-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Ophthalmology
2013; 2(1): 1-3
doi:10.5923/j.ophthal.20130201.01
Barriers to Uptake of Cataract Surgery: An Eye Camp Account
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJosephine N. Ubah1, Micheline A. Isawumi2, Caroline O. Adeoti1
1Department of Ophthalmology, College of Health Sciences, Ladoke Akintola University of Technology, Osogbo, Osun State, Nigeria
2Osun State University, Osogbo, Osun State, Nigeria
Correspondence to: Josephine N. Ubah, Department of Ophthalmology, College of Health Sciences, Ladoke Akintola University of Technology, Osogbo, Osun State, Nigeria.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
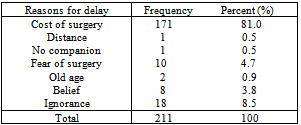
About 17.6m are blind from cataract global. In Nigeria about 486,000 Nigerians were estimated blind with a prevalence of about 1.8%. This level is still considered high. Cataract operation remains the only and very good option for treatment of cataract blindness. Factors preventing people from assessing sight restoration services remain a challenge to the eye care delivery. Free cataract surgeries is becoming a regular practice in Nigeria. Despite this practice, many people continue to turn out blind from cataract, either in one or both eyes. This study is interested in why people still present with blinding cataract. Through an interview assisted questionnaires, a descriptive study was carried out among cataract blind patients who turned up for cataract surgery during an eye camp. About 1570 persons were screened. Of this number, 297 were found to have cataract with visual acuity of 6/60 or worse.167 were bilaterally blind. Questionnaire was administered to the 297 persons. Complete information was obtained from 211 of the respondents. Cost of surgery was the greatest cause of delay in uptake of cataract surgery in 171 (81%) persons. This was followed by ignorance in18persons.Cost of surgery still causes a lot of delay in uptake of cataract surgery in the study population. Cataract surgical rate needs to be increased.
Keywords: Delay, Cataract Operation, Cost, Ignorance, Eyecamp
Cite this paper: Josephine N. Ubah, Micheline A. Isawumi, Caroline O. Adeoti, Barriers to Uptake of Cataract Surgery: An Eye Camp Account, Research in Ophthalmology, Vol. 2 No. 1, 2013, pp. 1-3. doi: 10.5923/j.ophthal.20130201.01.
1. Introduction
- About 17.6m are blind from cataract globally.[1] In Nigeria about 486,000 Nigerians were estimated blind with a prevalence of about 1.8% .[2] Cataract operation remains the only and very good option for treatment of cataract blindness. Over the years, new innovations have come up to restore the vision to even better levels compared to the pre morbid state. This applies to those with refractive errors prior to development of cataract. It has been observed that prevalence of cataract still remains high, especially in developing countries. Factors preventing people from assessing sight restoration services remain a challenge to the eye care delivery. This indirectly may have adverse effect on the earning power of the individual as well as the person taking care of him or her, and the society as a whole. This is especially applicable to those who are bilaterally blind. Delay in uptake of cataract operation could arise from the patients, relatives and the community on one hand, and the hospital on the other hand.[3] Problems related to patient could be fear, age, distance, one eye still okay, or patient feels he/she is fine. Barriers from close relatives include, lack of priority, financial constraints, no escort,discrimination against women, awaiting free treatment. Barriers from the community include unawareness of cataract treatment and beliefs.Barriers can also arise from the hospital, and these among others are no permanent cataract surgeon, low motivation for eye staff, high cost of surgery, quality of surgery and hospital protocols.During eye free camp programs in the country many people with cataract usually turn up. This necessitated this study to find out why they had not done the surgery before then.
2. Methods
- A descriptive study was carried out among candidates who were found to have cataract blindness during an eye camp in Osun State of Nigeria. About 1570 of them were screened. Of this number, 297 were found to have cataract with visual acuity of 6/60 or worse. 167 were bilaterally blind. Interview-assisted questionnaires were administered to them. The study was conducted in four localities in Osun State of Nigeria. All those who consented to supplying answers to the questions were included in the study. Those who either did not consent or did not answer the questions completely were excluded.Information on age, visual acuity and reasons for delay in uptake of surgery were obtained. Descriptive statistics was used to analyze the data.
3. Results
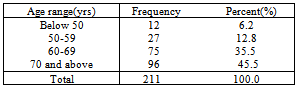
- Complete information was obtained from 211 of the respondents. The age distribution of the patients is shown in table 1 below.
|
|
4. Discussion
- This study has identified different reasons for delay in cataract surgery uptake in the study population. Cost was the major barrier, in more than 80% of the patients. In their study of 66 patients with cataract, 91.0% gave cost as the cause of delay in uptake of cataract surgery.[4] Cost has been cited in some other studies as the commonest cause of delay in presenting for cataract surgery.[5,6,7,8] In some instances, factors other than cost have been implicated.[9,10]In a study reported by Dhaliwal et al[9] behavioral barriers like patient being able to manage, can see with the other eye, too busy , fear of surgery etc, were found to be more dominant than the usual cost of surgery. Vaidyanathan K et al[10] observed a changing trend towards patients selection and service provision in the study they carried out in Karnataka State in India, patients had to wait for the cataract to mature. In Nigeria, cost seems to persist as the highest impediment to cataract surgery uptake.[5,8] Both direct and indirect costs, for example, expenses incurred by the companions of the patients constitute cost problems. In the country, Health Insurance Scheme is not yet well established. Many people still need to work hard to have access to health services. In some instances, the cost is subsidized or borne by the government, co-operate bodies and non-governmental organizations through eye camp programmes. Because these programmes are usually not steady, patients who cannot afford the cost of the surgeries tend to wait till one comes up. The second identified cause of delay is ignorance. The candidates were not aware of places where cataract surgical services were rendered. Some were afraid of operation. This problem usually arises where patients are aware of some persons who have had poor visual outcome. In these instances, the operation could have been for other eye problems. The poor visual outcome could also arise from cataract operation in people with blinding posterior segment problems. Patient selection, counseling and health education will assist in eliminating this problem. About 3.8% believed cataract was due to some reasons that could not be taken care of by operation. This is the superstitious group who may believe that there was a remote cause.Distance and lack of companion to the surgery venue were the least of the causes. Delay in cataract surgery uptake subsequently contributes to reduced cataract surgical rate and surgical coverage. According to the 2005-2007 blindness survey, only 28.8% of all cataract blindness in Nigeria had undergone cataract surgery meaning that more than ¾ of all the blind eyes were yet to be operated.[2]
5. Conclusions
- The current study has identified cost as the greatest cause of delay of cataract operation in Osun State of Nigeria. This seems to be the general trend in the other parts of the country where this type of study has been conducted. To take care of this and the other causes of delay, continual effort by the state government and well meaning organizations and individuals cannot be under estimated. Certain measures can be taken to tackle these problems. The National Health Insurance Scheme if well established can take care of cost to a great extent. Expansion of outreach programmes to different communities rather than concentrate in urban areas, and offering cataract surgical services at affordable rates will also be of help. Health Education has a great role to play as well, especially in creating awareness. Adequate dissemination of information through various media is usually will be very helpful. The media that are usually effective and are encouraged in the country include, town and trade unions, village meetings, churches, mosques, radio and television.