-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Ophthalmology
p-ISSN: 2471-7444 e-ISSN: 2471-7460
2018; 4(1): 7-8
doi:10.5923/j.ophthal.20180401.02

Transient Unilateral Sixth Nerve Palsy after General Anaesthesia, a Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAhmed Elabhar1, Talal Althomali2
1Ophthalmology Specialist, Saudi Arabia
2Pediatric Ophthalmology Consultatnt, Saudi Arabia
Correspondence to: Ahmed Elabhar, Ophthalmology Specialist, Saudi Arabia.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This is an unexpected case that was not reported before of transient isolated unilateral abducens nerve palsy after squint surgery under general anesthesia of a four years old Saudi girl. The patent underwent short uneventful lateral rectus recession in both eyes as a surgical correction of consecutive exotropia. 1st post operative day showed restricted abduction of the right eye not crossing the midline. Exploration excluded slipped lateral rectus muscle of the right eye and showed muscle in aimed position. [figure 2]. Full recovery of movement occurred one week later without residual restriction [figure 3]. Diagnosis was made as transient isolated abducens (sixth) nerve palsy for further assessment.
Keywords: Sixth nerve palsy
Cite this paper: Ahmed Elabhar, Talal Althomali, Transient Unilateral Sixth Nerve Palsy after General Anaesthesia, a Case Report, Research in Ophthalmology, Vol. 4 No. 1, 2018, pp. 7-8. doi: 10.5923/j.ophthal.20180401.02.
1. Introduction
- Isolated sixth cranial nerve palsy after lumbar puncture was firstly reported by Koeppen in 1967 [1]. Several similar cases were reported in the context of literature and extra ocular muscle paralysis was documented as a possible complication after spinal anesthesia [2]. What makes this case report unique is that lateral rectus muscle paralysis after general anesthesia was never reported in literature before , although their was a single case of isolated sixth nerve palsy in child who underwent three prolonged surgical procedures for managing of his Hirschsprung's-disease and postulated to be a complication to prolonged general anesthesia in 1972 [3], but this differs from that case as our surgery was short and uneventful and the paralyzed muscle was included in the surgical procedure.
2. Case Report
- A four years old female child was presented to our center with large consecutive exotropia. Her father handed us a discharge report of previous surgical intervention for correction of a 60 prism diopeters infantile esotropia through bi-medial rectus recession 7 millimeters at the age of two years, and complaint that his daughter developed large outward deviation of her eyes after that surgical intervention. History of the patient showed exposure to perinatal asphyxia during spontaneous vaginal delivery with delayed developmental milestones and mental retardation.On examination: visual acuity was 20/20 in both eyes with painless full extra-ocular muscle movement in all cardinal positions both uni-ocularly and binocularly. A 45 prism diopters and 40 prism diopters exotropia were found for distant and for near respectively. Slit lamp examination of both anterior and posterior segments were unremarkable and diagnosis was made as consecutive exotropia. Decision was made to recess lateral rectus muscle for 8 millimeters in both eyes.Surgical intervention was done in modified hang back technique. Post operative examination revealed incomittent consecutive esotropia measured 80 prism diopeters in primary position [figure 1] with limited abduction of the right eye not crossing the midline. We suspected slipped right lateral rectus muscle and immediately admitted the patient for exploration. As a surprise we found that the lateral rectus muscle is in the aimed position [figure 2]. One week later the condition completely resolved and movement of right medial rectus regained with no residual restriction [figure 3]. Based on the clinical findings diagnosis was made as post general anesthesia transient isolated right sixth (abducens) nerve palsy for further investigations.
 | Figure 1. Post operative right sixth nerve palsy |
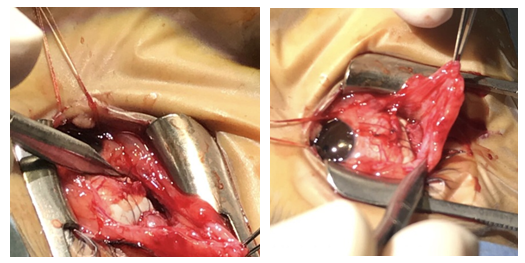 | Figure 2. Right lateral rectus muscle in aimed position during exploration |
 | Figure 3. Resolved sixth nerve palsy one week after surgery |
3. Discussion
- Common nerve damage associated with general anesthesia are hypoglossal nerve palsy, lingual nerve palsy, and external branch of laryngeal or recurrent laryngeal nerve palsies [4, 5]. Endotracheal intubation and use of laryngeal mask had been associated with cases of isolated or combined palsy of both hypoglossal nerve and lingual nerve in recent years [6].Idiopathic acquired sixth nerve palsy in childhood is common; other causes can be trauma, neoplasm, or inflammation. Pontine gliomas, elevated intracranial pressure, viral illness, ear or throat infections or benign recurrent sixth nerve palsy can be also among causes of acquired isolated abducens nerve palsies in children [7]. To our knowledge after literature review, this is the first transient isolated unilateral abducens nerve palsy case ever to be reported after uneventful surgical intervention done under general anesthesia.In our opinion, second surgery for exploration was mandatory to exclude slipped muscle after first surgery and has no relation to either sixth nerve palsy or spontaneous resolution of the case that followed. Perinatal asphyxia and cerebral palsy also has no direct relation to our case.
4. Conclusions
- Sixth nerve palsy of undetermined cause usually resolves spontaneously. If resolution does not occur within two to three months, the condition may persist. If additional neurologic signs or symptoms developed, imaging studies are indicated.