-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(4): 57-59
doi:10.5923/j.otolaryn.20140304.02
Cholesteatoma of Maxillary Sinus Mimicking Malignancy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLGudigenahally Madaiah Puttamadaiah, Maliyappanahalli Siddappa Vijayashree, Borlingegowda Viswanatha, Japneet Kaur
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Maxillary sinus cholesteatoma is a rare clinical entity with only a few cases reported in the literature. In our case a 25 year female patient presented with 6 month history of blood stained nasal discharge on the left side and 1 month history of nasal deformity. Nose examination revealed a white cystic mass in the left nasal cavity. CT scan showed a soft tissue mass seen in left maxillary sinus with the erosion of medial and lateral wall of the maxilla. Mass was removed through transnasal endoscopic route. Histopathologic examination of the excised mass revealed a fibrocollagenous wall that lined with the stratified squamous epithelium. The epithelium was overlaid with lamellar layers of keratin Histopathologic diagnosis was cholesteatoma. This case is reported for its unusual presentation.
Keywords: Cholesteatoma, Maxillary sinus
Cite this paper: Gudigenahally Madaiah Puttamadaiah, Maliyappanahalli Siddappa Vijayashree, Borlingegowda Viswanatha, Japneet Kaur, Cholesteatoma of Maxillary Sinus Mimicking Malignancy, Research in Otolaryngology, Vol. 3 No. 4, 2014, pp. 57-59. doi: 10.5923/j.otolaryn.20140304.02.
1. Introduction
- Maxillary sinus is lined by respiratory epithelium. A cholesteatoma (epidermoid inclusion cyst) is a cystic keratin-filled mass lined with stratified squamous epithelium. In the maxillary antrum, invasion of the buccal epithelium via an oral antral fistula has been proposed as a possible etiology of an antral cholesteatoma. The cholesteatoma is often present within a chronically infected sinus. [1] Involvement of maxillary sinus is very rare. Only few cases of maxillary sinus cholesteatoma have been reported in the literature. This case is reported for its unusual presentation.
2. Case Report
- A twenty-five year old woman presented with history of foul smelling blood stained nasal discharge from the left nasal cavity for the past 6 months. Since 1 month patient noticed nasal deformity. There was no past history of trauma.Clinical examination showed collapsed nasal bridge (figure 1). On anterior rhinoscopy reddish white cystic mass was seen occupying whole nasal cavity on the left side. Mass had pushed the septum to the opposite side. Right nasal cavity was narrow due to the displacement of the septum in to the right nasal cavity. Post nasal examination showed a reddish white mass completely filling the left choana. There was tenderness over the left maxillary sinus. Ear and throat examinations were normal. Nasal endoscopic examination showed a reddish white cystic mass filling the whole left nasal cavity.
 | Figure 1. Photograph showing collapsed nasal bridge |
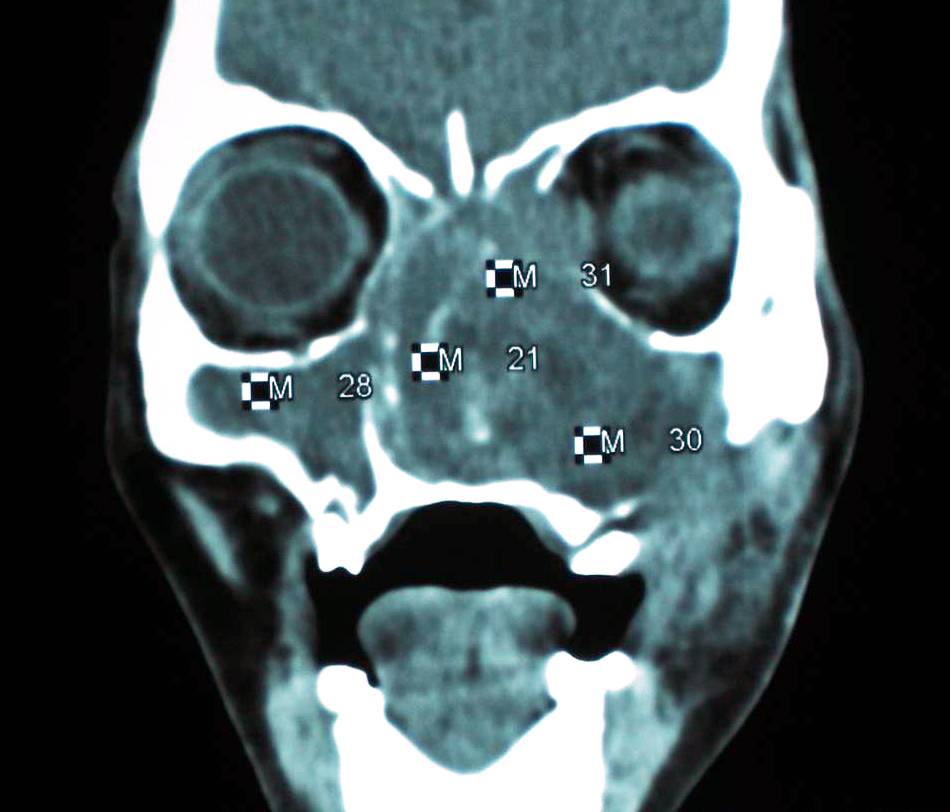 | Figure 2. CT scan picture showing soft tissue mass in the left maxilla with destruction of the medial and lateral wall of the sins and destruction of medial wall of the left orbit |
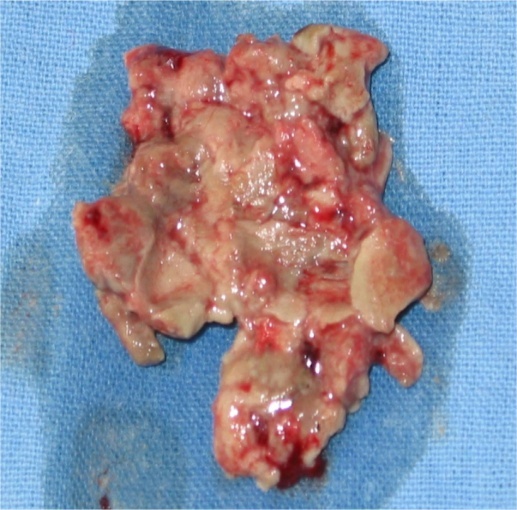 | Figure 3. Sowing mass removed from the left nasal cavity |
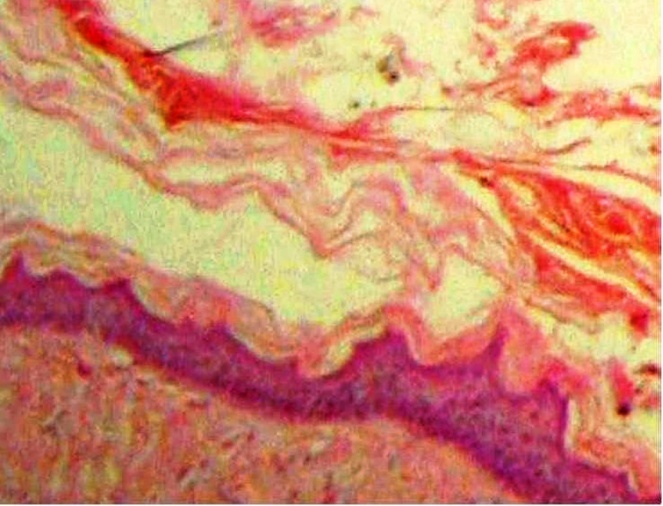 | Figure 4. Photomicrograph showing stratified squamous epithelium and lamellar sheets of keratin |
3. Discussion
- Cholesteatoma was first described by Cruveilhier in 1829 as a "pearly tumor because of its highly refractive and nodular surface [2]. The term cholesteatoma was given by Muller in 1838 [3]. Gordon 2007 proposed a theory according to which cholesteatoma is “a misdirected attempt to seal off a fistulous tract,” and that it should be specifically investigated in future cases of cholesteatoma in any part of the body, including the ear [4].When cholesteatoma occur in the facial bones, they probably arise from a congenital inclusion rest or a traumatic implantation [5]. Cholesteatomas can also arise in the cranium (including the temporal bone, orbit, and mandible), as well as in the skin, breast, kidney, and central nervous system5.Factors responsible for symptoms and signs are bone erosion, infection and anatomic relationship of maxillary antrum with orbit, nasal cavity, teeth, mouth and pterygomaxillary space [6]. Expansion of the cholesteatoma sac causes symptoms. As the cholesteatoma grows, pain becomes more severe. Extension of the lesion towards the osteomeatal complex causes rhinorrhea and sinusitis. Erosion of the anterolateral wall of antrum causes facial swelling and tenderness. Inferior erosion produces palatal swelling, and superior erosion produces proptosis. chemosis, erythema, and restriction of extraocular movements. Erosion into the nasal vestibule produces nasal obstruction. [6]Radiologically a typical cholesteatoma mimics maxillary mucocele. Cholesteatoma appears as a sharply circumscribed bony defect with smooth marginal sclerosis [7]. CT shows a cholesteatoma as a nonenhancing, expansile, homogenous lesion. On magnetic resonance imaging, it exhibits fairly low signal intensity on Tl-weighted imaging and high intensity onT2-weighted imaging [8].There are no consensus guidelines on the proper treatment of sinonasal cholesteatoma, although most authors recommend a Caldwell-Luc operation for maxillary sinus lesions. [6, 9, 10]. However in the present case, endoscopic removal of the mass was done. This procedure resulted in complete involution of the disease. On regular follow ups patient did not have any evidence of recurrence.Cholesteatoma of the maxillary sinus can sometimes mimics malignancy. To prevent the recurrence of the cholesteatoma, the walls of the cholesteatoma sac should be completely removed.