-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2013; 2(1): 12-14
doi:10.5923/j.otolaryn.20130201.03
A Rare Case of Sinonasal Cavernous Hemangioma
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLN. Dhanapala, C. Ravishankar, Ramya B., Supriya Bhat, Borlingegowda Viswanatha
Department of ENT, Bangalore Medical College and Research Institute, Bangalore, India
Correspondence to: N. Dhanapala, Department of ENT, Bangalore Medical College and Research Institute, Bangalore, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Hemangiomas are common benign lesions of the head and neck which predominantly originate from lips, tongue and buccal mucosa[1]. They occur infrequently in the sinonasal cavity[2]. Maxillary sinus hemangiomas are extremely rare[3]. They can produce destruction of the adjacent bones, making it difficult to differentiate it from the more common malignant epithelial tumors on the basis of imaging[2]. We report a case of maxillary sinus cavernous hemangioma in a 30 yr old male treated with endoscopic sinus surgery.
Keywords: Sinonasal, Cavernous, Hemangioma
Cite this paper: N. Dhanapala, C. Ravishankar, Ramya B., Supriya Bhat, Borlingegowda Viswanatha, A Rare Case of Sinonasal Cavernous Hemangioma, Research in Otolaryngology, Vol. 2 No. 1, 2013, pp. 12-14. doi: 10.5923/j.otolaryn.20130201.03.
1. Introduction
- Hemangiomas histologically are divided into two types, capillary and cavernous, depending on the dominant vessel size at microscopy[4]. The sinonasal cavity is an uncommon site of hemangiomas of the head and neck[2]. Most nasal hemangiomas arise from the nasal septum or vestibule and are of capillary type. Only a few arise from lateral wall of the nose and these are usually cavernous[5]. Being rare, they can cause diagnostic and therapeutic problems[6].Benign cavernous hemangiomas like inverted papillomas / sinonasal polyps can cause bone erosion, the appearance of which on CT scan can mislead the radiologist to the false diagnosis of a malignant tumor. At angiography, foci of pooling of contrast material within the lesion confirm the diagnosis of hemangioma. Complete excision of tumor is the treatment of choice.
2. Case Report
- A 30 yr old male presented to us with right sided nasal obstruction and intermittent epistaxis of 4 months duration. On examination, the right nasal cavity was completely obstructed by a friable, reddish-brown mass arising from the lateral wall which bled on probing. CT scans after Intravenous administration of contrast material showed a large heterogenous minimally enhancing soft tissue mass in right maxillary sinus and nasal cavity with the anterior and posterior walls of maxillary sinus were partially eroded. Excision biopsy of the nasal mass was done and the histopathology report showed features of cavernous hemangioma. Subsequently, endoscopic excision of the maxillary mass was done along with medial maxillectomy. Intra-operatively the anterior wall was found to be papery thin and the posterior wall was partially eroded. The intra and post-operative periods were uneventful with no significant hemorrhage encountered. Histopathology of the specimen confirmed the diagnosis of cavernous hemangioma with no features of malignancy. The patient is asymptomatic with no recurrence 15 months after surgery.
3. Discussion
- Hemangiomas, histologically are divided into two types, capillary and cavernous, depending on the dominant vessel size at microscopy[4]. Sinonasal hemangiomas are rare and when they occur they usually arise from nasal septum and vestibule. They are predominantly of cavernous type[2]. Maxillary sinus hemangiomas are extremely rare[3]. A recent review reported only 17 maxillary sinus hemangioma cases in the literature[7]. Maxillary sinus hemangiomas grow slowly and cause local destruction due to pressure effect[8]. Cavernous hemangiomas have a microscopic appearance of large blood filled canals lined with a single layer of endothelial cells and separated by scanty connective tissue stroma. Histologically, they are sharply defined but encapsulated lesions[6]. CT scan may show a) non homogenous mass due to areas of hemorrhage and necrosis, b) changes in adjacent bone with sinus expansion, c) bone destruction misinterpreted as sign of malignancy and / or d) phleboliths due to dystrophic calcification following intravascular thrombosis. But CT / MRI do not provide pathognomonic data for haemangiomas[8]. CT and MRI are especially of use to reveal the boundaries and the soft tissue extension of the lesion. Angiography is always warranted if there is any suspicion about the nature of these vascular tumors, as it enables us to decide if there is any need for transarterial embolization, in order to prevent hemorrhage during surgical intervention[2].Differential diagnosis should include neuroma, inverted papilloma, mucocele and other benign or malignant vascular tumors[8]. Complete excision of the tumor is the treatment of choice and no recurrence has been reported following paranasal hemangioma surgery[6]. Intraoperative hemorrhage related to hemangiomas is variable and it presents with minimal or massive bleeding[7]. The fear of sudden loss of large quantities of blood is more with cavernous hemangiomas than with capillary type[9]. In our case, the short history and partial erosion of anterior and posterior maxillary walls arouse a high degree of suspicion of malignancy. The opacification of ethmoidal cells which were interpreted as inflammatory changes due to obstruction of middle meatus were confirmed during surgery.
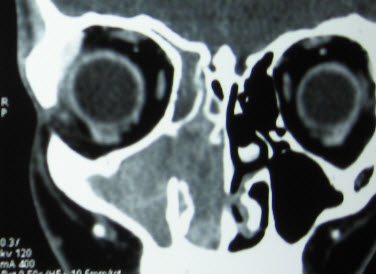 | Figure 1. Coronal CT image of Paranasal sinuses showing heterogenous mass occupying right maxillary sinus and right nasal cavity |
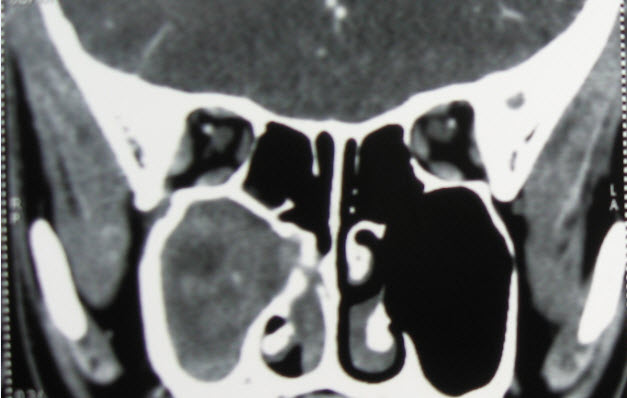 | Figure 2. Coronal CT image of Paranasal sinuses showing heterogenous mass occupying right maxillary sinus and right nasal cavity |
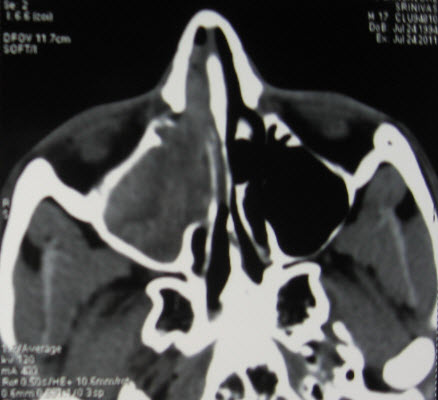 | Figure 3. Axial CT image of paranasal sinuses showing heterogenous mass occupying the right maxillary sinus along with partial erosion of anterior wall of the maxillary sinus |
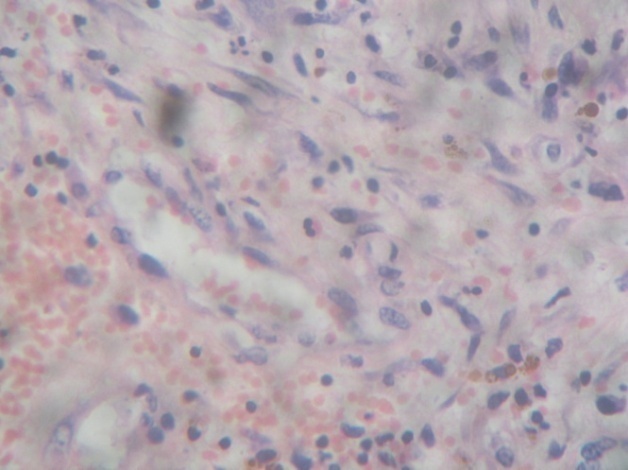 | Figure 4. Histology slides showing large (cavernous) spaces, lined by tumor endothelial cells (which appear very similar to normal cells). These interconnected spaces are filled with blood and separated by a fibrous tissue |
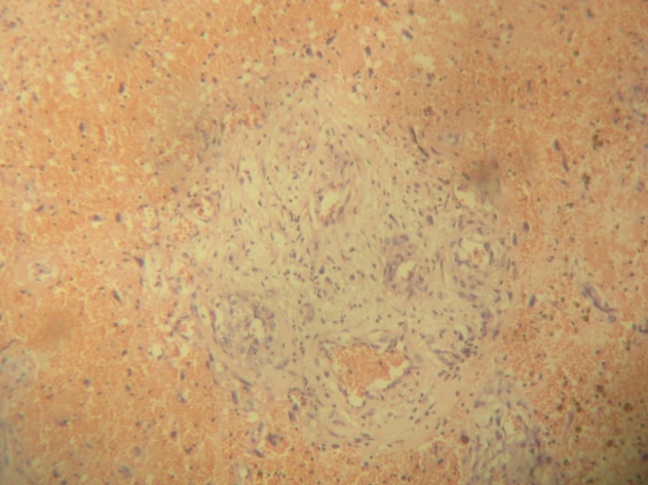 | Figure 5. Histology slides showing large (cavernous) spaces, lined by tumor endothelial cells (which appear very similar to normal cells). These interconnected spaces are filled with blood and separated by a fibrous tissue |
4. Conclusions
- Sinonasal tumors with bone erosion should not be presumed to be malignant always. Benign cavernous hemangiomas of sinonasal cavity, though rare, can cause substantial bone erosion and should be considered in the differential diagnosis of sinonasal tumors.