-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2023; 13(2): 53-59
doi:10.5923/j.nursing.20231302.02
Received: Sep. 17, 2023; Accepted: Sep. 30, 2023; Published: Nov. 23, 2023

Health Education Intervention and HIV/AIDs Prevention Behaviours among Young People in Calabar Metropolis, Cross River State, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLImmaculata Etim Bassey 1, Elizabeth Edem Okon 1, Idode Mercy 1, Okutepa Eleojo Toyin 1, Akaba Felicia Bosede 1, Bassey Emmanuel Etim 2, Effiom John Edwin 3
1Department of Nursing Science, Faculty of Basic Medical Sciences, Igbinedion University, Okada
2Department of Emergency Medicine, Faculty of Emergency Medicine, Medicine and Health, Whiston Hospital, Prescot, United Kingdom
3Department of Social Science Education, Faculty of Arts and Social Science Education, University of Calabar, Calabar, Nigeria
Correspondence to: Effiom John Edwin , Department of Social Science Education, Faculty of Arts and Social Science Education, University of Calabar, Calabar, Nigeria.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Aim: This study investigated health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria. One purpose of the study was stated and to achieve the purpose of the study. One research question was formulated, which was converted to one statement of hypothesis. A literature review was carried out based on the variable under study. Method: The survey research design was considered most suitable for the study. A stratified random sampling technique was adopted in selecting 327 respondents used as sample for the study. A validated 20 items four-point modified Likert scale questionnaire was the instrument used for data collection. The face and content validity of the instrument was established by experts in Test and Measurement and Evaluation. The reliability estimates of 0.85 of the instruments was established using the test-retest method. Simple linear regesiion statistical tool was used to test the hypotheses formulated for the study. The hypothesis was tested at 0.05 level of significance. Results: The results obtained from the data analysis revealed that health education intervention significantly influences HIV/AIDs prevention behaviours among young people in Calabar metropolis of Cross River State Nigeria. Conclusion: Based on the findings of the study, it was concluded that health education intervention significantly influences HIV/AIDs prevention behaviours among young people in Calabar metropolis of Cross River State Nigeria. Therefore, it was recommended, that continuous health education programs and seminars on HIV prevention practices be organized by NGOs, and Ministries of Health within the motor parks for the drivers, to inform the drivers and equip them with skill to protect them from the infection.
Keywords: Health Education interventions, HIV/AIDs prevention measures, Condoms, Abstinence
Cite this paper: Immaculata Etim Bassey , Elizabeth Edem Okon , Idode Mercy , Okutepa Eleojo Toyin , Akaba Felicia Bosede , Bassey Emmanuel Etim , Effiom John Edwin , Health Education Intervention and HIV/AIDs Prevention Behaviours among Young People in Calabar Metropolis, Cross River State, Nigeria, International Journal of Nursing Science, Vol. 13 No. 2, 2023, pp. 53-59. doi: 10.5923/j.nursing.20231302.02.
1. Introduction
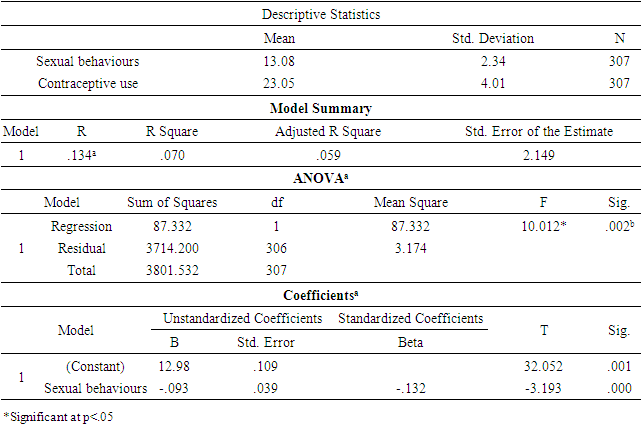
- The Human Immunodeficiency Virus (HIV) is the root cause of Acquired Immune Deficiency Syndrome (AIDS). Since the first instance among homosexuals was identified in 1981, this disease has grown to be the biggest epidemic now affecting humanity (Idoko, 2014). The virus has infected more than 60 million people worldwide, and an estimated 40 million of those people are currently infected. The majority of infections in the globe, including those in Africa, are brought on by HIV type 1. However, AIDS is increasingly being brought on in Africa by HIV type 2, according to the National Institute of Medical Research (NIMR) (2015). These viruses' negative impact on helper cells causes cellular immunodeficiency illness, which makes the patient vulnerable to a wide range of diseases and cancers.Without regard for race, age, or gender, the sickness has spread throughout the entire planet. Additionally, it has spread beyond the "at risk group" to impact the entire populace. It is the fourth leading cause of death globally and is prevalent in Sub-Saharan Africa. Although contact with blood and blood products can also spread the disease, sexual contact is the most prevalent method of infection. Most HIV infections in poor nations happen in young adults, and over half of people living with HIV/AIDS today are between the ages of 15 and 24. Although they are the country's future, young people frequently embrace life styles and behaviour that have long-term effects. Among the risk behaviours that put people at risk for HIV and other Sexually Transmitted Infections (STIs), as well as unintended pregnancy, are sexual conduct, drug addiction, alcohol consumption, and tobacco use (Pathfinder International, 2015).Drug, alcohol, and tobacco use have an impact on their self-control, which makes it harder for them to negotiate sexual activity. The inability of young people to assess risk appropriately when presented due to restricted access to reliable information and competent medical care are other variables that increase their susceptibility to these actions. After South Africa and India, which have the highest numbers of persons living with HIV/AIDS, Nigeria has the third-highest estimated number. According to estimates, nearly 20% of HIV/AIDS patients in SSA reside in Nigeria. More than one in twenty people in the general population are affected by the epidemic, which is also the top cause of mortality in the nation and has claimed over 850,000 lives. As of 2005, 300,000 individuals had just contracted the virus, making up an estimated 2.9 (1.7–4.2) million persons who were sick. According to Harries, Maher, and Graham (2014), the estimated prevalence rate in that year was 4.4% as opposed to 5.4% and 5% in 2004 and 2003, respectively.Zone-specific variations in prevalence range from 3.3% in the Northwest to 7.7% in the South-South zone. According to Umar (2016), some states, including Cross River (12.0%), Benue (9.3%), Adamawa (7.5%), and Akwa Ibom (7.2%), had prevalence rates that were greater than the national prevalence estimate. For people between the ages of 25 and 29, 20 to 24, and 15 to 19 years, the age variation is 5.4%, 5.6%, and 4%, respectively. The disease has a severe effect as evidenced by the decline in Life Expectancy (LE), which fell from 53 years in 1990 to 45.5 years in 2002.The current LE would have been 57 years without the epidemic, and it might have increased to 62 years by 2015 and 70 years by 2025, respectively. Young people, who make up 20% of Nigeria's population and have the capacity to contribute to the growth of the nation, are experiencing a rapid spread of the infection.Assuming a 10-year incubation period, these young persons will pass away in their early to mid-thirties given that HIV/AIDS infections in Nigeria primarily affect people in their early to mid-twenties. These fatalities will undoubtedly lead to the loss of human capital that can be used to produce goods and services, which will have a detrimental impact on the productivity of many industries in the nation, including agriculture and education, as well as the already fragile health sector. The cost of chronic illness has an impact on each family member, their employers, the community, and the country as a whole. HIV/AIDS will result in a decrease in revenue output and an increase in expenditures at the workplace. This is a result of the rising costs of healthcare, burials, training, and hiring new workers to take the place of the sick and deceased. The illness gradually claims the lives of parents, kids, young people, potential leaders, and wage earners, resulting in a loss of the present and future labour force and impoverishment at all levels. The United Nations General Assembly Special Session (UNGASS) declaration on commitment on HIV/AIDS from 2001 placed the fight against HIV/AIDS among young people at the forefront of the global response (Federal Ministry of Health, 2018).Over 8% of young people in places including Cameroon, Central Africa, and Sierra Leone lacked enough awareness about HIV, according to UNICEF, UNAIDS, and WHO (2011). Only 1% of Somalian girls knew how to prevent contracting the sickness, and only 25% of girls had heard of the illness (Christian Aid, 2013). Only 9% of Ukrainian females could properly name the three main prevention methods for sexual transmission, despite the fact that nearly all of them (99%) had heard of AIDS. Only 37% and 33% of young people in India and Bangladesh, respectively, had ever heard of HIV or AIDS (Christian Aid, 2013). According to a survey conducted in 17 countries, more than half of the teenagers polled were unable to name even one way to protect oneself from HIV/AIDS (NFPA, 2016). In Mozambique, 62% of boys and 74% of adolescent girls were uninformed of at least one method of HIV prevention. In Nigeria, a pilot research among adults and youth in the southwest of the country revealed that 91.4% of respondents had a high level of knowledge about HIV/AIDS (NFPA, 2016).Another research of secondary school students in Delta State found that the majority (94%) of participants knew a lot about HIV/AIDS (Obro & Tabowei, 2016). A study of teenagers at five Lagos-area schools revealed that 76% of them had heard of AIDS, 36% thought HIV could be spread through kissing, and 20% didn't think it could be spread through sex. Similar findings were found in a study conducted in a tertiary institution in Ile-Ife, which showed respondents with high levels of sexual activity had acceptable understanding of HIV/AIDS. On the other hand, investigations conducted at the national college among secondary school students in various sections of the nation showed that before to intervention, there was a lack of information concerning HIV/AIDS.Despite the significance of health education to Calabar Metropolis citizens, study studies and articles have produced conflicting findings, with some claiming that young people have great knowledge of HIV/AIDS while others claim that they have low knowledge. It is based on this problem that this research examined health education intervention and HIV/AIDS prevention behaviours among young people in Calabar Metropolis, Cross River State, Nigeria.Statement of the problemIn terms of sickness and mortality, HIV/AIDS is one of the deadliest infectious illnesses in the world. It was projected that 4.3 million people globally contracted the virus for the first time in 2006. With a range of 34.1-47.1 million, this takes the average number of individuals living with HIV/AIDS at 39.5 million. In that same year, the illness claimed the lives of an average of 2.9 million individuals. More than 10 million of the almost 40 million individuals living with the virus—3.9 million men and 6.2 million women—are between the ages of 15 and 24. This information showed that young women face substantially greater risks than their male counterparts, which may be due to an imbalance in the power between the sexes. This is the outcome of adverse cultural norms, a lack of access to education or personal money, which furthers the status of women as lower status individuals and increases their susceptibility to HIV/AIDS.About 2.5 million new HIV infections occur each year, with young people accounting for half of all new infections. throughout 7,000 young people throughout the world get the virus daily, with one young person becoming infected every 15 seconds on average. The epidemic is most prevalent in underdeveloped nations, where around 85% of these young people reside.Unfortunately, this age group has significantly greater rates of unprotected sexual activity, unexpected pregnancy, and STIs. Therefore, the significant rise in infections and mortality in this economically active age group would have a negative impact on the country's social and economic growth. Young individuals are especially at risk of getting HIV since the heterosexual mode of transmission is responsible for 90–95% of HIV infections in Nigeria. numerous sexual partners, the presence of another sexually transmitted illness in either partner, the use of psychotropic drugs, and having numerous partners are all risk factors for this infection. The increased risk of exposure for young people is a result of their frequent ignorance of HIV/AIDS. Furthermore, they might not be aware of how susceptible they are to the infection, how to prevent it, or have restricted access to preventative measures. This population's awareness of HIV/AIDS serves as a gauge for the effectiveness of the Millennium Development Goals (MDGs), which were adopted at the September 2000 Millennium Summit. The promotion of voluntary counselling and testing (VCT) and expanding intervention to young people were two additional tactics that programme directors should take into account when determining if they would ever attain the 2003 National Policy Goal and the international obligations set out by UNGASS and the MDGs. Many young individuals who attend higher institutions live apart from their family and might not have enough money for necessities. They are more likely to engage in dangerous sexual behaviours as a result, frequently with several partners. They have a great urge to experience as youngsters as well. They are at risk of contracting HIV/AIDS because of all these variables. Additionally, a lot of young people continue to hold harmful misunderstandings about HIV/AIDS. The morbidity and mortality brought on by HIV/AIDS must be reduced, and young people must be given the information they need to make educated decisions. Adoption of safe behaviours should include receiving accurate information about HIV infection. It is anticipated that their peers would be inspired to make safe decisions if they are provided with enough and reliable information. If they do this, they may develop into peer educators and educate other young people.UNAIDS, the United Nations Special Programme on HIV/AIDS, has indicated that nine out of ten people living with HIV throughout the world are unaware of their status. This is so because many of the afflicted individuals are still in good health and have never deliberately sought counselling or undergone testing. VCT aims to stop additional HIV transmission and is a significant gateway to education. But many young people either don't have access to VCT facilities, or even if they did, they could be unwilling to test or seek treatment out of concern about stigmatisation and prejudice. The services can also be excessively pricey, ugly, or hostile for them. It is based on this problem that this study assessed the influence of health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria.Purpose of the studyThe purpose of the study was to examine the influence of health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria.Research questionsWhat is the influence of health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria.Statement of hypothesisThe hypothesis states thus, there is no significant influence of health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria.
2. Materials and Methods
- Experimental setting The research method used was a survey. A research design is utilised, in accordance with Salaria (2012), when the aim of a survey is to collect and assess data on the phenomena under study from a representative of the whole population with the intention of generalising the findings to the entire population.Area of the studyThe study area, Calabar Metropolis, is in the southern portion of Nigeria's Cross River State, where it serves as the state's capital. Between latitudes 4 50'N and 5 10'N and longitudes 8 17'E and 8 20'E, it includes Calabar Municipality and Calabar South Local Government Areas. It is bordered to the east by Akpabuyo LGA and to the north by Odukpani LGA. The Great Kwa River to the east and the Calabar River to the west encircle Calabar Metropolis. The current urban area is located on the Calabar River's eastern bank. Mangrove wetlands impede its development in the southern portion. It is thought to occupy a land area of around 274.593 km2. According to Inyang (1980), Calabar has a tropical equatorial (Af) climate with high yearly rainfall, high temperatures, and high relative humidity. The mean annual average temperature is 26.1 C, and there is 2750 mm of annual rainfall. The population of the study region, which was believed to be 10,000 in pre-colonial times, increased dramatically from 328,876, in 1991, to 99,352 in 1993. The population was estimated at 371,022 people in the most recent census in 2006 (National Population Commission (NPC) [Nigeria], 2006). Calabar's physical bounds have expanded in tandem with its population increase. This expansion of the physical borders means a proportional reduction in the amount of land and vegetation in the region, which has an immediate effect on the microclimate (Eni, & Ukpong, 2014).Participants/sampling technique/Sample62,098 male and female juveniles from the Calabar municipal and Calabar South Local Government Areas made up the study's population (participants). A stratified random sampling strategy was employed in the investigation. Each Local Government Area has its own stratum, from which respondents were picked. 310 respondents, representing 5% of the Local Government Areas, made up the sample for the study. Instrument for data collectionTo achieve the purpose of the study, the researcher used survey questionnaire tagged “Health Education Intervention and HIV/AIDs prevention behaviour Questionnaire” (HEIHAPBQ) to capture data for the study. This instrument was developed by the researcher. The survey questionnaire has three sections: personal data of respondents (Section A), Health Education Intervention (Section B), and HIV/AIDs Prevention Behaviour (Section C). Information sought in Section A were sex, age, educational level, location and marital status. To obtain data for this hypothesis, respondents were asked to use a scale of 1 to 4 to respond and the scale used is interpreted as 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. i.e this instrument consists of 15 items (statements) which were attached to a four-point Likert scale ranging from “strongly agree” to strongly disagree” as pivotal point of the scale. Moving from “strongly disagree” to “strongly agree”, positive items were scored from 1 to 4, respectively, while negative items were scored in the reverse order.Validity and reliability of the instrumentTwo university lecturers who specialise in measurement and evaluation, along with a health professional, were tasked with carefully reviewing and evaluating the instrument for its relevance, content, face, and construct validity in order to ensure that it measures what it is intended to measure. A few of the components in sections B and C were to be eliminated at the advice of the experts, while others were to be added to the instrument. Two things (in Sections B and C) were ultimately deleted, while two others were changed. They underwent a reliability test as well, which showed extremely excellent evidence of data consistency. After that, data from a pilot research involving 40 teenagers in the Akpabuyo Local Government Area who were not study participants gave information for the instrument's subsequent validation and reliability assessment. The purpose of the pilot test was also to determine if it would be possible to collect the necessary data using the instrument. The instrument was readable, according to the pilot study's findings, and after using the spearman-Brown correlation approach, the Cronbach reliability method produced a reliability coefficient of 0.85 for the instrument.Data Collection Data for the study were collected with the aid of the questionnaire. The questionnaires were distributed to the youths in Calabar metropolis who were between the ages of 14 to 29 years. The services of one research assistant were requested to facilitate in the distribution of the questionnaires. The 307 distributed questionnaires were collected from the respondents as soon as they finished with their responses out of 310 questionnaires that were administered.Ethical ConsiderationThe respondents were informed that participation in the study was completely voluntary and that opting out would not have any negative consequences. Oral consent from the person was required in order for them to be a study subject. The goal of the study, as well as any prospective benefits, were explained to the responders. Subjects were made aware of the importance of data confidentiality, privacy, identification, voluntary engagement, and the choice to decline research participation. If the participant elected to quit the study before or during the conclusion of data collection, they were notified of the withdrawal procedures.Statistical tool for data analysisTo answer the research questions addressed in this study, mean and standard deviation analyses as well as item-by-item analyses were used. The influence of health education intervention on HIV/AIDs prevention behaviours among young people in Calabar Metropolis of Cross River State Nigeria was examined using simple linear regression statistical technique.
3. Results
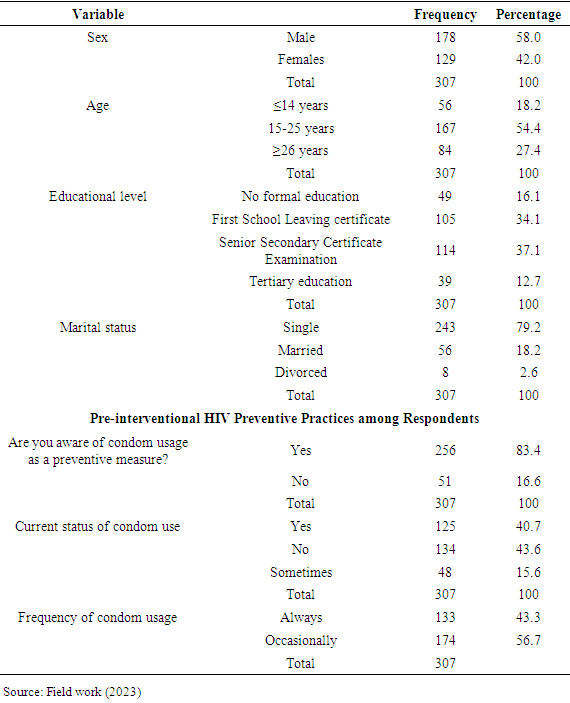
- Out of the 307 respondents included in the study, the demographic data showed that 129 respondents, or 42.0 percent of the total, were female and 178 respondents, or 58.0 percent, were male. This outcome is shown in Table 1. These results showed that there are more men than females in the studied region. A closer look at the results' age distribution showed that, of the 307 respondents, 56 (18.2) were 14 years old or younger, 167 (54.4) were in the range of 15 to 25 years old, and 84 (27.4) were 26 years of age or older. Further, the results of respondents' educational backgrounds showed that, of the 307 respondents, 49 (16.1) have no formal education, 105 (34.1) have completed their FSLC, 114 (37.1) have completed their SSCE, and 39(12.7) have completed their higher education. The results also showed that 243 (79.2) people are single, 56 (18.2) people are married, and 8 (2.6%) people are divorced. In terms of respondents' pre-interventional HIV practises, 256 (83.4%) agreed and 51 (16.6%) disagreed that they are aware that using condoms as a preventative step is a good idea. Out of 307 respondents, 125 (40.7) agreed, 134 (43.6) disagreed, and 48 (15.6) said using condoms should be an option. Finally, 133(43.3) and 174(56.7) stated that they regularly and infrequently use condoms, respectively.
|
|
4. Conclusions
- The study's findings led to the conclusion that health education interventions had a considerable impact on young people's HIV/AIDS preventive practices in Nigeria's Cross River State capital city of Calabar. Following the health education intervention, there was a noticeable rise in condom use along with a decrease in hazardous behaviours including having several sexual partners and using CSWs.
5. Recommendations
- Based on the study's findings, it was advised that NGOs and Ministries of Health organise ongoing health education programmes and seminars on HIV prevention techniques for the drivers within the motor parks in order to inform the drivers and give them the knowledge and skills they need to protect themselves from the infection.