-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2014; 3(3): 46-48
doi:10.5923/j.otolaryn.20140303.03
A Unique Case of Keratocystic Odontogenic Tumor Mimicking Malignancy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMylanahalli Doddarangiah Prakash, Borlingegowda Viswanatha, Glen Edwin D’Souza
Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India
Correspondence to: Borlingegowda Viswanatha, Otorhinolaryngology department, Bangalore medical college & research institute, Bangalore, India.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Philipsen in 1956 [1] was the first person to describe odontogenic keratocyst (OKC). It is now designated by the World Health Organization (WHO) as a keratocystic odontogenic tumor (KCOT) and is defined as “a benign uni or multicystic, intraosseous tumor of odontogenic origin, with a characteristic lining of parakeratinized stratified squamous epithelium and potential for aggressive, infiltrative behavior” [2]. WHO recommends the term keratocystic odontogenic tumour as it better reflects its neoplastic nature [2]. They have an annual incidence of 3.5-5 per million population [3]. They usually but not always present as large multilocular cysts, which drives the patient to the hospital. Here we present a case of keratocystic odontogenic tumor in a 28 years old male patient who presented to us with a large hard painful swelling over the right cheek, with clinical features suggestive of malignancy of the maxillary sinus.
Keywords: Keratocysticodontogenic Tumor (KOCT)
Cite this paper: Mylanahalli Doddarangiah Prakash, Borlingegowda Viswanatha, Glen Edwin D’Souza, A Unique Case of Keratocystic Odontogenic Tumor Mimicking Malignancy, Research in Otolaryngology, Vol. 3 No. 3, 2014, pp. 46-48. doi: 10.5923/j.otolaryn.20140303.03.
1. Introduction
- Odontogenic cysts develop from redundant epithelium left behind in the jaws as a result of tooth development [4], but keratocystic odontogenic tumors are lined by parakeratinized and stratified epithelial lining whose basal layer has a neat arrangement of palisaded columnar and cuboidal cells, on top of which are several layers of squamous epithelium. This lining has a high mitotic rate and rarely can become dysplastic and develop into squamous cell carcinoma [5]. It isn’t unheard of for patients to wait till the pain supersedes the physical unsightliness in our part of the country for seeking medical attention. Here we present a case of a large keratocystic odontogenic tumor which occupied the whole of the right maxillary sinus mimicking malignancy of the area and brought the patient to us when he started experiencing pain in the area.
2. Case Report
- A 28 year old male presented with a history of swelling in the right cheek since 6 months. Initially it was 0.5X0.5 cms in size and it gradually increased to the present size over a period of 6 months. Patient came to the hospital after pain started in his right cheek. It was associated with unilateral headache and difficulty in chewing on the right side. There was no history of previous irradiation or surgery. No significant dental health issues were reported by the patient.On clinical examination a fixed hard oval mass of about 6X6 cms was present over the maxillary sinus region [Figure 1]. The skin over the mass was regular and it had a smooth surface. The mass was tender on deep palpation. The nasal examination and endoscopy was within normal limits. Oral cavity and oropharynx examination was within normal limits. There was no cervical lymphadenopathy.
 | Figure 1. Showing the patient with gross swelling at the right cheek |
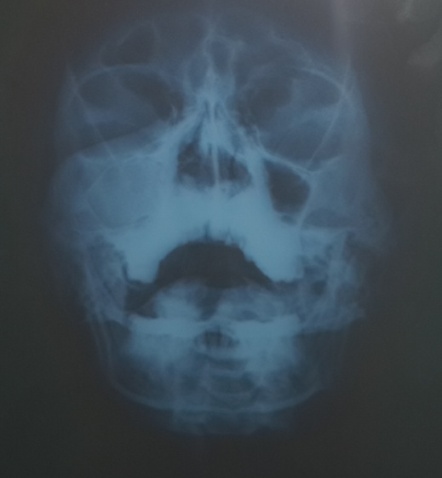 | Figure 2. Radiograph of paranasal sinuses [Water’s view] showing opacity in the right maxillary sinus |
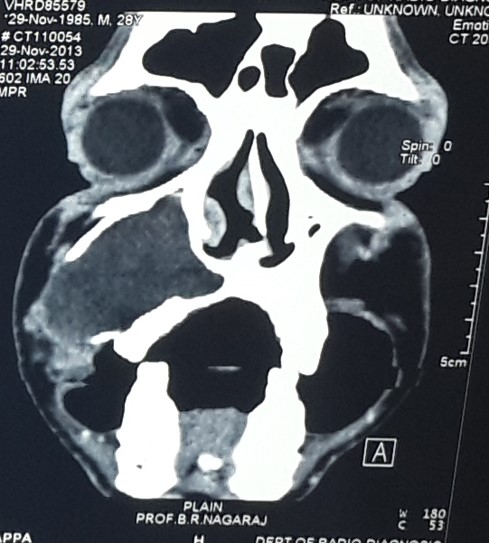 | Figure 3. CT scan image showing mass in the right maxillary sinus and erosion of the lateral wall |
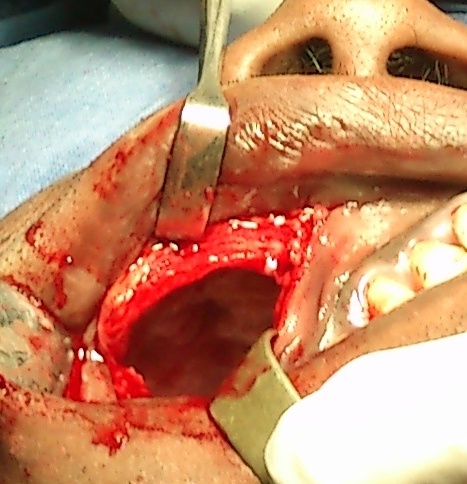 | Figure 4. Intraoperative photograph showing right maxillary sinus after removal of the mass |
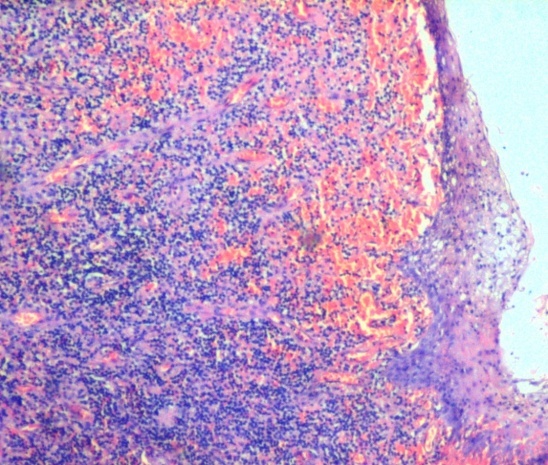 | Figure 5. Photomicrograph showing epithelial lining with parakeratinised cells, keratin debris and satellite cysts |
3. Discussion
- Keratocystic odontogenic tumors are low grade neoplasm supported by abnormal tumor suppressor genes [6]. Keratocystic odontogenic tumors have a peak incidence between the second and fourth decade of life. Usually they are asymptomatic and are found incidentally. They can be associated with erupted, unerupted or non tooth bearing areas of the jaw. They are commonly found in the mandible and the maxilla. They sometimes masquerade as large dentigerous cysts. Rarely do they reabsorb tooth roots and this makes them resemble neoplasm. Malignant transformation into squamous cell carcinoma is rarely reported at 0.12% [5, 6, 8].Treatment options include marsupilisation, enucleation with or without usage of Carnoys solution which is 1 g of ferric chloride (FeCl3) dissolved in 24 mL of absolute alcohol, 12 ml of chloroform, 4 ml of glacial acetic acid. These methods show a recurrence rate between 17% to 56%. Ghali and Connor report 0% recurrence after complete removal after radical treatment, but this may result in damage to inferior orbicular nerve, inferior alveolar nerve or tooth root. In addition reconstruction surgery may be required [9, 10].
4. Conclusions
- Keratocystic odontogenic tumors are low grade neoplasm which sometimes mimic malignancy. They may require surgical management when symptomatic. Recurrence rates being high are a matter of concern for the patient and the surgeon and complete removal is essential to prevent recurrence.