-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2024; 14(1): 1-21
doi:10.5923/j.nursing.20241401.01
Received: May 23, 2024; Accepted: Jun. 17, 2024; Published: Jun. 22, 2024

Perspective of Care: Challenges Faced by Family Caregivers with Cancer-diagnosed Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLCristian Rey A. Gecosala, Jainah Rose G. Amilbahar
College of Medicine and Allied Health Sciences, University of Southern Mindanao, Kabacan, Cotabato, Philippines
Correspondence to: Cristian Rey A. Gecosala, College of Medicine and Allied Health Sciences, University of Southern Mindanao, Kabacan, Cotabato, Philippines.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

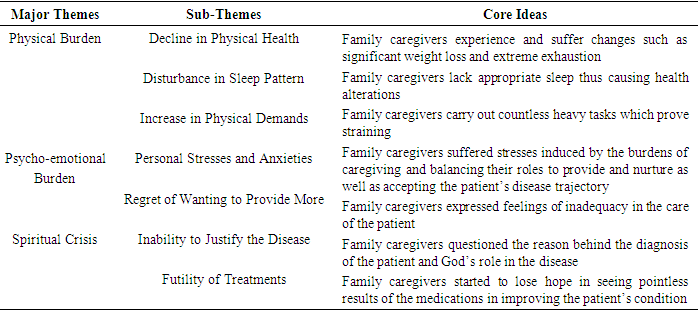
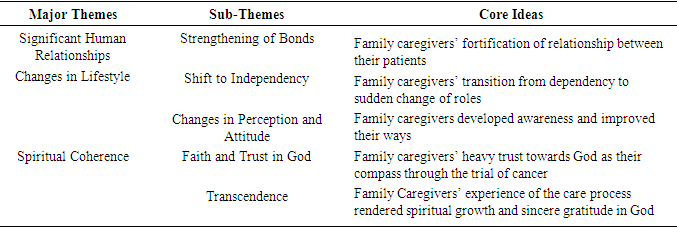
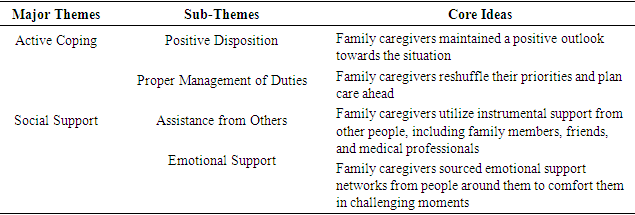
This study sought to explore, investigate, and analyze the data on the challenges faced by family caregivers in caring for the cancer-diagnosed patient. Specifically, this study aims the illumination of the following: gather data pertaining to the sociodemographic characteristics of the family caregivers and medical profile of the cancer-diagnosed patient; probe on the challenges faced by family caregivers in caring for the cancer-diagnosed patient; investigate on the outcomes the caregiving role had on the family caregiver’s lifestyle and outlook in life; and discover the coping mechanisms utilized by family caregivers in coping with their roles and responsibilities. By delving into these aspects, the study emphasized its purpose to profoundly understand the ways of care of family caregivers caring for cancer patients, propound methods that will advance cancer care and alleviate the difficulties undergone by this specific group, and formulate ways to put into structure a support system tending to their needs. The study was conducted from June 2023 to July 2023 utilizing a qualitative approach using one-on-one interview as its method of collecting data. The participants involved in this study were seven (7) coming from any provinces in the SOCCSKSARGEN region in the Philippines. Audio recorders, transcripts, and coding sheets of the participants’ statements were utilized to explore and understand the different challenges they undergo. Thematic Analysis was used as a method of exploring, analyzing, and understanding the challenges faced by family caregivers in caring for the cancer patient. Various themes emerged as manifestations of their challenges, the outcomes of the role in their lives, and how they coped with the responsibilities. The study put into light multifaceted struggles of family caregivers involving their personal lives, changes in physical and psycho-emotional health, and changes in their spirituality. In turn, these difficulties contributed significant outcomes which encompassed both positive and the negative. There are eight (8) major themes that emerged from this study: Physical Burden, Psycho-emotional Burden, Spiritual Crisis, Significant Human Relationships, and Changes in Lifestyle, Spiritual Coherence, Active Coping, and Social Support. It proves significant that the healthcare system must strengthen support structures that assist family caregivers. Challenges in undertaking care for terminally ill patients can decrease quality of life and can result in the decline of quality care given towards patients.
Keywords: Family Caregiver, Cancer, Coping Mechanisms of Family Caregivers, Challenges in Caring for a Cancer-diagnosed Patient
Cite this paper: Cristian Rey A. Gecosala, Jainah Rose G. Amilbahar, Perspective of Care: Challenges Faced by Family Caregivers with Cancer-diagnosed Patients, International Journal of Nursing Science, Vol. 14 No. 1, 2024, pp. 1-21. doi: 10.5923/j.nursing.20241401.01.
Article Outline
1. Introduction
- Cancer in its definition refers to a number of illnesses characterizing an uncontrollable development of cells that has the ability to destroy normal tissues. Cancer is a major public health issue in the Philippines, as well as in many other countries around the world. By the estimation of the International Agency for Research on Cancer back in 2018, there are reportedly 17 million cases of cancer and 9.5 million deaths related to cancer globally. In the Philippines in 2018, there were 141, 021 cancer cases and 86, 337 cancer-related deaths, according to statistics (World Health Organization, 2020). A Department of Health data from the year 2015 to 2019 accounted 0.25 percent of total mortality in the SOCCSKSARGEN region from cancer in all its forms. These figures show that there is a growing need to focus on cancer patients’ care. A significant shift that involved the health-care system occurred toward the end of the last century, with the goal of replacing hospital care with outpatient care and delegating responsibility for patient care to families; changes such as these in the health-care system made cancer care not an exemption. When a patient is diagnosed with cancer, both the family members and the patients are typically involved in the care process and in making important medical or health decisions (Qalawa, et al., 2015; Hassan, et al., 2016; Nady, et al., 2017; Mohammed, et al., 2018; Said, et al., 2018; Mohamed, et al., 2019; Masaud, et al., 2021; Farag, et al., 2024).Caring for a patient in the advanced stages of an illness presents significant challenges to the family caregiver’s personal life and can result in changes in all aspects of the individual's life. Individuals in stressful situations tend to assign meaning or explanation to their stressful experiences based on their worldview. Given the goal of palliative care, which is primarily to improve patients’ and caregivers’ quality of life, and in line with development programs aimed at assisting caregivers in providing quality care to cancer patients, examining the various challenges faced by family caregivers is critical. The present study, therefore, was conducted to investigate the challenges faced by Filipino family caregivers of patients with cancer during their caregiving processes (Nemati et al., 2017; Hassan, et al., 2021; Nady, et al., 2018; Atwa, et al., 2019; Abd El Salam, et al., 2021; Ali, et al., 2021; Ramadan, et al., 2021). Cancer is the leading cause of mortality around the globe, which by the year 2020 accounted for nearly one in every six deaths, with approximately 10 million fatalities recorded. Among the common cancers are those in the colon, lung, rectum, breast, and prostate (World Health Organization, 2022). Cancer affects 189 of every 100,000 Filipinos in the Philippines, with four Filipinos dying of cancer every hour, or 96 cancer patients every day. This is stated in a study undertaken by the University of the Philippines’ Institute of Human Genetics, National Institutes of Health. As reported in the 2015 Philippine Cancer Facts and Estimates, the most common cancer is breast cancer accounting to 20,267 cases and the third leading cause of cancer-related deaths (7,384 cases) among Filipinos, next to lung and liver cancer.Cancer is among the four epidemic non-communicable diseases (NCDs) or lifestyle-related illnesses (LRDs), which also include type 2 diabetes, chronic respiratory diseases, and cardiovascular diseases. Cancer is a term used to describe conditions in which defective cells divide uncontrollably and invade neighboring tissues. These cells can also metastasize to different areas of the body via the circulatory and lymphatic systems. Non-communicable diseases are now considered a massive “silent disaster” ravaging the Filipino population, claiming 300,000 lives per year, 800 per day, and 33 per hour. It has been compared to “two 747 planes packed with passengers colliding every day” in terms of human cost. Such diseases share several risk factors, which includes inadequate physical activity, an unhealthy diet, use of tobacco, and harmful alcohol use (Flores, 2022).Cancer cells have evolved mechanisms to avoid being destroyed by the body’s immune system. Researchers from all over the world are working on various strategies to circumvent these complex mechanisms (Diamond Light Source, 2022).As accounted in the year 2018, with 22.9% of cancers in females and over 2 million cases, breast cancer in women is the most common malignancy and the second most common cancer in the world (Seward and Wild, 2014). Although the prevalence is higher in Western Europe and North America, it’s increasing in developing countries as a result of increased life expectancy, urbanization, and the adoption of Western lifestyles. According to the American Cancer Society (2020), the five-year survival rate of 63% as of 1960 has recently improved to 90%, owing to an early detection of cancer through mammogram screening, as well as improved surgery and adjuvant treatment. As evidenced, breast cancer mortality rates fell to 6.6% in 2018 (Global Cancer Observatory, 2020; Kamal, et al., 2021; Nady, et al., 2018; Elzeblawy, et al., 2021).When a patient is diagnosed with cancer, it does not only significantly affect the patients but their family members as well. The source of emotional and social support for patients primarily comes from family caregivers. They have a relevant impact on how well patients cope with their illness. Along with these are the increasing cases of patients being left to self-manage their illnesses, which often makes them suffer the debilitating side effects of treatment at home, as hospital stays are becoming shorter. As a consequence, cancer patients’ family caregivers’ burden of responsibility has increased, emphasizing the significance of their role in supporting the patient. This review defines a family caregiver as ‘who the patient says it is'. Thus, FCs can encompass a wide range of relationships, including blood relatives, friends, neighbors, and others. Family Caregivers are indeed an important and valuable source of essential and unpaid support, supplementing other formal health care services (Hu et al., 2018).A reform from a family-as-patient perspective should be implemented, which includes family caregivers, given the critical role they play in illness management and the recovery of the patient. FCs have a significant contribution on clinical outcomes. Thus, we benefit patients indirectly by supporting family caregivers. Now, the question at hand is how to best assist family caregivers. FCs face a slew of issues and burdens associated with caregiving.With high morbidity and mortality rates, cancer affect patients and their families in a variety of aspects which places it as one of the most feared diseases. Cancer, as a life-threatening and long-lasting illness with various treatment modalities, forces families to deal with the physical, emotional, social, and financial burden it imposes (Abbasi et al., 2020; Lee Wong et al., 2020). Because cancer affects the entire family, the majority of caregivers for cancer patients were first-degree relatives. Caregivers, also patients, face numerous physical, social, mental, and economic challenges.Because cancer is a complex and multifaceted disease, a cancer diagnosis in a family member alters the daily routines of other members of the family and exposes them to new situations. As stated in the study of Üzar Özçetin and Dursun (2020), although most family caregivers willingly do these tasks and with a sense of accomplishment for tending to their dear family member, the burden and stress of providing care becomes evident as the caregiving process progresses. Numerous researches have shown that the burden of caregiving has a physical, social, and psychological impact on caregivers’ lives (Hsu et al., 2014; Vahidi et al., 2016; Govina et al., 2015, 2019; Lee Wong et al., 2020).The struggles of caregivers with the disease process also includes health care procedures, treatment appointments, witnessing the suffering of the patient and approaching death, their constant fear of losing their patient, and financial issues (Abbasi et al., 2020). They may decide to make amends in their daily life routines, business and social lives, take on new responsibilities, or give up previous hobbies, all of which contribute to an emotional effect that causes anxiety and depression (Geng et al., 2018; Govina et al., 2015; Lee Wong et al., 2020).According to Keramatikerman (2020), identified as one of the world’s most fatal diseases, cancer affects millions of people each year. Newly diagnosed cancer patients may face a slew of unknown difficulties, including physical and emotional issues that may impair the quality of their lives and lead to anxiety and problems specifically depression, and other issues. Patients are not the only ones managing health-related issues; families also play an important role in illness management because their time is majorly spent at home supporting clients. The status of a family caregiver is expected to be a supportive individual who is unpaid that provides medical and emotional assistance in addition to disease treatment.They deal with cancer at every stage, including diagnosis, treatment, monitoring, and patient follow-up. According to a research, one-fourth of family caregivers of patients diagnosed with colorectal cancer experience varying levels of stress during diagnostic procedures. Unmet needs such as expenses, the burden of the disease emotionally, side effects of chemotherapy and the treatment process may all contribute to stress. Patients’ spouses are the most likely family caregivers to be significantly affected by cancer, with 38.9% experiencing depression while caring for their partners. One more research found that large amount of time spent caring for cancer patients has a greater effect on female spouses than those of their counterpart because aside from illness, additional tasks are carried on by females at home. Apart from that, the fear of the cancer recurring even after survivorship is evident. This makes their level of strain distress increased than that of patients, which also puts them at a higher chance to suffer from cardiovascular and infectious diseases as a result of stress and a weakened immune system (Keramatikerman, 2020).In the simplest manner, a diagnosis of a certain disease like cancer changes the overall health of not only the diagnosed patient, but also of families and their caregivers. This disease to a person means a pivotal or even life-changing experience that for the whole course of the illness may include distress and other health issues. It is a situation in a patient’s life which alters many aspects of their routines, from roles at the working place, at school if the patient is still a student, and most especially at home. Recognizing these significant changes in someone’s way of living can help them throughout their hardships and provide them assistance when they need it (American Cancer Society, 2022). Not only does cancer scar a patient, it also imposes a burden, economically that is substantially increasing as a consequence of many factors including the expenditure involving caring for a cancer patient. This economic struggle begins right from the moment a person is diagnosed with cancer and is maintained throughout the patient’s disease process (Yabroff et al., 2012).Although, as research suggests, some family caregivers chose the ineffective coping attitude in the form of avoidance isolation and can be classified as emotional actual and biochemical. The preference of the majority still leans on the effective coping attitude identified as religious asylum, seeking external aid, acceptance cognitive restructuring, and active planning. The experience of caring is perceived by these people to be multidimensional. Caregiving can result in positive outcomes such as a boost in affection and intimacy, personal development, improvement of close relationships, satisfaction, social support from others, and self-esteem, as well as negative outcomes such as psychological, physical, emotional, social, and economic issues (Karabulutlu, 2014).Evidence from past scientific efforts suggests that family caregivers of cancer patients experience increased levels of negative emotions and psychological distress, which also includes anxiety and depression. A percentage of 46.5 of caregivers manifest anxiety while depression was found in 42.3% of them, according to Geng et al. (2018). Furthermore, Perez-Ordóez et al. (2016) discovered that anxiety can reach up to 76% among them. It is common for cancer caregivers to employ a variety of techniques when it comes to coping that can lessen or may discard the negative effects of depression and anxiety-causing issues; however, some coping techniques may also exacerbate these same problems (Aydogan et al., 2016).Coping has long been a problem around the world in terms of cancer care. It is the process defined as the management challenges and needs caused by the overall experiences undergone by a person, using behavioral and cognitive efforts to formulate solutions not only to personal dilemmas but also to interpersonal issues, and in the pursuit of stress management and reduction. Coping manages the distress that is brought about by a specific problematic context, through managing issues that cause strain, also by changing the factors that affect stress. Satisfaction is achieved by receiving coping training by which contains learning strategies in coping. As a result, this is evidenced by more efficient approaches in coping. According to research, family caregivers of these patients utilize a variety of techniques in order to cope with the challenges they face (Rachel et al., 2022).As it can affect anyone in the population, cancer is a disease of major concern. In any parts of the world, unfortunately, specific population groups suffer more from the disease and its impacts. This is referred to as cancer disparities. In order to determine these disparities, we will have to consider aspects such as ethnicities/race, age, sex, and socioeconomic status. In the United States, black American men account for the highest rate for cancer cases than that of women in the country amounting to 484.7 per 100,000 men every year. As compared to women accounting for 419.9 per 100,000 women every year. The same research finds that, with the combination of the different aspects, the diagnosis of cancer and death from it leans on men than women (National Cancer Institute, 2015).Focusing on Philippine context, the diagnosis of cancer in liver, lung/respiratory, prostate, colon/rectum, leukemia, and stomach are among the common sites in men. On the other hand, in Filipino women, common sites reported are found in the breast, lung/respiratory, cervix, ovary, colon/rectum, and liver (Department of Health, 2012).According to the Department of Health (2012), it stated that cancer prevalence for both men and women results to 0.3%. It is noted in the publication that this prevalence is elevated in urban areas and occurs greater in higher class populations which was stated to be 0.5% and in the National Capital Region which is 0.5% as documented.Theoretical Framework A fundamental concept connected in this study is Jean Watson’s Theory of Caring. According to Watson (1997), the core of the Theory of Caring is that “humans cannot be treated as objects and that humans cannot be separated from self, other, nature, and the larger workforce.” Encompassing Watson’s theory is the entire field of nursing, emphasizing on the interpersonal relationship between the caregiver and the care recipient. The focus of this theory is on “the centrality of human caring and on the caring-to-caring transpersonal relationship and its healing potential for both the one who is caring and the one who is being cared for” (Watson, 1997). Lower-order biophysical needs, such as the need for food and fluid, elimination, and ventilation, are at the bottom of Watson’s hierarchy of needs. The lower-order psychophysical needs are then addressed, which include the need for activity, inactivity, and sexuality. Finally, there are higher order needs, which are psychosocial in nature. The need for achievement, affiliation, and self-actualization are included in this classification.This study is also anchored on the Transactional Model of Lazarus and Folkman. According to this model, stressful situations are dealt by people by appraisals of stressors and resources. The primary appraisal addresses the individual meaning of the specific stressor, which in this case are the challenges faced by family caregivers. The secondary appraisal examines the individual’s abilities and resources to deal with the situation. Individual coping efforts are employed on this basis to deal with the stressful situation. According to research, caregiver burden typically includes tasks above and beyond assisting with activities of daily living.The consequences of a care situation are determined by the imbalance between the challenges or difficulties encountered and the resources of the family caregiver. Caring for a cancer patient can result in both positive and negative experiences. Caregiving for chronically ill patients may present difficulties for family caregivers. The difficulties that family caregivers go through are frequently overlooked.From a scientific standpoint, the hardships that family caregivers face are a theoretical construct. The Transactional Model of Lazarus and Folkman serves as the conceptual foundation for the assessment of the situation. The subjective evaluation of family caregivers’ experiences is critical for the delivery and improvement of appropriate care.To create an effective discourse, it is necessary to first identify the factors that are central to a person’s stress management and the methods that effectively target these factors. The transaction between people and their external environment is central to the interpretation of stress by Lazarus and Folkman. According to this model, stress may not be a stressor if the person perceives the stressor as positive or even challenging rather than a threat. Furthermore, if the person possesses or is capable of using adequate coping skills, stress may not be a result of or developed as a result of the stressor. As proposed by the model, people can be taught to manage their stress and cope with their stressors. They may learn to alter their perception of the stressor, giving them the ability, strength, and confidence to improve their respective lives and deal with all types of stressors. Stress can result from both negative and positive stressors. The severity and duration of stress vary according to the circumstances and emotional state of the person experiencing it.Objectives of the Study The purpose of this narrative study was to investigate and understand the challenges faced by family caregivers of cancer-diagnosed patients. In this research, challenges of the family caregivers will be generally defined as problems and issues that interfere with the quality of care or ability to achieve goals in caring for the cancer patient. Specifically, it aims the illumination of the following: First, what are the family caregiver’s demographic data and the patient’s medical profile; second, what are the challenges faced by the family caregiver in caring for the patient with cancer; third, how does the challenges affect the family caregiver’s lifestyle and outlook in life; and lastly, how does the family caregiver cope with the existing challenges.Limitations of the Study The present study was conducted on Filipino family caregivers of cancer patients, regardless of ethnicity and religion, residing in SOCCSKSARGEN region. The results cannot be generalized to caregivers from other nationalities and residents outside the region or to other informal caregivers. Repeating the study on these said groups can help identify context-appropriate coping strategies and the factors influencing them among caregivers and therefore enable the caregivers to provide better patient care and improve quality of life both for themselves and for their patient.
2. Methodology
- This section focuses on presenting the research design, role of the researcher, research participants and materials, data collection, and data analysis utilized in the study.Research DesignThis research employed the qualitative phenomenological research design utilizing adapted interview questionnaire technique. The definition of phenomenological study is the approach a researcher takes as means to do an exploration of what people have experienced and how they understand a phenomenon. It is utilized as a form of analysis of the lived experiences of people in the world and to explain the behavior, motivations, and characteristics of people and situations in a target group. This design was used since the study’s purpose was to determine the respondents’ experienced challenges in caring for patients with cancer, how it affected them, and their way of coping with those difficulties.Role of the ResearcherIn the conduct of the study, the researcher attempted to access the thoughts, feelings, and experiences of the participants. It proved not an easy task for the researcher, as it involved asking the respondents to talk about things that were very personal to them. The researcher set aside biases, explicate beliefs, and personal opinions. Securing consent was given by the participants and assured them of confidentiality of information collected and established rapport to acquire trust and in-depth communication.Research Participants and MaterialsThis research study focused on determining, exploring, and understanding the difficulties and challenges experienced by family caregivers of cancer-diagnosed patients in order to profoundly comprehend contexts of care especially in complex cases. Participants were residents of SOCCSKSARGEN region in the Philippines, a family caregiver of a patient with cancer, equally male and female, regardless of sexual orientation, of good mental status, and consent was fully considered. The researcher included a total number of 7 participants, coming from any province in the region. It was considered that the family caregiver’s patient is diagnosed in the III or IV stage of cancer, any cancer types, regardless if the cancer-diagnosed patient was living or deceased. The study utilized an adapted questionnaire that was self-administered by the researcher to the respondents. A one-on-one interview was arranged consisting of open-ended questions that probed the respondents’ experiences which were answered truthfully and with informed consent by the participants.Data CollectionThe respondents were selected using purposive sampling technique from bona fide residents anywhere in SOCCSKSARGEN region.The researcher first obtained an approval from the Program Chairman of Bachelor of Science in Nursing to commence the research study in the locale. After determining the participants, an informed consent was given to them stating the purpose, goal, and nature of the study with the researcher tending to every question of the participants. A one-on-one interview was arranged by the researcher consisting of questions which were answered by the participants. Each interview lasted for an hour and a half through videoconference and was conducted during the months of June to July. The researcher met the participants once or until sufficient data was gathered. Afterwards, the data collected was analyzed using thematic analysis. All materials, methods, and data gathered were subject for scrutiny to obtain approval from the research ethics board. In the course of the one-on-one interview as the mode of data collection, an informed consent was obtained and secured in accordance with the Data Privacy Act of 2012 otherwise known as Republic Act No. 10173, thus maintaining confidentiality.Ethical ConsiderationsEthics refer to governing moral principles which influences the behavior of a person or the conducting of an activity. In order to adhere to the ethical standards of research throughout the duration of the study, the researcher followed appropriate steps.Before the conduct of the study, the participants were made fully aware and informed of the background and purpose of the research they are participating into. A voluntary informed consent was obtained containing additional information as to the benefits, risks, and expected outcomes of the study. The informed consent letter contained adequate information and emphasized on the participant’s choice on whether or not to enroll in the study. The letter also provided assurance to the participants that no human rights shall be violated, their privacy upheld all of the time, identities and interview answers remain confidential throughout the research study.Conflict of Interest. The conduct of this study upheld the highest ethical standards and credibility. The researcher made sure there are no conflicts of interest throughout the research study. The researcher was responsible for all expenses spent throughout the study. Informed Consent Process. In this study, participants were given the freedom to participate or decline after the researcher has adequately provided all relevant information related to the study, its purpose, and method of collecting data. An informed consent form was obtained after a thorough explanation of the research has been provided. In the informed consent formed contained necessary information relevant to the study and the participant’s cooperation in the research. It stated that the participation is voluntary and the participants were given the time to decide and ask questions to the researcher.Confidentiality. In line with this, everything the participants provide in the conduct of this study such as interview answers and/or records will be kept confidential. Any information obtained related to the participants and the patients with cancer will remain private, only the researcher and the participants have access to in the exception of the events which prove significant of protecting the participants’ rights and welfare.Potential Risks, Adverse Events and Discomforts. Along the course of the interview, the participants may feel discomfort and feelings of sadness brought about by the sensitive nature of the topic. If the participants feel the questions being asked towards them make them feel uneasy, uncomfortable, or bring to them emotional distress, the participants have the right to reject answering and withdraw from the study. This study emphasizes the participant’s welfare and dignity throughout the study.Potential Benefits to Participants, Respondents, and/or to Society. As a result of the endeavors of this study, the struggles being faced by family caregivers caring for cancer patients will be profoundly understood, thus, opportunities for better policy making in government will be realized, betterment of providing services and care in the nursing profession, newfound information that may be incorporated in the education of nurses, and acceptance and empathy in our society.Participation / Withdrawal of Participants / Respondents. The participant’s participation is voluntary. Their refusal to participate will involve no penalty or loss of benefits to which they are otherwise entitled. The participant may withdraw his/her consent at any time and discontinue participation without penalty. They are not waiving any legal claims, rights or remedies because of your participation in this research study.Data AnalysisThe data gathered and utilized were analyzed using thematic analysis to arrive at main themes exploring the challenges faced by family caregivers in caring for cancer-diagnosed patients. The socio-demographic details were presented in a table format showing the participants’ and patients’ relevant personal data.Thematic Analysis’ accessibility and flexibility makes it an increasingly convenient and popular analysis of qualitative data (Braun & Clarke, 2006). In the course of the analysis, the researcher first had a familiarization of the data collected from which generation of initial codes will originate. The researcher probed on relevant information using inquiries of their personal data, lived experiences, and how they managed through the adversities. Afterwards, themes contained in the data were determined and reviewed extensively by which were defined at the last part of the analysis. From the raw data arose codes that were later grouped and identified as themes that explained and answered the study’s queries. This method places emphasis in the identification, analysis, and interpretation of patterns contained within the qualitative form of data.ValidityIn this study, validity and reliability of the study were examined thoroughly by the researcher and the criteria suggested. To establish credibility, the researcher has had adequate cooperation and engagement with the participants. Reviews were implemented by the help of the research adviser and the adviser’s additional comments were also used. The researcher checked the dependability of the data through performing activities such as consultations with the research adviser for material review. Confirmability had been done by diminishing, as much as possible, all presumptions and prejudices. The findings’ validity was also verified by the study’s participants.
3. Results and Discussion
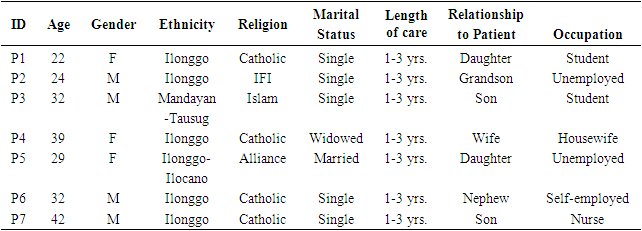
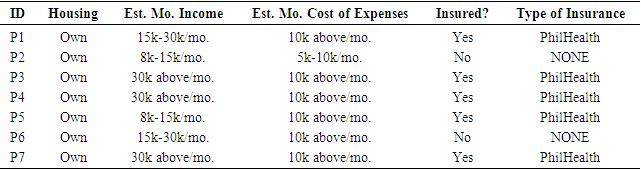
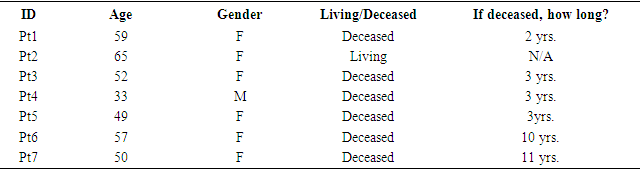
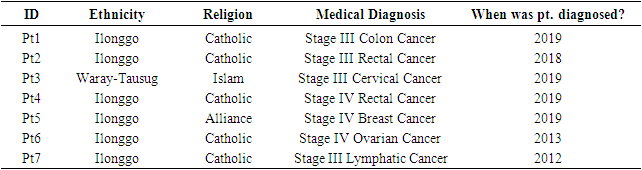
- This chapter focuses on presenting the results synthesized following the conducted one-on-one interviews with the participants. This part includes presenting the findings of the interviews, the themes with which emerged from those accounts, and discussions of each related topic. Also, this chapter offers a description of the obtained results of the study. Throughout the conduct of the interviews, the participants of the study were freely given the choice to converse their thoughts, experiences, and insights in the language of their preference or what we refer to as ‘mother tongue’. In accordance with the aims outlined in this research, the results of each research question are further discussed.The sociodemographic characteristics of the interviewed family caregivers are described first, followed by the medical profile of patients diagnosed with cancer, and thereafter the results and themes of the succeeding research questions are presented. In this current study, there are eight (8) emerging themes identified; Physical Burden, Psycho-emotional Burden, and Spiritual Crisis transpired from the experienced challenges of family caregivers; Significant Human Relationships, Changes in Lifestyle, and Spiritual Coherence came up in exploring the outcomes of caregiving in their lives; and Active Coping, and Social Support as the family caregivers’ coping mechanisms in the context of caring for the patient with cancer.Socio-demographic CharacteristicsThe sociodemographic characteristics of the participants and the profile of the patients diagnosed with cancer were gathered through the one-on-one interviews with the aid of the semi-structured questionnaire. The data gathered in this section rightfully contribute to the analysis of the results of this study. The sociodemographic details of the interviewed participants are separated from that of the details of the patients with cancer and are discussed further in this section. In this part, the researcher put into account significant information pertaining to the context of care of family caregivers such as length of caring for the patient, the estimation of expenses at the period of care, and the membership of the patients in any insurance plan. Also, the cancer patients’ demographic details and medical profile are laid out to identify their diagnosis, when were they diagnosed, and other pertinent data.Socio-demographic Details of Interviewed Family Caregivers. Of the 7 participants in this study, 4 of the family caregivers were male and 3 were female. The majority of the participants range from the ages 22-32 years old which accounts for 5 of the family caregivers. The remaining 2 participants age from 39-42 years of age. The youngest participant was 22 years old and the oldest participant in the sample was 42 years old. With regards to their ethnicities, 5 family caregivers are Ilonggo, while 1 participant as Ilonggo-Ilocano, and the other 1 identify as Mandayan-Tausug. In the aspect of religion, among the 7 family caregivers, 4 are Roman Catholics, 1 is a member of the Iglesia Filipina Independiente (IFI), 1 participant belong to the Islam religion, and 1 participant belonging to the Alliance Church. Pertaining to their marital status, 5 participants are single, 1 participant is married, and 1 is widowed. The sample consisted of 3 individuals who are unemployed, 2 participants reporting they were still a student at the time of rendering care to the patient, 1 participant was self-employed, and 1 was employed as a nurse. Aside from the role of being a caregiver, 4 family caregivers are children of the cancer patient, 1 participant is the patient’s grandson, 1 participant being the patient’s wife, and 1 participant is a nephew. Upon investigation, all 7 participants involved in this study cared for the cancer patient in a span of 1-3 years. At the time of the illness and its progression, both the family caregiver and the care recipient lived under the same home. All of the participants (7) stated that they own the house they live in.Having to juggle work and life situations is no easy task for family caregivers especially that they are faced with a daunting challenge in caring for a cancer patient. As discussed in the study of A. Fuchsia Howard et al. (2022), deciding on whether to seek or revamp their employment or stay unemployed to focus solely on caregiving can result to a sense of loss or grief. This situation does not entail a voluntary choice or move for the family caregivers but rather a decision mostly considering the welfare of the terminally-ill patient. In the study’s sample, most participants committed to the service of providing care to their loved ones diagnosed with cancer.Among 7 participants, 3 reported to have an estimated monthly income of 30,000 and above, 2 individuals were earning 8,000 to 15,000 per month, and 2 participants with a 15,000 to 30,000 income. With the diagnosis of the patient with cancer came the cost of treatment and other necessities for the patient, majority or 6 participants estimated that they spent 10,000 and above for expenses every month, with only 1 reporting they spent only between 5,000 to 10,000 every month. With this, cancer patients of 5 family caregivers had health insurance specifically PhilHealth.The emergence of financial struggles may come from expenses in treatment and other necessities that are not covered under government universal health care assistance or private insurances. According to Abrams et al. (2021), indirect costs that may involve transportation and living expenditures contribute to the escalating expenses and in turn these situations offer burden and somehow distress to many families. Enrolling the patient into an insurance plan may alleviate costings, which in this study, proved worthy for family caregivers in supporting them amid financial hurdles.
|
|
|
|
|
|
|
4. Conclusions and Recommendations
- The results of the study revealed that family caregivers undergo various challenges in context of caring for the cancer-diagnosed patient. Upon investigation of the participants’ statements and answers in the interview, family caregivers go through classified burdens that affect not only their physical aspect but also their psycho-emotional health. Participants were able to share details of their difficulties that was intertwined with the acceptance of the caregiver role. It also manifested issues in regards to their spirituality. During the course of the care process, participants reported to have questioned their faith and the patient’s chance of improvement. In retrospect, their challenges brought about exhaustion that resulted in alterations in health and routine.The research also probed on the outcomes of the caregiving process and role towards the family caregiver and the data showed that the burden of caregiving had a toll on the participants’ well-being. This pertained to significant changes in the body such as weight, stress, and mood issues. This implies that family caregivers experienced significant exhaustion from the caregiver role. Exhaustion can change many aspects of daily living and it manifested through breakdowns, feelings of extreme sadness, regret, and a period of being hopeless. One of the driving forces for these family caregivers to handle the role is pity, love, and debt of gratitude. They are willing to be involved in any task if it means the welfare of their patients. However, caregiving had not only brought negative results but also positive outcomes on the individuals. Improvement and coherence in one’s spirituality, fortified relationships arose since the beginning of the caregiver role. The support of family caregivers will inevitably create consequences in the quality of care being provided to the patients as this is also critical in the trajectory of the disease. Caregiver burden not only decreases quality of life for caregivers but also indicate a sense of loss of control over their lives.As the synthesis of the study, family caregivers utilized different coping strategies or techniques in order to maneuver themselves in situations. These mechanisms allowed them to surpass the difficult challenges and made them stronger over time. They maintained a positive outlook in life, properly planned their tasks, and also got help from support networks around them which included their families, friends, and the community.It is significant for qualitative researches that address the caregiver aspect of care to flourish and get published so that further measures and programs are crafted so that their welfare will be upheld. Based on the findings and conclusion of the study, the following are recommended:1. The initiation of support groups for family caregivers caring for patients with cancer that will cater their emotional needs and will involve focus group discussions which let caregivers express their experiences with a goal of alleviating suffering, pain, and distress.2. Planning to include and cater family caregivers strained of caregiver burden in therapy sessions that will further aid them in molding a productive outlook at their situations and thus preventing any adverse consequences of exhaustion. 3. Institutions such as the government or any private organization, may it be through a public-private partnership should establish a Cancer Resource Center for one of the purposes of caregiver support and patient assistance.4. Nurses and other concerned authorities should initiate for the education, crafting, and implementation of programs that will uphold the status of family caregivers. These could be through programs honing the skills of potential individuals for caregiving.5. The stern advocacy of a national agenda to develop, fund, and implement inclusive health policies that covers cancer care not only for the provision of the patients but the inclusion of the family care provider. 6. The public’s awareness should be increased for them to be able to comprehend and empathize with family caregivers and their cancer-diagnosed patients. These can be done through cancer and cancer care seminars conducted in the community setting.7. Future researchers must be staunch promoters on understanding the scope of cancer care through the conduct of more studies.
ACKNOWLEDGEMENTS
- This research paper was realized through the constant support, invaluable assistance, and undying motivation of everyone with whom were involved in the drafting of this study, including dear friends, parents, mentors, participants, and the researcher himself. The researcher wishes to extend his acknowledgement and express his gratitude and dedication towards the following individuals for their contributions to the successful completion of this thesis:To Ma’am Jainah Rose F. Gubac, PhDNS, MAN, RN, for being the researcher’s thesis adviser, for dedicating her time, patience, and diligence throughout the process of the study. Most especially, for enlightening the researcher with her wisdom and expertise in carrying out important tasks of this research.To Ma’am Jza A. Taposok, MAN, RN, Ma’am Lalyn N. Cabauatan, MAN, RN, and Ma’am Marchie Lou C. Ereje, MAN, RN, for their kind assistance particularly their considered efforts and advice.To Ma’am Dahlia S. Arancel, MD, DPBA, FPSA, PhD, and other members of the College of Medicine and Allied Health Sciences faculty and administration, for the earnest approval of the conduct and completion of this research study.To Honey Lyn M. Loria, GJ Pauline L. Buhayan, and Angeline C. Gonzales, the researcher’s friends, for journeying with the researcher throughout various stages of the study and for boosting his morale. To Marianne L. Yuayan, Carl Michael P. Quidato, and Lovely Alexi L. Dolormente, for their commitment in assisting the researcher during the conduct of the study. The researcher values your time and effort.To the cancer-diagnosed patients and their family caregivers, for allowing the researcher to create discourse with them and for being the core element of this study. This endeavor would not be fulfilled without their unrelenting support and cooperation.To Mama Mae Joy A. Gecosala and Papa Reynaldo A. Gecosala, the researcher’s beloved parents, for always having his back and the constant reminders and unconditional love they gave during the labor-intensive hours spent on this study. Truly, they have been incredible research assistants.To the Almighty God, above all, who continues to shower the researcher with His abundance and mercy, and guidance throughout the journey. His infinite wisdom and loving presence keep the researcher on the right path.