-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2021; 11(3): 49-55
doi:10.5923/j.nursing.20211103.01
Received: Jun. 27, 2021; Accepted: Jul. 19, 2021; Published: Aug. 15, 2021

Provider Related Factors Influencing Satisfaction with Prevention of Mother to Child Transmission Services among HIV Positive Postnatal Mothers Attending MCH/FP Clinic in EL5H, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLLeah Njeri Mureithi1, Sherry Oluchina2, Dainah Kariuki2
1School of Nursing, Jomo Kenyatta University of Agriculture and Technology and Embu County, Department of Health, Kenya
2School of Nursing, Jomo Kenyatta University of Agriculture and Technology (JKUAT), Kiambu, Kenya
Correspondence to: Leah Njeri Mureithi, School of Nursing, Jomo Kenyatta University of Agriculture and Technology and Embu County, Department of Health, Kenya.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Fulfilment of patient/client needs and desires through the delivery of health care is perceived as satisfaction. Client satisfaction has been seen to influence whether a person seeks Prevention of Mother To Child Transmission (PMTCT) services, adhere to treatment and maintain an enduring relationship with practitioners. To establish provider related factors influencing Human Immunodeficiency Virus (HIV) positive postnatal mother satisfaction with PMTCT services a facility based cross-sectional study was used for both qualitative and quantitative data. Data was analysed through cross-tabulation, chi-square correlations and logistic regression model. 91.0 percent response rate was achieved and considered satisfactory in generalizing the study findings. Majority of the respondents, 93.7% were highly satisfied with provider factors regarding the seven services offered at EL5H. However, 0.9% and 5.4% of the respondents reported dissatisfaction and neither satisfied nor dissatisfied with provider factors respectively. Cross tabulation showed that, majority of the respondents were dissatisfied with; waiting time (17.6%), male involvement (13.6%), staffing (10.8%) and service time (4.1%). Based on the outcome of chi-square test, there was a significance association between provider related factors and client satisfaction (𝑥2 =142.72, df=24, p<0.001), logistic regression analysis showed counselling and male involvement were significantly associated with client satisfaction. Financing and training of health care workers, Quality Assurance and Quality Improvement, addressing human for health gaps, provision of comprehensive Counselling and scale up partner involvement especially male partners is highly recommended in improving and sustaining client satisfaction on PMTCT services. Further studies and periodic assessments on client satisfaction on PMTCT services is highly recommended.
Keywords: Provider related factors-service provider’s aspects that influenced client satisfaction, Satisfaction-State of fulfilment or gratification of one’s needs or expectations
Cite this paper: Leah Njeri Mureithi, Sherry Oluchina, Dainah Kariuki, Provider Related Factors Influencing Satisfaction with Prevention of Mother to Child Transmission Services among HIV Positive Postnatal Mothers Attending MCH/FP Clinic in EL5H, Kenya, International Journal of Nursing Science, Vol. 11 No. 3, 2021, pp. 49-55. doi: 10.5923/j.nursing.20211103.01.
Article Outline
1. Introduction
1.1. Background of Study
- Research has shown that Prevention Mother To Child Transmission (PMTCT) of Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) refers to intercessions to impede HIV transmission from an infected mother to her infant during prenatal period, labor, delivery, and breastfeeding (WHO, 2015). Similarly, Prevention of Mother to Child Transmission prevention (PMTCT) is a term used for designed programs and interventions to reduce the risk of HIV transmission from mother to child (PPFAR, 2017).Worldwide more than 75million people have been infected with HIV (Nature Reviews Disease, 2015), and there are now 36.7 million individuals living with the infection (Global Aids Update, 2016). Approximately 25.5 million people living with HIV are in Sub-Saharan Africa, which contributes to 70% of new HIV infections globally (Global HIV&AIDS Statistics, 2015). Mainly, Human Immunodeficiency Virus/Acquired Immune-Deficiency Syndrome affects people of reproductive age, increasing infections among women who now account for new cases in Sub-Saharan Africa.Kenya is one of the most affected countries by HIV and is jointly ranked fourth in the world alongside Mozambique and Uganda among countries with HIV transmission from mother to child (MTCT) (global information, 2017). According to Fitz (2014) client satisfaction is core to quality of PMTCT services and serves as an important component in continuous evaluation of delivered services to achieve desired outcomes. Client satisfaction with services offered influences their compliance and is an indirect indicator for quality of services. Safeguarding clients’ satisfaction with mother to child transmission prevention services is essential for increasing uptake, promoting compliance and confinement in care. Furthermore, providing better services attracts more clients and increases the utilization of health care services (creel, et al, 2012).
1.2. Objective
- To assess provider related factors influencing HIV positive postnatal mother satisfaction with PMTCT services.
2. Research Materials and Methods
2.1. Study Design
- Facility based cross sectional study was used to obtain both qualitative and quantitative data.
2.2. Study Area Description
- The study was conducted at Embu Level Five Hospital in Embu County (EL5H). The hospital is in the outskirts of Embu town a long Embu- Meru highway approximately two kilometres from Embu town and 120 kilometres from Nairobi (Kenya County Guide, 2016).
2.3. Study Population
- One eighty (180) HIV positive post-natal mothers booked for July, 2019 psychosocial support group meetings.
2.4. Inclusion Criteria/ Exclusion Criteria
2.4.1. Inclusion Criteria
- 1) HIV positive postnatal mothers
2.4.2. Exclusion Criteria
- 1) Newly diagnosed HIV positive postnatal mothers2) HIV positive postnatal mothers below 6 weeks post-delivery.3) Mentally unstable and very sick HIV positive mothers
2.5. Sampling
2.5.1. Sample Size Determination
- The researcher used Yamane (1967:886) formula;
 Where: n = sample sizeN = Total populatione = Margin of error is 5%
Where: n = sample sizeN = Total populatione = Margin of error is 5% n = 130To take care of non-respondent estimated to be 10%, the sample size was converted to 143.
n = 130To take care of non-respondent estimated to be 10%, the sample size was converted to 143.2.5.2. Sampling Technique
- Proportionate to sample size was used to calculate HIV positive postnatal mothers to be sampled from the estimated sample size of 143 mothers in each of the eight (8) psychosocial support groups.
|
2.6. Variables
2.6.1. Dependent Variables
- Satisfaction with PMTCT services was used as the dependent variable for the study. Overall level of satisfaction was measured through a five-point Likert scale based on various pmtct services offered.
2.6.2. Independent Variables
- The independent variables for the study included provider related factors (provider client interaction, counselling, understanding client’s needs, staff attitude, staffing, male involvement, privacy, confidentiality, waiting and service time.
2.7. Data Collection
2.7.1. Data Collection Procedures
- Data collection was done in 8 weeks. Data was collected during pmtct psychosocial support group meetings. The questionnaires were administered by the research assistants.
2.7.2. Data Collection Tools
- Data was collected using semi -structured questionnaires. The questionnaires included socio-demographic characteristics and client satisfaction related to service providers. Likert scale was used to assess satisfaction level. The scale ranged from 1 to 5. Three (3) neither satisfied nor dissatisfied, 1 denotes very dissatisfied, 2 dissatisfied, 4 satisfied and 5 very satisfied.
2.8. Pretest Tool
- Pretesting of the semi- structured questionnaires was done prior to the actual date of data collection at Kerugoya level five hospitals in Kerugoya County. The hospital had similar locality and characteristics thus the researcher expected similar results. Ten (10%) of study participants was used for pretesting to ensure validity and reliability of instruments.
2.9. Quality Assurance Procedures
2.9.1. Validity
- Issues not clear were clarified after pre-testing. Unnecessary questions were deleted after thorough scrutiny. Rephrasing of necessary questions was done accordingly before study commencement.
2.9.2. Reliability
- This was assured by counter checking the completed interview schedules daily to identify and correct any errors that might have occurred.
2.10. Ethical Considerations
- Ethical approval to conduct this study was provided by research and ethics committee (ERC) Nairobi University (UON) Kenyatta National Hospital (KNH). Approval was also received from chief executive officer in Embu level five hospital and Kerugoya level four hospital. Additional approval was provided by officers in charge of maternal neonatal child health clinic. Written consent was obtained from study participants before data collection after they had been informed about the objectives and purpose of the study. Study subjects were given the chance to decline participation or interrupt at any time if they didn’t feel comfortable. Client’s names were not retrieved from the register.
2.11. Data Management
- Data collection was done using semi structured questionnaires. The questionnaires were coded before administration. Manual cleaning of the filled questionnaire was done to check for completeness. Information from the focused group discussion was coded in the computer and checked for completeness. Data was then fed in statistical package for social sciences (SPSS) version 24.0 and cleaned for inconsistencies and missing values. The data was processed, tabulated, and analysed to generate frequency, tables, and graphs.Rate of satisfaction and other variables was computed using descriptive statistics. Bivariate analysis was performed using chi-square to identify factors related to satisfaction and measure association between HIV positive postnatal mothers’ satisfaction and PMTCT services offered at Embu level five hospital. To further establish the variance and strength of association, logistic regression analysis was performed on the independent variables. Data was then presented inform of graphs, pie charts and tables.
2.12. Data Storage, Security, and Access
- The filled in questionnaire was stored in a locked cupboard and the keys kept by the researcher. Coded data was stored in a folder in the researcher’s computer that had password. Filled in questionnaires were stored in a locked cupboard under the custody of the researcher for a period of ten years after data analysis before being disposed. Accessibility of the same by the authorized persons such as KNH-UON ERC during storage period shall be possible upon linking with the researcher. The researcher would also allow access of the coded and analysed data, stored in her computer with a password to the authorized persons upon requisition.Storage of data in a locked cupboard and in the researchers’ computer with a password would help to deny access of the information to the unauthorized persons.
2.13. Study Limitations
- Due to limited time and finances the study was confined to maternal neonatal child health clinic in Embu county hospital. Further, since it is not a trend study, the results obtained were only applicable at one point in time when the study was carried out. Similarly, low turnout of HIV positive postnatal mothers made the study take longer than expected. Finally, the study focused on HIV positive post-natal mothers hence limiting its generalization to all the HIV positive clients.
3. Results and Findings
3.1. Response Rate
- There were seventy-four (74) respondents who managed to fill in the questionnaires (51.7%) and seven (7) FGD interviews were conducted due to saturation (39.2%). Each group had an average of eight members, making a total of 130 respondents out of the targeted sample size of 143. This was translated to a response rate of 91.0%.
3.2. Respondents’ Sociodemographic Characteristics
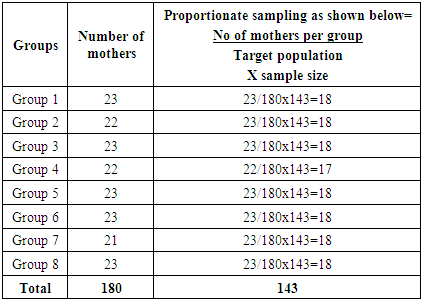
- The survey findings showed that majority of the respondents, 79.7% (n=110/138) were aged 25-49 years while the least, 5.1% (n=7/138) were those aged between 15-19 years. Majority of the respondents, 79.7% (n=110/138) were married, while 17.4% (n=24/138)) were single. Those divorced and widowed were 1.4% (n=2/138) each. Majority of the respondents, 36.2% (n=50/138) had parity 2+0, while the least, 6.5% (n=9/138) were para 3+1 and above. Over half of the mothers, 60.1% (n=83/138) had secondary education and above. Most of the respondents, 42% (n=58/138) were housewives. Respondents from Embu county contributed 86.9% (n=9/138) of the sampled respondents.
|
3.3. Provider Related Factors
- Provider related factors included the provider interaction with the clients, staff attitude, understanding client’s needs, staffing, privacy, and confidentiality, waiting and service time as experienced by the clients. The factors were based on various PMTCT services to include HIV testing, family planning, ARV drug prophylaxis, infant prophylaxis, infant feeding practices, early infant diagnosis, and psychological support group.
3.3.1. Provider Related Factors that Influenced Client’s Satisfaction
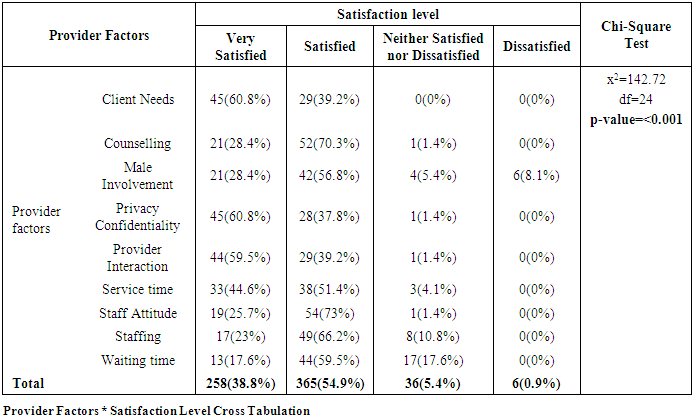
- Majority of the respondents, 93.7% were highly satisfied with provider factors regarding the seven services offered at EL5H. However, 0.9% and 5.4% of the respondents reported dissatisfaction and neither satisfied nor dissatisfied with provider factors respectively. Cross tabulation showed that, majority of the respondents were dissatisfied with; waiting time (17.6%), male involvement (13.6%), staffing (10.8%) and service time (4.1%). Based on the outcome of chi-square test, there was a significance association between provider related factors and client satisfaction (𝑥2 =142.72, df=24, p<0.001).
3.3.2. Logistic Regression on Provider Related Factors
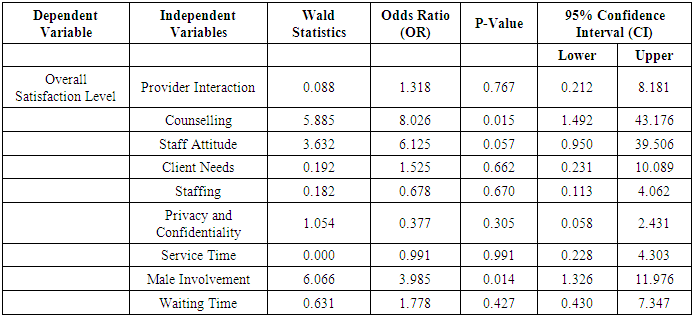
- Ordinal logistic regression analysis was performed to model the relationship between the predictors (provider related factors) and overall levels of satisfaction (very satisfied, satisfied, and other). The traditional 0.05 criterion of statistical significance was used for all tests. Counselling and male involvement were the predictors with significant parameters for comparing the very satisfied group with the satisfied group. This further showed, improvement of the two variables would increase client satisfaction by 8 and 4 times respectively as compared to other provider related factors increasing the odds ratio by over 4 times.
3.3.3. Participants Likes about PMTCT Service Providers
- From the FGD, most of respondents registered satisfaction, stating that the services should continue as they were. Regarding the main theme on participants likes about pmtct service providers the emerging sub- themes included provider interaction and male partner involvement.
3.3.3.1. Sub-Theme 1: Provider Interaction
- Majority of the participants reported that, they had good interaction with their service providers. One of the participants noted that:“The staff at the facility are emphatic to us and they also understand our needs” (Respondent 5 FGD 2).This sentiment was seconded by another participant who said that:“The staff have good communication skills, and they understand our needs adequately.” (Respondent 3 FGD 1).
3.3.3.2. Sub-Theme 2: Male Partner Involvement
- Participants echoed to the statement that the service providers provided options and encouraged clients to come with their partners for testing and counselling as one respondent indicated that: “My partner is able to know his HIV status, he is also counselled before and after testing” (Respondent 3 FGD 6).
3.3.4. Participant’s Dislike about PMTCT Service Providers
- From the FGD, participants felt that there were aspects that they disliked and needed attention to improve their overall satisfaction. Regarding the main theme on participants dislikes about PMTCT service providers the emerging sub- themes included provider attitude and waiting time.
3.3.4.1. Sub-Theme 1: Provider Attitude
- Despite the many positive feedbacks, majority of the respondents expressed that there was need for some staff to change their negative attitude. For instance, one participant noted that:“Some service providers are rude and lack good interaction skills. In the HIV testing services, health providers did not give counselling to the partner before testing” (Respondent 1 FGD 2).
3.3.4.2. Sub-Theme 2: Waiting Time
- The other concern was the waiting time where several participants reported that they waited for long before being served. One participant said that: “We wait for long period of time before we are attended to, and this reduces our morale to seek treatment.” (Respondent 3 FGD 5).
|
|
3.3.5. Participant’s Suggestions Related to Service Providers to Improve PMTCT Services
- From the FGD’S regarding to the main theme on participants suggestions about PMTCT service providers the emerging sub- themes included maintaining client confidentiality and staffing.
3.3.5.1. Sub-Theme 1: Maintaining Client Confidentiality
- One of the suggestions was to ensure high confidentiality for the clients during counselling, and to allay all fears before testing. In support of these assertions, one respondent noted that:“The health care professionals need to counsel us while upholding our confidence, and not to in still fears in us. This creates a good environment for the overall testing services and other procedures.” (Respondent 6 FGD 8).Another respondent in the same 7 supported the above sentiment by reporting that:“Our confidentiality is paramount and this needs to be maintained” (Respondent 4 FGD 8).
3.3.5.2. Sub-Theme 2: Staffing
- Majority of participants reported that there was need to improve staffing in MCH/FP clinic. One of them suggested that: “There is need to increase the number of health care professional in the section of family planning services” (Respondent 7 FGD 4).
4. Discussion, Conclusions, and Recommendations
4.1. Discussion
4.1.1. Socio-Demographic Information
- The survey findings showed that majority of the respondents, 79.7% (n=110/138) were aged 25-49 years. Majority of the respondents, 79.7% (n=110/138) were married. Most of the respondents, 36.2% (n=50/138) had parity 2+0 and above. Over half of the mothers, 60.1% (n=83/138) had secondary education and above. Most of the respondents, 42% (n=58/138) were housewives. Respondents from Embu county contributed 86.9% (n=9/138) of the sampled respondents.
4.1.2. Provider Related Factors
- Provider related factors included the provider interaction with the clients, counselling, staff attitude, understanding client’s needs, staffing, male involvement, privacy and confidentiality, waiting and service time as experienced by the clients. The factors were based on various PMTCT services to include HIV testing, family planning, ARV drug prophylaxis, infant prophylaxis, infant feeding practices, early infant diagnosis, and psychological support group.
4.1.2.1 Provider Related Factors that Influenced Satisfaction of HIV Positive Postnatal Mothers with PMTCT Services
- Majority of the respondents, 93.7% were highly satisfied with provider factors regarding the seven services offered at EL5H. However, 0.9% and 5.4% of the respondents reported dissatisfaction and neither satisfied nor dissatisfied with provider factors respectively. Cross tabulation showed that, majority of the respondents were dissatisfied with; waiting time (17.6%), male involvement (13.6%), staffing (10.8%) and service time (4.1%). Based on the outcome of chi-square test, there was a significance association between provider related factors and client satisfaction (𝑥2 =142.72, df=24, p<0.001).The results pointed that respondents were satisfied with the provider factors as opposed to other options, neither satisfied nor dissatisfied and dissatisfied. The findings by Lyatuu, Msamanga, and Kalinga (2008) also relate to this study findings where aspects like counselling, preconception care, antenatal care, health education and family planning were offered by supporting, non-judgmental staff with adequate time to listen to each of the patients. A study with similar findings was done by Yeshewas (2016) in Dessie referral hospital, Ethiopia on quality of PMTCT services that showed; despite clients being highly satisfied with the PMTCT services offered, there are clients who were not satisfied with the waiting time they spent while accessing services.Logistic regression analysis showed that, counselling and male involvement were the predictors with significant parameters for comparing the very satisfied group with the satisfied group increasing the odds ratio by over 4 times. This further showed, improvement of the two variables would increase client satisfaction by 8 and 4 times respectively as compared to other provider related factors. satisfaction on aspects like; HIV testing, infant feeding practices, early infant diagnosis and male involvement ensure HIV+ mothers are able to care for their infants, thus promising quality health.
4.2. Conclusions
- Majority of the respondents were highly satisfied with an average rate of over 93 percent compared to those who were dissatisfied and neither satisfied or dissatisfied with the services of health providers at the MCH/FP clinic at an average rate of 0.9% and 5.4% respectively. Cross tabulation showed that, majority of the respondents were dissatisfied with, waiting time (17.6%), male involvement (13.6%), staffing (10.8%) and service time (4.1%). Counselling and male involvement were the predictors with significant parameters for comparing the very satisfied group with the satisfied group increasing the odds ratio by over 4 times. Shortage of health care workers, time management and partner involvement are critical component of providing quality PMTCT services at MCH/ FP clinics. Therefore, training of health care workers on time management, addressing the human for health gaps and scaling up of partner involvement especially male partners can contribute significantly to improving and sustaining client satisfaction on PMTCT services in Kenya.
4.3. Recommendations
- 1. Policy makers to plan and provide financing on training health care providers on Quality Assurance and Quality Improvement for increased client satisfaction on PMTCT services.2. Need for the policy makers to address Human Resources for Health to improve provider – client ratios for improved quality of PMTCT services.3. Need to develop policies that encourage comprehensive counselling and support partner involvement for increased and sustained client satisfaction on PMTCT services.4. Further studies and periodic assessments on client satisfaction on PMTCT services are recommended.
ACKNOWLEDGEMENTS
- The study acknowledges Leah Njeri Mureithi, Sherry Oluchina, BSCN, MSCN, PHD, Dainah Kariuki BSCN, and MSC. Leah was involved in manuscript write up while Sherry and Dainah were involved in guidance and supervising of this study from beginning to the end.
DEFINATION OF TERMS
- Dissatisfaction - Failure of service offered to meet clients’ expectation/needs/demandsEmbu Level 5 Hospital (EL5H) - Referral and teaching hospitalFocused Group Discussion (FGD) - A group of HIV positive postnatal mothersHIV Positive postnatal Mothers - Clients who are HIV positive attending post-pregnancy clinicMaternal Child Health & Family Planning (MCH/FP) - Department offering integrated services to under-fives, pregnant and postnatal mothersPrevention of Mother To Child Transmission (PMTCT) - program that prevents HIV transmission from HIV positive mother to her baby in pregnancy and postnatally during lactationProvider related factors-service provider’s aspects that influenced client satisfactionPsychosocial Support Groups (PSSG)-groups of HIV positive postnatal mothersSatisfaction -Ability of service offered to meet clients’ expectation/needs/demands