-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(4): 53-56
doi:10.5923/j.otolaryn.20140304.01
Osteoma Mastoid with Cholesteatoma of External Auditory Canal - A Rare Presentation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLGudigenahally Madaiah Puttamadaiah, Borlingegowda Viswanatha, Glen Edwin D’Souza
Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology Department, Bangalore Medical College & Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Osteomas of temporal bone are rare, slow growing neoplasm. They can occur in all parts of temporal bone, including the bony portion of the external auditory canal (EAC).A complication of osteoma of EAC is ear canal cholesteatoma. Here a male patient aged 37 years presented with history of right ear discharge for 10 years, decreased hearing for 8 years and a spontaneously discharging swelling with sinus in the post auricular region for 15 days. On examination of right ear there was complete obliteration of EAC by a hard bony mass and tympanic membrane was not visualised. The swelling in the post auricular region was fluctuant with mucopurulent discharge. Facial nerve examination was normal. Tuning fork tests showed conductive hearing loss in the right ear. Computerised axial tomography of temporal bone showed a solitary osteoma which was pedunculated arising from posterior wall of right EAC with a soft tissue mass filling the medial part of EAC and middle ear. A diagnosis of Osteoma of EAC with cholesteatoma was made and was posted for surgery. Modified radical mastoidectomy and tympanoplasty was done with complete excision of EAC osteoma and cholesteatoma.
Keywords: Osteoma mastoid, External auditory canal cholesteatoma
Cite this paper: Gudigenahally Madaiah Puttamadaiah, Borlingegowda Viswanatha, Glen Edwin D’Souza, Osteoma Mastoid with Cholesteatoma of External Auditory Canal - A Rare Presentation, Research in Otolaryngology, Vol. 3 No. 4, 2014, pp. 53-56. doi: 10.5923/j.otolaryn.20140304.01.
1. Introduction
- Osteomas of temporal bone are rare, slowly growing neoplasms. Osteomas occur in all parts of the temporal bone, including the EAC, mastoid and squamous portions, zygomatic process, glenoid fossa, middle ear, Eustachian tube, petrous apex, internal auditory canal, and styloid process. [1, 2, 3] Temporal bone osteomas are slow growing tumours whose exact aetiology is still not known. Probably, they arise from pre-osseous connective tissues, most often localized at the suture line [4].
2. Case Report
- A male patient aged 34 years from a village came to our hospital with chief complaints of painful swelling which was discharging behind the right ear since 15 days. He also gave the history of discharge from right ear for 10 years and decreased hearing in right ear since 8 years. On clinical examination of right ear there was complete obliteration of right EAC with a bony hard mass occupying the whole circumference of it. Tympanic membrane was not visible [Figure-1].
 | Figure 1. Photograph showing oval mass in the external auditory canal |
 | Figure 2. Photograph showing swelling in the right post auricular region |
 | Figure 3. CT scan showing pedunculated bony mass arising from posterior wall of right ear canal and soft tissue mass filling the medial part of the ear canal |
 | Figure 4. Intraoperative photograph showing pedunculated bony mass arising from the posterior bony ear canal |
 | Figure 5. Intraoperative photograph showing removed bony mass |
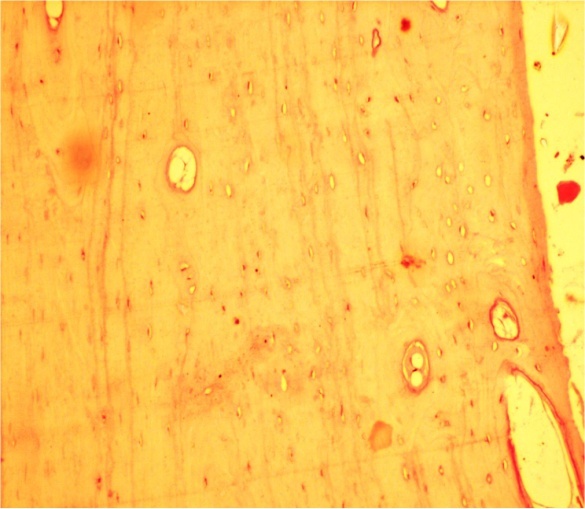 | Figure 6. Microphotograph showing mature lamellar bone and fibro vascular tissues |
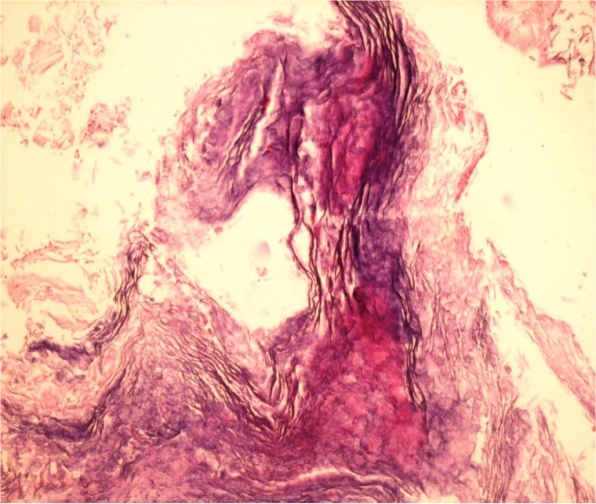 | Figure 7. Microphotograph showing stratified squamous epithelium and overlying lamellar sheets of keratin |
3. Discussion
- Temporal bone osteomas are slow growing tumours whose exact aetiology is still not known. Probably, they arise from pre-osseous connective tissues, most often localized at the suture line [4]. A variety of theories inciting their growth has been suggested from time to time including trauma with subsequent ossifying petrositis as suggested by Freiberg et al [5]. Other theories suggested that congenital mechanism and pituitary influence [6]. These tumours are most often found in post-pubertal age. The aetiopathogenesis of osteoma remains controversial. Reported etiologic factors have included trauma, surgery, radiotherapy, chronic infections, heredity, and glandular conditions, such as pituitary dysfunction. Varboncoeur et al [6] suggested that osteomas arise either from an embryonal cartilaginous rest or from a persistent embryologic periosteum. Yamasoba et al [7] proposed that osteoma may be of a congenital nature, based on their reported case of an osteoma that was seen in conjunction with congenital cholesteatoma. Kaplan et al [8] theorized that a combination of trauma and muscle traction may play a role in the development of osteoma. [9] Osteomas are commonly seen in the paranasal sinuses, but they are rarely found in the temporal bone [9, 10]. Ohhashi et al [11] reported that extracanalicular osteomas of the temporal bone occur twice as often in females and that EAC osteomas occur twice as often in males. Cholesteatomas of the external auditory canal is uncommon, observed in 0.1- 0.5% of patients who come with an otologic disorder [12, 13, 14]. External auditory canal osteoma is also a rare entity with an estimated incidence of of 0.05% of total otologic surgery [9]. The association that we are presenting here between an osteoma and cholesteatoma is extremely rare with only a few reported cases in literature [3, 12, 14, 15].On CT scan, osteomas typically appear as a well circumscribed mass without surrounding bony destruction. Histopathologically, osteomas are made up of discrete fibrovascular channels surrounded by lamellar bone. Pathologically, four types of osteoma has been identified: osteoma compactum, osteoma cancellare, osteoma cartilagineum, and osteoma mixtum [16].Complication of ear canal osteoma is external ear canal cholesteatoma. To prevent this complication, osteoma of the ear canal should be operated early. A case of osteoma with cholesteatoma of ear canal leading to posterior canal wall erosion and cerebellar abscess has been reported [3]. In a literature review in 2006 authors found only ten reported cases of external auditory canal cholesteatoma with posterior canal wall erosion and extension into the mastoid cavity, out of which in five cases facial canal erosion was present [3].Osteoma of the temporal bone with ear canal cholesteatoma is a rare clinical entity. These patients should be operated immediately to prevent complications of ear canal cholesteatoma.