-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(3): 49-51
doi:10.5923/j.otolaryn.20140303.04
A Rare Case of Isolated Nasal Neurofibroma Mimicking Sinonasal Polyp
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMylanahalli Doddarangiah Prakash, Borlingegowda Viswanatha, Glen Edwin D’Souza
Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Neurofibromas are benign peripheral nerve sheath tumors which originate from Schwann cells. They are known to occur in extremities as a local manifestation of Von Recklinghausen’s disease i.e. type 1 neurofibromatosis, but isolated neurofibroma occurring in the nasal cavity is a rare entity. Here we report one such case in a 60 year old lady who, presented to us with complaints of difficulty in breathing and a mass protruding from her right nasal cavity. Clinical diagnosis of inverted papilloma was made. Computed tomography suggested a polyp like mass lesion in the right nasal cavity, which was excised in toto by endoscopic endonasal approach. The mass was histologically confirmed to be a neurofibroma. Isolated neurofibroma, even though a rare entity in the nasal cavity should be thought of when history and clinical examination is not classical of other well-known nasal masses like sinonasal polyps or papillomas.
Keywords: Nasal neurofibroma, Sinonasal polyp
Cite this paper: Mylanahalli Doddarangiah Prakash, Borlingegowda Viswanatha, Glen Edwin D’Souza, A Rare Case of Isolated Nasal Neurofibroma Mimicking Sinonasal Polyp, Research in Otolaryngology, Vol. 3 No. 3, 2014, pp. 49-51. doi: 10.5923/j.otolaryn.20140303.04.
1. Introduction
- Neurofibromas are benign peripheral nerve sheath tumors. They arise from schwann cells and fibroblasts of the connective tissue of the endothelium. They are broadly classified into dermal and plexiform types. Dermal type is associated with individual peripheral nerves and plexiform types are usually associated with many nerve bundles [1]. Of the 25% to 45% neurofibromas that arise in the head and neck region, only 4% involve the nasal cavity and paranasalsinuses [2]. Solitary neurofibromas without associated von Recklinghausen's disease are rare. They have a malignant potential of 2.6% and if associated with von Recklinghausen’s disease, the chances for malignant transformation are 3-15% [3]. It is not unheard of for the plexiform variety to undergo malignant transformation [4].
2. Case Report
- A 60 year old lady presented to us at the outpatient department of our institute with a history of difficulty in breathing through her nose and a mass protruding from the right nasal cavity. She gave us a history of the mass being present in her nasal cavity for four years and was slowly growing in size. She first noticed heaviness and difficulty in breathing from the right nasal cavity about four years back and was clinically diagnosed to have a nasal polyp at the local hospital. Since the mass was growing in size and now was protruding from the nasal cavity, she was referred to medical college hospital for further management.She gave a history of 3 episodes of epistaxis which were after manipulation. The bleeding was scanty and stopped by itself on application of pressure over the nostril. Patient had mucopurulent nasal discharge which subsided on taking antibiotics. She complained of having generalized weakness and occasional hemicranial headache, which was relieved on taking analgesics. The patient is a known diabetic diagnosed about 12 years back and is on regular medication. She did not give a history of any other abnormal growth or lumps being present over her body or extremities.On anterior rhinoscopic examination, a pale pinkish polypoidal mass lesion was seen protruding from the right nostril which was soft, non tender, non shrinkable and did not bleed on touch [Figure 1]. A probe could be passed around it for about 1 cm. There was copious amount of mucopurulent discharge in the nasal cavity. The septum was deviated to the left, prominently where the mass was abutting it. Left nasal cavity was normal. There were no palpable neck nodes. On examination her ears and throat were normal.
 | Figure 1. Photograph showing mass protruding from the right nasal cavity |
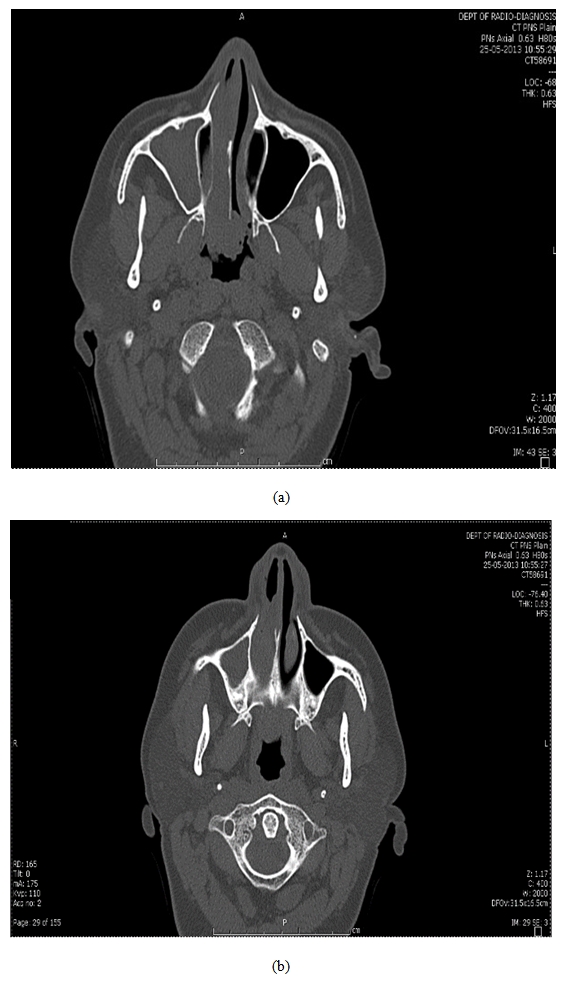 | Figure 2. CT scan images showing the extent of the mass in the right nasal cavity |
 | Figure 3. Photograph showing mass excised from the right nasal cavity |
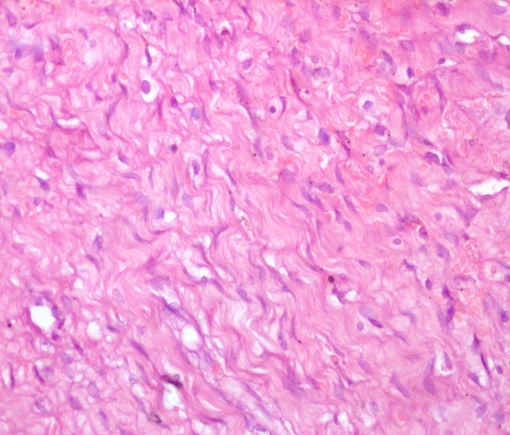 | Figure 4. Microphotograph showing spindle cells with wavy nuclei and myxoid stroma |
3. Discussion
- Neurofibromas are benign peripheral nerve sheath tumors. Nasal cavity involvement is seen in 4% of the cases [1]. On CT scan heterogenous contrast enhancement is seen in characteristically in neurofibromas [5, 6].Neurofibromas arise from the non myelinating schwann cells in the peripheral nervous system. They can arise from multiple peripheral nerve sheath tumors which sometimes arise from the head and neck area. Histopathological examination typically shows characteristic curved indented and ovoid schwann cell nuclei with spindle cells and wavy nuclei. Myxoid stroma in wavy fibrils can be appreciated [7, 8]. They are usually assoicated with neurofibromatosis which are autosomal dominant in nature and have neurofibromas arising from other sites in the body as well. Isolated cases of localised neurofibroma without other associated signs are a rare finding.Specifically, neurofibromas and schwannomas have been reported to occur in the nasal cavity, ethmoid sinus, maxillary sinus sphenoid sinus and very rarely the frontal sinus [8].Neurofibromas are more of a histological diagnosis thanks to the charateristic findings like spindle cells with wavy nuclei, wavy collagen fibrils and scattered mast cells. They need to be differentiated from schwannomas and malignant peripheral nerve sheath tumors though. Immunohistochemistry is of use in this regard when neurofibromas show reaction with S-100, NSE and Vimentin [1, 7, 8]. Surgical excision is the mainstay of treatment in symptomatic masses and various methods such as open, endoscopy assisted , endoscopic endonsal approach are employed for the same depending on the site and size of the lesion.
4. Conclusions
- A rare case of isolated neurofibroma of the nasal cavity which presented as polypoidal nasalmass was excised en masse using endoscopic methods and was diagnosed histopathologically as neurofibroma of the nasal cavity. The patient was symptom free during 6 months follow-up period. Immunohistochemisty may play an important role in dignosing nasal neurofibromas. Complete excision of the mass as far as possible provides relief from nasal symptoms. Endoscopic endonasal approach can be used as a treatment modality for such cases.