-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2021; 11(2): 41-47
doi:10.5923/j.nursing.20211102.03
Received: Jul. 27, 2021; Accepted: Aug. 6, 2021; Published: Aug. 15, 2021

Socio-Cultural Factors Influencing Utilization of Preconception Care among Women Seeking Antenatal Care in Machakos Level 5 Hospital, Machakos County, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWashingtone Omondi Owino1, Sherry Oluchina2, Carolyne Kerubo Nyariki2
1School of Nursing, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Oyugis, Kenya
2School of Nursing, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Nairobi, Kenya
Correspondence to: Washingtone Omondi Owino, School of Nursing, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Oyugis, Kenya.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Care provided before conception can promote the general wellbeing of women before conception and in between the future pregnancies. Despite this, the whole idea of preconception care still remains to be fully exploited. The main objective of this study was to assess socio-cultural factors influencing utilization of preconception care among women seeking antenatal services in Machakos level 5 hospital. Retrospective descriptive cohort study design was used. The study was carried out in the Antenatal Clinic at Machakos Level 5 Hospital, Kenya. A sample of 233 pregnant women from 478 pregnant women who attended antenatal clinic per month was randomly selected. Systemic sampling was used, where every second client was requested to take part in the study, upon being subjected to inclusion criteria. Whenever the second client was not legible to take part, the next client was considered. A semi-structured questionnaire was used to collect data. The level of utilization of preconception care was 14.6%. Respondents who were formally employed were 5.7 times more likely to utilize preconception care, compared to their unemployed counterparts (p = 0.004, OR = 5.707). Respondents who were assisted to make decision to seek preconception care were 5.236times more likely to utilize preconception care, (p<0.0001, OR = 5.236), compared to those who were not assisted.This study concluded that level of utilization of preconception care was low. Factors that affected utilization of preconception care were employment status of respondents and being assisted by someone else to make decision to use preconception care.
Keywords: Preconception care, Antenatal care clinic, Utilization, Socio-cultural factors
Cite this paper: Washingtone Omondi Owino, Sherry Oluchina, Carolyne Kerubo Nyariki, Socio-Cultural Factors Influencing Utilization of Preconception Care among Women Seeking Antenatal Care in Machakos Level 5 Hospital, Machakos County, Kenya, International Journal of Nursing Science, Vol. 11 No. 2, 2021, pp. 41-47. doi: 10.5923/j.nursing.20211102.03.
Article Outline
1. Introduction
- Pre-conception care is any interventions, either advice or treatment, and lifestyle modifications women receive regarding components of preconception care to improve health before being pregnant [1-3]. Components of preconception care include: HIV testing and counseling, STI screening and treatment, Infertility treatment, Nutrition, Ferrous and folic acid supplementation, Immunization, contraception, Advice on cessation of alcohol and cigarette smoking. Preconception period is range between 3-6 months before conception. Utilization in this study is the use of any one of the components of preconception care at least once before being pregnant [4]. Globally, four out of ten women report unplanned pregnancies [5]. In sub-Saharan Africa, poor preconception care was due to low economic status, illiteracy and lack of awareness [6]. In Kenya, 1.8 million women had unplanned pregnancies per year & maternal mortality was 362 per 100,000 live births per year [7]. From the year 2015 to 2016 Machakos County had 50,000 women with unplanned pregnancies & maternal mortality of 100 per 100,000 live births per year. During the same period, 30,000 women had unmet needs for contraception [7]. Most of these unmet needs of contraception, un-planned pregnancies & mortalities can be avoided if preconception care is practiced.Preconception care improves interval between pregnancies, reduces unplanned pregnancies and pregnancies at risk of genetic disorders and environmental exposures. It also improves maternal & neonatal health outcomes, thus reducing maternal & neonatal mortality. Women seeking ANC services were chosen because they had just conceived and were more likely to recall if they used preconception care. This study therefore was meant to shed more light on factors affecting utilization of preconception care at Machakos level 5 hospital and help in development of policies and strategies for improving utilization of pre-conception care.
2. Materials and Methods
2.1. Study Setting, Design and Population
- This study was carried out in Antenatal Clinic of Machakos Level 5 hospital in Kenya whereby retrospective descriptive cohort study design was used. According to the antenatal register, an average of 478 pregnant women was seen at the clinic monthly in the year 2019. The figure was used to estimate the target population for the study. All pregnant women of reproductive age who sought antenatal care in ANC clinic at Machakos level 5 hospital formed the study population.
2.2. Inclusion Criteria and Exclusion Criteria
- All pregnant mothers who attended antenatal clinic were included in the study while, all pregnant women who were mentally or physically sick at the time of the study were excluded from the study.
2.3. Sampling Technique and Sample Size
- The study used population proportion sample size calculation in determining the sample which was found to be the true representative of the study. Systemic sampling technique was applied in selecting the pregnant women at the antenatal clinic. The procedure was explained to the respondents after which every 2nd client meeting the inclusion criteria was interviewed. The process continued until the sample size of 233 respondents was achieved. This was a true representative of the pregnant women seeking antenatal care at Machakos level 5 hospital.
2.4. Data Collection Tools
- A researcher administered questionnaire with both open and closed-ended questions was used to collect data from the pregnant women over a period of about one month. The questionnaire captured: level of utilization of preconception care and socio-cultural factors. Key informants interview guide with 5 questions was used to collect qualitative data from key informants.
2.5. Pre-Test of the Questionnaire
- The pre-test of the questionnaire was done at the Thika level 5 hospital to determine the validity and reliability of data collection tools before the real study. The pretested sample represented 10% of the final study sample size. The questionnaire was then revised to ensure that the questions provided the desired answers.
2.6. Data Analysis and Presentation
- Data was coded, entered and analysed using SPSS version 26 software. Descriptive statistics was utilized. Under this, quantitative data was presented in pie charts, bar graphs, frequency tables, and histograms. Qualitative data from key informants was comprehensively transcribed, analysed thematically and an elaborate summery written. Information from the key informants was collaborated with results from the semi structured questionnaire, and then similarities and differences were elaborately described.Chi square test was calculated to help in evaluating the association between independent variables (socio-cultural factors), and dependent variable (utilization of preconception care). To assess effects of each independent variable that predict the outcome of dependent variable, binary logistic regression was done.
2.7. Ethical Considerations
- Permission to carry out the research was given by the Jomo Kenyatta University of Agriculture School of Nursing. Proposal was presented to the University of Eastern Africa Baraton, research and ethical committee for ethical clearance for conducting the study (Ref No: UEAB/REC/03/08/2020). Permission was granted by National Commission for science, Technology and Innovation (NACOSTI) and authority sought from Machakos level 5 hospital management. Further consent was obtained from the antenatal clinic in charge. Respondents were requested to give consent by signing an informed consent form.
3. Results
3.1. Level of Utilization of Preconception Care Among Women Seeking ANC Services at Machakos Level 5 Hospital
- This study found out that only (14.6%) of respondents used preconception care.
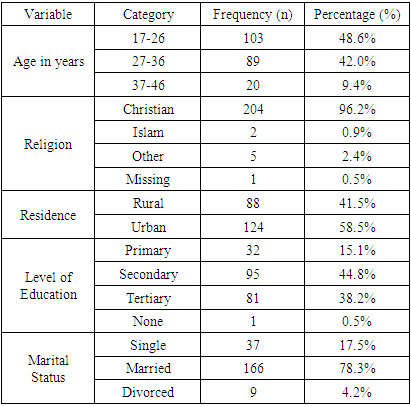
3.2. Socio-Demographic Characteristics of the Respondents
- Majority of women 48.6% (n=103) were aged 17-26 years. Most of the women 96.2% (n=204) were Christian. Fifty eight point five percent (n=124) and 41.5% (n=88) lived in urban and rural setup respectively. On the level of education, minority of the women 15.1% (n=32) had primary education. On marital status, majority of women 78.3% (n=166) were married. (Table 1)
|
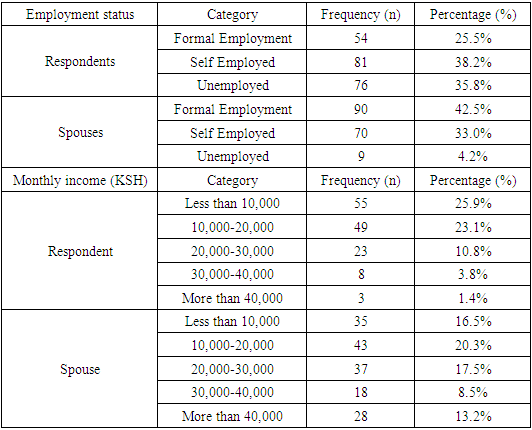
3.2.1. Employment and Income Status of the Respondents and Their Spouses
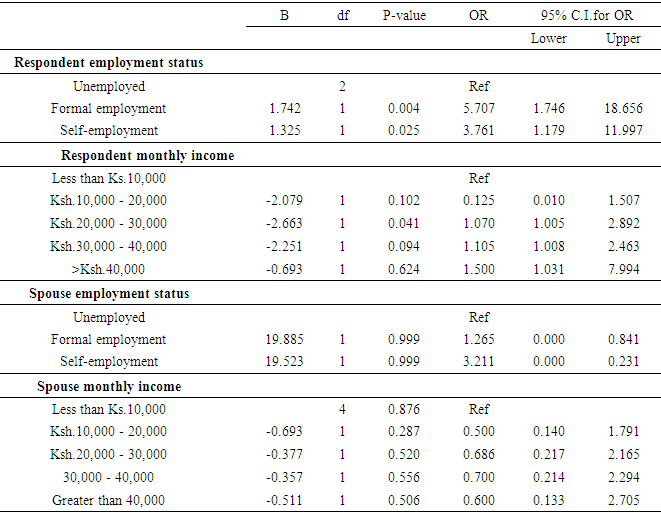
- This study found out that, 25.5% (n=54) of respondents had formal employment and 35.8% (n=76) were unemployed. Among their spouses, 42.5% (n=90) had formal employment. Majority, 25.9% (n=55) of the respondents earned less than 10,000ksh. Among their spouses, 20.3% (n=43) earned between 10,000ksh to 20,000ksh while 13.2% (n=28) earned more than 40,000ksh per month. (Table 2)
|
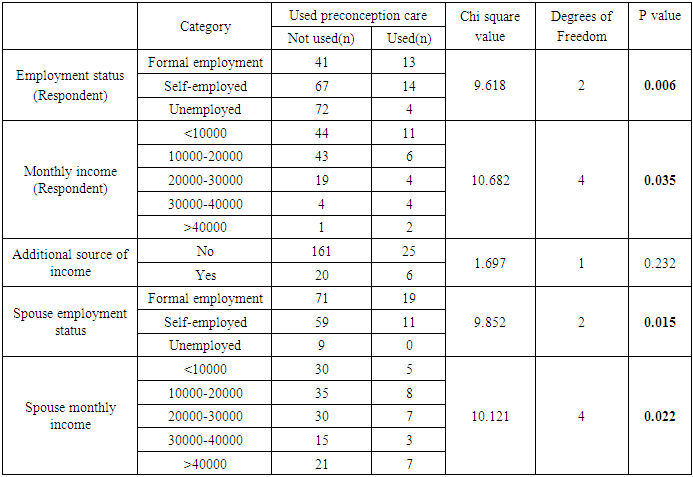
3.2.2. Association between Demographic Factors and Utilization of Preconception Care
- On Chi square test, employment status and basic monthly net income of the women and employment status and monthly net income of their spouses were significantly associated with utilization of preconception care (p values = 0.006, 0.035, 0.015 and 0.022) respectively. (Table 3)
|
|
3.3. Socio-Cultural Factors Affecting Utilization of Preconception Care
3.3.1. Presence of Cultural Beliefs and Practices on Utilization of Preconception Care
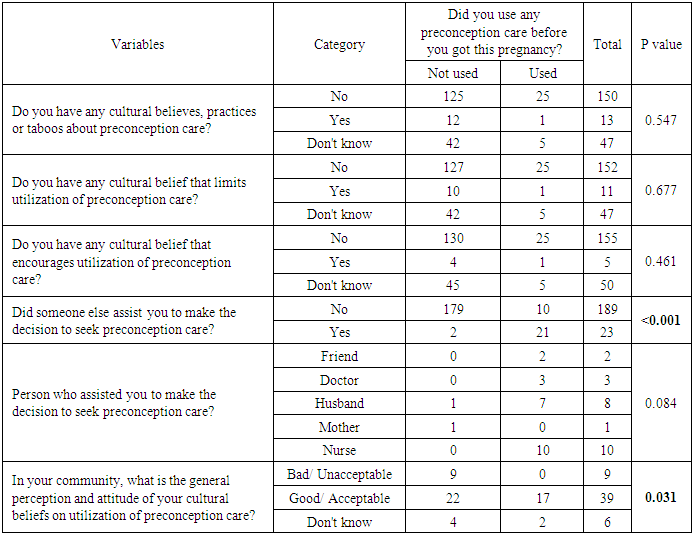
- The study found out that majority of women 70.8% (n=150) did not have any cultural beliefs or practices affecting utilization of preconception care.
3.3.2. Presence of Cultural Beliefs that Encourage Utilization of Preconception Care
- On this, the researcher found out that majority of the respondents 73.1% (n=155) did not have cultural practices that encourage utilization of preconception care, 2.4% (n=5) said they have while 23.6% (n=50) said that they did not know whether there are any cultural practices that encourage utilization of preconception care.
3.3.3. Presence of Cultural Beliefs that Limit Utilization of Preconception Care
- On this, the researcher found out that majority of the respondents 71.7% (n=152) did not have cultural practices that limit utilization of preconception care, 5.2% (n=11) said they have while 22.2% (n=47) said that they did not know whether there are any cultural practices that limit utilization of preconception care.
3.3.4. Assistance to Use Preconception Care
- On this, the study found out that majority 89.2% (n=189) of the respondents were not assisted by anyone to use preconception care, while 10.8% (n=23) were assisted to use preconception care. Majority of women 43.5% (n=10) were assisted by nurses to use preconception care, 8.7% (n=2) by friends, 13.0% (n=3) by doctors, 30.4% (n=7) by husbands, 4.4% (n=1) by mothers.
3.3.5. General Attitude and Perception of People on Use of Preconception Care
- This study also sought to find out the attitude and perception of people on the utilization of preconception care. The community’s general perception and attitude of cultural beliefs on utilization of preconception care are bad/ unacceptable 4.2% (n=9), and good/ acceptable 18.4% (n=39), while 2.8% (n=6) don't know.
3.3.6. Cultural Beliefs
- Majority of women 46.2% (n=6) reported failed conception as the cultural belief that influence utilization of preconception care.
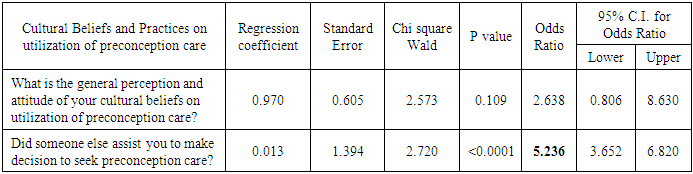
3.3.7. Association between Socio-Cultural Factors and Utilization of Preconception Care
- On Chi square test, being assisted by someone else to make decision to use preconception care and perception of culture on use of preconception care were statistically significant with P-values <0.001 and 0.031 respectively (Table 5).
|
|
4. Discussion
4.1. Level of Utilization of Preconception Care Among Women Seeking ANC Services at Machakos Level 5 Hospital
- This study found out that only (14.6%) of respondents used preconception care which was higher than a study carried out in Sudan by Khalid [8] which found the level of utilization to be 9%. This difference could be due to variation in socio-demographic and economic status between the two geographical locations. However, it was lower than the finding from a study done in Brazil [9] which found the level to be 15.9%. The possible explanation might be due to difference in the study setting, study participants and health care system of the countries.It is was also significantly lower than study conducted in Saudi Arabia [10], which found the level of utilization to be 29.3%. This might be due to the fact that this study in Saudi Arabia was a cumulative result of different studies that were conducted on different study participants with large sample size in different study settings and period.
4.2. Demographic Characteristics Affecting Utilization of Preconception Care Among Women Seeking ANC Services at Machakos Level 5 Hospital
- The present study revealed that majority 78.3% of respondents were married. This finding was similar to study done in Kenya by Chepngetich [11] on preconception care utilization that reported married women to be at 70.6%. Similarly, a study done in Kenya Coast General Hospital [12] found 68% of the respondents to be married. This similarity could be due to the fact that the two studies were done in Kenya. This was however lower than a study done in Nigeria [13], that revealed 97.8% of the respondents to be married. This difference could be due to differences in geographical settings with different inhabitants.This present study found out that formal employment was significant associated with utilization of preconception care (P= 0.004). Similarly, a study done in Ethiopia [14], showed a significant association between employment status and income level of respondents with utilization of preconception care. Another study by Markos and Bogale, in Goba Woreda, Oromia region of Ethiopia [15] established that employment status of women greatly influenced their ability to utilize preconception care. This similarity could be attributed to fact that the two studies were carried out in more of an urban setting. On the contrary, a study done in Kenya by Gitonga [16] showed no significant relationship between respondent’s employment status and utilization of preconception care. In the above study, utilization of preconception care did not depend on respondent’s employment status level, rather, it was found out that other factors like socio-cultural played a significant influence. Another contrasting study done in Nigeria [17] among women of the Amassoma community on awareness and barriers to utilization of preconception care services found out that there was no significant association employment status of women and the utilization of preconception care. This difference could be due to differences in the study setting and variation in inhabitants from which study samples were drawn.
4.3. Socio-Cultural Factors Influencing Utilization of Preconception Care Among Women Seeking ANC Services at Machakos Level 5 Hospital
- This study found out that being assisted by someone else was significant associated with utilization of pre-conception care (P=< 0.0001). Similarly, a study done in Nigeria [18], on preconception care preparedness, found out that socio-cultural perception affects utilization preconception care. A study done in Kiambu County [11] also had a similar finding that being assisted by someone else influenced utilization of preconception care (P<0.05). This is in agreement with a study by Nawal, and Goli, [19] who found out those socio-cultural interventions before pregnancy can help promote wellbeing of adolescents and adult women and improve subsequent pregnancy and childbearing outcomes hence utilization of preconception care.Contrary to this, a study by Obi and Okojie, [18] on preconception care preparedness and complication readiness: knowledge and practices among pregnant women in Benin City Edo state, Nigeria and found out that socio-cultural factors had very minimal influence on utilization of preconception care. This difference could have been brought about by variations in socio-cultural practices of the two communities that were interviewed in the studies.
5. Conclusions
- The following conclusions were made from the study. Level of utilization of preconception care at Machakos level 5 hospital was found to be low at 14.6%. The only socio-demographic factor that affected utilization of preconception care was formal employment of respondents. Being assisted by someone else was the only socio-cultural factor that affected utilization of preconception care.