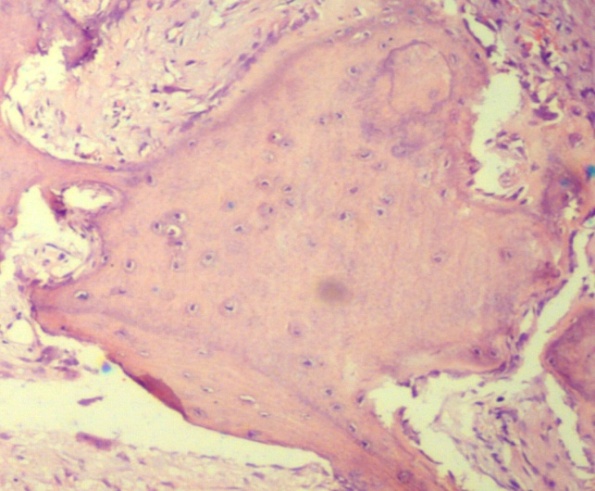 | Figure 4. Microphotograph showing mature lamellar bone and fibro vascular tissues |
3. Discussion
- Osteomas have been classified in many ways like unilateral or bilateral, by their pattern of growth into in growing or outgrowing, and according to histopathological appearance as spongeous or compact or mixed [3]. Asymptomatic incidental finding is the most common mode of presentation of an ear canal osteoma. It can present with a serious complication when it is associated with ear canal cholesteatoma, which erodes the surrounding structures [4].The osteomas are benign true bone tumours rarely encountered in head and neck and in EC it is still rarer. It can be easily diagnosed from otoscopic examination and clinical examination. It must be differentiated with the counterpart disease like exostosis of the EC. There are still unsettled controversies whether to consider these both as single pathological entity. But clinically osteomas are unilateral, single pedunculated and situated in suture lines in contrast to exostosis denoting a reactionary condition which presents with multiple sessile and bilateral disease.The incidence is more in young adults and more commonly seen in 3rd and 4th decade. Our patient was is in early 3rd decade. This is a male predominant disease of unknown aetiology. The aetiopathogenesis of osteoma remains controversial. Reported etiologic factors have included trauma, surgery, radiotherapy, chronic infections, heredity, and glandular conditions, such as pituitary dysfunction [4]. Varboncoeur et al [5] suggested that osteomas arise either from an embryonal cartilaginous rest or from a persistent embryologic periosteum. Yamasoba et al [6] proposed that osteoma may be of a congenital nature, based on their reported case of an osteoma that was seen in conjunction with congenital cholesteatoma. On CT scan, osteomas typically appear as a well circumscribed mass without surrounding bony destruction. Histopathologically, they are made up of discrete fibrovascular channels surrounded by lamellar bone. Pathologically, osteomas are classified as: 1. Osteoma compactum- histologically composed of dense lamellated bone tissue traversed by few vessels.2. Osteoma cancellare - consists of cancellous bone and fibrous cellular tissue.3. Osteoma cartilagineum - consists of bone and cartilage.4. Osteoma mixtum - consists of mixture of types of bone found in osteoma compactum and osteoma cancellare [7, 8].The decision regarding whether to operate or not depends on each case depending on its size, symptoms and more importantly the complications. The symptoms arise mainly due to the interference of desquamation process of EC skin with potential to develop cholesteatoma and erode the surrounding structure. There have been even reports of extra cranial (invasion into the mastoid cavity, facial canal erosion) and intracranial complications (cerebellar abscess, meningitis) with such cases [4].
4. Conclusions
- Osteoma is a slow growing asymptomatic benign tumour. It becomes symptomatic when it is large enough to occlude the sound waves and alter the physiology of external ear canal. Complication of external ear canal osteoma is external ear canal cholesteatoma and early surgical intervention is advised to prevent complications.