-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Otolaryngology
p-ISSN: 2326-1307 e-ISSN: 2326-1323
2013; 2(1): 6-11
doi:10.5923/j.otolaryn.20130201.02
Telephonic Conversational Difficulty as the Sole Symptom in a Patient with Cerebellopontine Angle Epidermoid: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShivashankar N.1, Taly A. B.2, Rose Dawn Bharath3, Prem. G.4
1Department of Speech Pathology and Audiology, National Institute of Mental Health and Neuro Sciences, Bangalore, India
2Department of Neurology, National Institute of Mental Health and Neuro Sciences, Bangalore, India
3Department of Neuroimaging and Intervention Radiology, National Institute of Mental Health and Neuro Sciences, Bangalore, India
4Department of Speech pathology and Audiology, Amrita Institute of Medical Sciences and Research Centre, Kochi, India
Correspondence to: Shivashankar N., Department of Speech Pathology and Audiology, National Institute of Mental Health and Neuro Sciences, Bangalore, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The objective of this case report is to highlight the importance of audiological investigations in a patient whose sole complaint was difficulty hearing over telephone. The patient is a 45 year old man, approached for an amplification device for his reported difficulty of hearing over the telephone in the left ear of five years duration. A telephonic conversation test revealed functionally adequate hearing bilaterally. However, detailed audiological investigations suggested left retrocochlear lesion with possible involvement of the brainstem. This audiological formulation led to neuroimaging studies, which identified an epidermoid in the cerebellopontine angle. Thus, this case report emphasizes the importance of detailed audiological work-up in patients who are neurologically asymptomatic to unravel the neuroauditory lesions.
Keywords: CPA Tumors, Dichotic Digits Test, Auditory Brainstem Response, Telephone Conversation
Cite this paper: Shivashankar N., Taly A. B., Rose Dawn Bharath, Prem. G., Telephonic Conversational Difficulty as the Sole Symptom in a Patient with Cerebellopontine Angle Epidermoid: A Case Report, Research in Otolaryngology, Vol. 2 No. 1, 2013, pp. 6-11. doi: 10.5923/j.otolaryn.20130201.02.
1. Introduction
- The cerebellopontine angle (CPA) is one of the most common sites of intracranial tumors and approximately 10% of them originate in the CPA. The primary tumors of the CPA include vestibular schwannoma (VS), meningioma, epidermoid, arachnoid cyst, schwannoma of the Vth, VIIth, IXth, Xth and XIth cranial nerves, primary melanoma, hemangioma, lipoma, dermoid and teratoma[1]. Epidermoid tumors account for approximately 1% of all primary intracranial tumors and amongst them 40% appear in the CPA site[2]. Hearing impairment has been reported to be one of the common manifestations in them accounting for 37.6% followed by trigeminal neuralgia, 29.7%; dizziness or vertigo, 19.4%; facial palsy, 19.4%; headache, 17.9%; and diplopia, 16.7%[2]. However, difficulty listening over the telephone as the sole manifestation of hearing impairment is rare. The present case study reports this unusual feature in a patient who incidentally sought hearing aid fitting in the presumed impaired ear. The objective of this paper is to highlight the importance of application of audiological test protocol in unraveling the silent lesion.
2. Case Report
- Mr. BK aged 45 years, male, sought for a suitable hearing aid to his left ear for his reported difficulty to engage in telephonic conversations for the last five years. The patient had a history of one episode of brief lasting pain over the left face a year ago. He was clinically diagnosed to have left trigeminal neuralgia and treated with carbamazepine successfully. He had not reported hearing impairment at the time of neurological consultation. Following the diagnosis of left trigeminal neuralgia, few months later, reported to have experienced a brief lasting dizziness that remitted spontaneously. He denied any other neurological or systemic symptoms at the time of audiology consultation. He was able to carry on otherwise, with his professional as well as personal duties efficiently.
3. Methods
- The audiological approach was in the following order; 1. Telephonic conversation test. 2. Puretone audiometry and Speech audiometry tests (Speech Reception Threshold-SRT, Speech Discrimination Score-SDS & Performance Intensity for Phonetically Balanced test-PIPB). 3. Dichotic Digits Test (DDT). 4. Immittance audiometry. 5. Auditory brainstem response (ABR) and 6. Distortion Product Otoacoustic Emission (DPOAE) measurements. All audiological tests were carried out with standard procedures and test situations.
4. Results
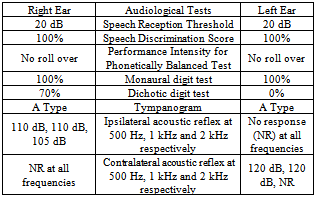
- A telephonic conversation test that was carried out demonstrated no difficulty in speech understanding in both ears. Appreciating his ability to hear in both ears with equal efficiency, the patient shunned the plan of hearing aid fitting in the alleged hearing impaired left ear. However on inquiry, he reported that ‘speech signals’ in the left ear were not ‘as sharp’ as that of the right ear. This was probably the salient description of his reported hearing difficulty. Thus, he was further subjected to puretone and speech discrimination tests. The pure tone audiometry showed hearing within 20 decibel (dB) in both ears at all octave frequencies from 250 Hz-8 kHz on air conduction testing. The SRT was 20 dB in both ears. The speech discrimination (SD) in quiet was 100% in both ears. No roll-over effect was observed for PIPB. Despite tests showing normal speech discrimination the patient was subjected to DDT because of his reported feeling of ‘reduced sharpness in speech’. Prior to the administration of the DDT, monaural digits test (MDT) score was ascertained which yielded 100% score in both ears. The DDT demonstrated left ear extinction (0%) while the right ear score was 70% (Table 1). This finding implicated a central auditory disorder making further audiological investigations inevitable. Immittance audiometry revealed normal “A” type tympanograms in both ears that suggested normal middle ear function. The acoustic stapedius reflex was absent left ipsilaterally and right contralaterally. It was present at normal sensation level right ipsilaterally but elevated left contralaterally (Table 1).
|
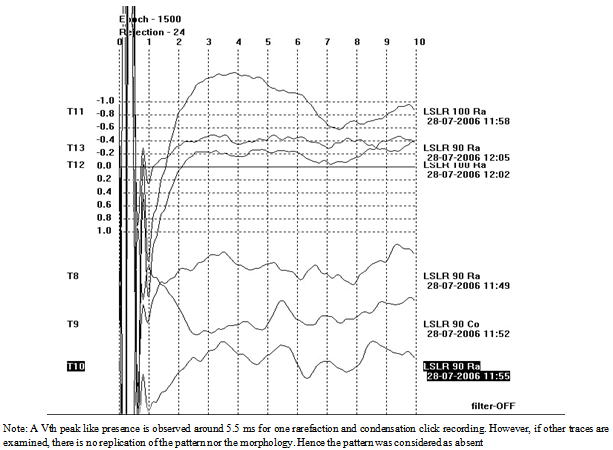 | Figure 1. Left ear ABR for rarefaction clicks at 90 dB nHL. LSLR refers to left stimulation with left recording |
 | Figure 2. Right ear ABR for rarefaction clicks at 90 dB nHL. RSRR refers to right stimulation with right recording |
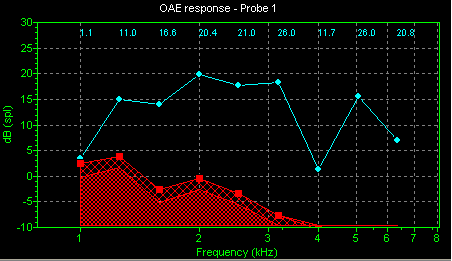
 | Figure 3. Left Ear DPOAE |
 | Figure 4. Right ear DPOAE |
 | Figure 5. MRI T1 weighted sagittal image through the right para sagittal plane showing extrinsic compression of the mid pons by a well defined hypointense lesion |
 | Figure 6. T2 weighted axial image revealing an extra axial hyperintense lesion in the left CP angle, prepontine cistern crossing on to the right CP angle compressing and displacing the mid pons anterolaterally |
5. Discussion
- Congenital intradural epidermoid tumors are the third most common tumors of the CPA site[3]. Epidermoids are slowly progressive tumors[4]. Therefore, symptoms may surface late in the course of the illness. However, patients often present relatively early when the predominant symptom is trigeminal neuralgia[5]. The symptoms and signs are caused by displacement of the adjacent neurovascular structures. Approximately 64% of epidermoid tumors have been reported to have secondary trigeminal neuralgia[6]. Our patient had a history of one episode of brief lasting pain and was clinically diagnosed to have left trigeminal neuralgia. He was treated with carbamazepine successfully.Greater proportion of normal hearing in nonacoustic tumors of CPA site has been reported by Hirsch & Anderson [7]. In their study 50% of patients in the nonacoustic group had demonstrated normal hearing as against 23% in the VS group and the difference between these two groups was statistically significant. They also have reported greater prevalence of poor speech discrimination in acoustic tumor ears on comparison with nonacoustic tumor ears (47% versus 35%). Our patient had also demonstrated normal hearing bilaterally with normal speech discrimination score. Higher proportion of normal hearing in the nonacoustic type tumors may be due to relatively less involvement of auditory nerve. However, Dawes and Jeannon[8] reported no difference in the pattern of hearing loss with respect to tumor type. Their patient population consisted of VS and facial neuroma and the findings noted were attributed to the close proximity of both VS and facial neuroma with the auditory nerve. Lakhdar et al[9] have reported that the audiometric explorations provided only orienting contribution in their surgical series of 10 patients.The left ear extinction on DDT implicated suppression of left sided caudal brainstem auditory pathways in this patient in the presence of good performance on MDT as well as 100% speech discrimination bilaterally. This was rather a defining point for a suspicion of retrocochlear pathology. The clinical utility of the DDT in identifying brainstem lesion have has been well documented[10, 11].In our patient the pattern of acoustic stapedius reflex abnormality strongly suggested left ear retrocochlear pathology with possible involvement of the brainstem. There was no clinical evidence of facial nerve disorder in the patient. Hirsch and Anderson[5] have reported acoustic reflexometry findings in CPA tumor patients classified based on tumor type. They observed comparatively higher efficacy for stapedius reflex tests in identifying nonacoustic CPA tumors. Efficacy of contralateral stapedius reflex estimation in CPA tumors identification has also been reported by Mangham et al[12] and Ferguson et al[13]. The ABR which reveals auditory nerve synchrony, showed absent response in both ears in our patient and suggested dysfunction at the brainstem level. It is interesting to note the discrepancy between the results of ABR and speech discrimination score in our patient. This may be due to the epidermoid tumor type itself, being creepy in nature exerts less effect on stimuli rich in external redundancy like the test used in the current study such as, speech discrimination, PIPB or MDT. The tumor presence was unraveled only when we employed less redundant stimuli such as dichotic test or short duration stimuli like click used in the ABR. Bilateral absence of ABRs in our patient may be due to extensive tumor invasion. The presence of DPOAE in both ears also suggested intact vascular supply to the cochleae in the presence of the tumor. This finding goes in correspondence with Mobley et al[14] study which has shown fewer propensities of nonacoustic tumors of the CPA to cause sensory hearing loss via blood supply disruption to outer hair cells.Our patient’s audiological findings suggested two possibilities; left ear retrocochlear pathology with brainstem involvement or bilateral retrocochlear lesions. The former was considered most likely diagnosis as the performance on DDT in the right ear is 20% below the normal score that lessened the possibility of bilateral lesion. These findings were consistent with his reported difficulty of telephonic conversation in the left ear. The audiological diagnosis led to an MRI scan, which identified a space occupying lesion in the CPA site. Generally epidermoid tumors are located anterolateral or posterolateral to the brainstem and tend to expand where physical resistance is low and may extend around the brainstem into the contralateral cistern[15]. In congruence with the nature of the epidermoid tumor, our patient also had extensive invasion extending into the right CPA region with no demonstrable hearing loss. Audiologically the only complaint was of conversational difficulty over the telephone. No surgical intervention was planned as the patient continued to be asymptomatic neurologically and is so till date. A similar presenting symptom of difficulty in conversing over the telephone in an eight year old child and ultimately the audiological evaluation led to the diagnosis of a space occupying lesion which was later confirmed by the imaging study revealing a cerebellar pilocytic astrocytoma has been reported by Berg et al[16]. Their patient had mild sensorineural hearing loss in the right ear and slight low frequency sensorineural hearing loss in the left ear with poor speech recognition in the right ear. The acoustic stapedius reflex was absent right ipsilaterally and left contralaterally. The ABR was normal in the left ear and only wave I was present in the right ear. In contrast, our patient had audiometrically bilateral normal hearing with good speech recognition score, absence of acoustic stapedius reflex left ipsilaterally and right contralaterally as well as elevated left contralaterally and extinction of the left ear on dichotic test. The only common symptom between these two patients was their inability to follow conversation over telephone. The audiological diagnosis in the present case could have been missed if only puretone audiometry was done as adopted in the traditional way of audiological testing.
6. Conclusions
- It was the hearing difficulty over the telephone in the left ear that prompted this patient to seek the help of an audiologist for hearing aid fitting. The audiological detection of a space occupying lesion which was confirmed by the imaging studies emphasizes the importance of audiological investigations in identifying the nature of the disorder. The highlight of the present report is the importance of ascertaining auditory behavior and administration of auditory tests in identifying retrocochlear lesions. Thus, audiological investigations could well be a preliminary diagnostic tool in identifying the silent lesions affecting the auditory system.