-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2021; 11(2): 36-40
doi:10.5923/j.nursing.20211102.02
Received: Jul. 10, 2021; Accepted: Jul. 21, 2021; Published: Jul. 30, 2021

Health System Factors Associated with Adherence to Tracheostomy Care Guidelines among Critical Care Nurses at a National Referral Hospital in Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNewton Ongaki Ochoki1, Mutisya Albanus Kyalo2, Mwangi Elijah Githinji2
1School of Nursing, Jomo Kenyatta University of Agriculture and Technology and Critical Care Nurse at Avenue Group, Nairobi, Kenya
2School of Nursing, Jomo Kenyatta University of Agriculture and Technology, Kiambu, Kenya
Correspondence to: Newton Ongaki Ochoki, School of Nursing, Jomo Kenyatta University of Agriculture and Technology and Critical Care Nurse at Avenue Group, Nairobi, Kenya.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

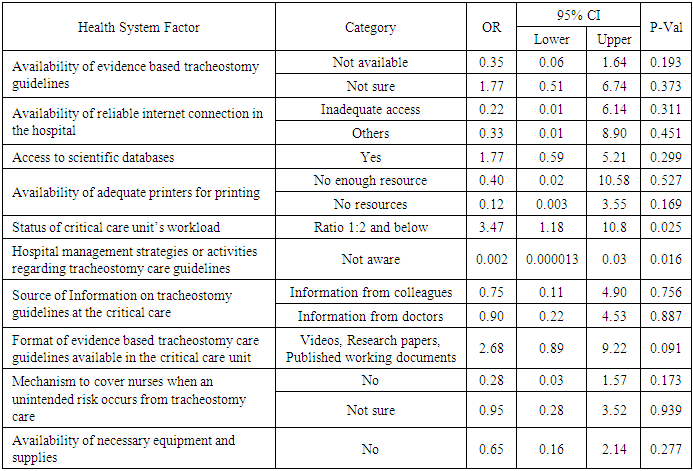
Tracheostomy care is a routine nursing procedure in critical care units of many hospitals. This study therefore sought to establish health system factors associated with adherence to tracheostomy care guidelines among critical care nurses. This was an analytical cross-sectional study conducted in a national referral hospital in Kenya among critical care nurses. The sample size comprised a total of 79 nurses working in the critical care unit. An observational checklist and a self-administered questionnaire was used to collect quantitative data. Data was analyzed using R studio version 1.4.1103. In the bivariate analysis Fishers exact test or chi-square test was used to find associations between health system factors and adherence to the guidelines while in the multivariate analysis binary logistic regression was used to establish health system factors associated with adherence to the guidelines. Statistical significance was set at a P value below 0.05 at 95% confidence interval. The study findings revealed that 18(22.8%) nurses adhered to tracheostomy care guidelines while 61(77.2%) did not. Awareness of hospital management strategies and activities regarding tracheostomy care guidelines was the only health system factor associated with adherence to tracheostomy care guidelines in the multivariate analysis (AOR 0.21; 95% CI: 0.05-0.73; P=0.019). Nurses who were not aware of hospital management strategies or activities regarding tracheostomy care guidelines were less likely to adhere to tracheostomy care guidelines compared to those who were aware.
Keywords: Adherence, Tracheostomy care guidelines, Health system factors, Critical care unit
Cite this paper: Newton Ongaki Ochoki, Mutisya Albanus Kyalo, Mwangi Elijah Githinji, Health System Factors Associated with Adherence to Tracheostomy Care Guidelines among Critical Care Nurses at a National Referral Hospital in Kenya, International Journal of Nursing Science, Vol. 11 No. 2, 2021, pp. 36-40. doi: 10.5923/j.nursing.20211102.02.
Article Outline
1. Introduction
1.1. Background of the Study
- Tracheostomy placement is indicated for respiratory distress. The care of a tracheostomy is routine in intensive care units. This care should be done through utilizing tracheostomy care protocols. Internationally adherence to tracheostomy care guidelines is affected by various factors [1].These guidelines give information on assessment of the airway for patency, sizes of suction catheters, use of a humidifier system or heat moisture exchange, duration for suctioning and infection prevention techniques such as through use of closed system suction catheters. The guidelines also give information on multidisciplinary team work in the care of a tracheostomized patient [2].In Kenya the devolved system of governance allows for counties through partnerships with the national government to publish such guidelines. In the absence of county and national guidelines, hospitals or nurses can develop the guidelines based on scientific evidence. Studies from Sub Saharan Africa regions have established the importance of all stakeholders in provision of healthcare to work with government institutions to facilitate adherence to the guidelines and establish factors affecting adherence [3].For adherence of tracheostomy care guidelines to be optimal Intensive care units should ultimately have infrastructure which facilitates access to tracheostomy care guidelines. This will enable practice of tracheostomy to be evidence based and upto current standards [4].
1.2. Research Objective
- To establish health system factors associated with adherence to tracheostomy care guidelines among critical care nurses at a national referral hospital in Kenya.
2. Methodology
2.1. Study Design
- This was an analytical cross-sectional study design. These are studies which measure exposure and outcomes but at a single time [5]. The design enabled collection of quantitative data at a single point for measurement of associations without influence. This design was relevant because it allowed for measurement of exposure and outcomes within the specific defined population in the study at one point.
2.2. Sampling and Recruitment Procedure
- Due to the number of the study population, the researcher carried out a census that included a target population of 79 critical care unit nurses. The study therefore did not involve sampling. The inclusion criteria for this study were all nurses stationed at the general intensive care unit. The exclusion criteria included student trainees who are normally not routinely involved in provision of tracheostomy care.
2.3. Data Collection
- A coded self-administered questionnaire and observational checklist for each nurse was used to collect quantitative data. To eliminate biasness nurses were observed without their knowledge when they were performing tracheostomy care. The guidelines for adherence were adopted from scientific databases such as PubMed and Cinahl published across various platforms for use including government websites [6]. Health system factors affecting adherence were obtained from filling a structured questionnaire by the nurses. Pre-testing of the data collection tools was done with ten nurses at the neurological intensive care unit of the national referral hospital. Data was collected for a period of three months. Data collection was done by a trained research assistant who is a licensed critical care nurse. The research assistant did not participate in the study and was trained on study objectives, study informed consent, data collection procedure and checking completeness of questionnaires.
2.4. Data Management
- Data was coded then entered to Epidata version 3.1. It was later cleaned. Thereafter it was exported to Microsoft excel 2010. The data was then afterwards exported to Rstudio version 1.4.1103 for analysis. Descriptive Statistics was used to describe frequencies, means and percentages. Adherence to tracheostomy care guidelines was binary with a cut off of 80% [7]. Fishers test and Chi-square test was used to test for association between health system factors and observed adherence level in the univariate analysis. Binary logistic regression was later used in the multivariate analysis to determine statistically significant factors affecting adherence to the guidelines when controlling for possible confounders. The threshold for Statistical significance in the study was set at a P value of < 0.05 with a 95% confidence interval.
2.5. Ethical Considerations
- Ethical approval was provided by University of Nairobi ethical review body along with the study hospital ethical review body. Afterwards license to conduct the study was issued upon application by the National commission for science, technology and innovation of Kenya (NACOSTI). All the information in the study was held in strict confidentiality through assigning codes to the questionnaires. Signed informed consent was gained from the participants to collect data and no harm was present during the study period. Directives by the Kenyan government on prevention of transmission of COVID-19 during the study was also followed.
2.6. Study Limitation
- Limitation of this study, is that it was conducted in one center and thus the situation in other hospitals may not have been reflected. Another limitation is that tracheostomized patients in the hospital, did not report what they viewed as health system factors affecting adherence to tracheostomy care guidelines as it was only done by the nurses.
3. Results
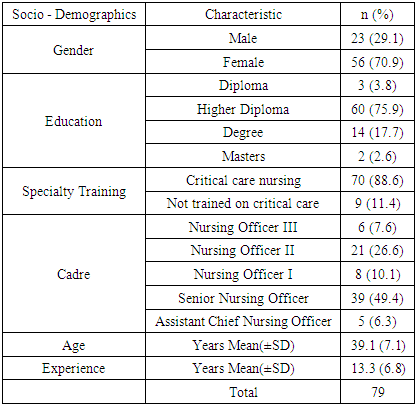
- The study participants consisted of 79 nurses stationed at the intensive care unit. Mean age of the participants was 39.1 years and they had a mean experience of 13.3 years. A total of 23 (29.1%) nurses were male while 56 (70.9%) were female. Majority of the nurses 60 (75.9%) had trained up to higher national diploma level. In relation to specialty training, 70 (88.6%) nurses had been trained on critical care nursing while 9(11.4%) had no specialized training in critical care. In terms of cadre, senior nursing officers were the majority at 39(49.4%). Table 1 shows a descriptive analysis of the socio-demographic data.
|
|
|
|

4. Discussion
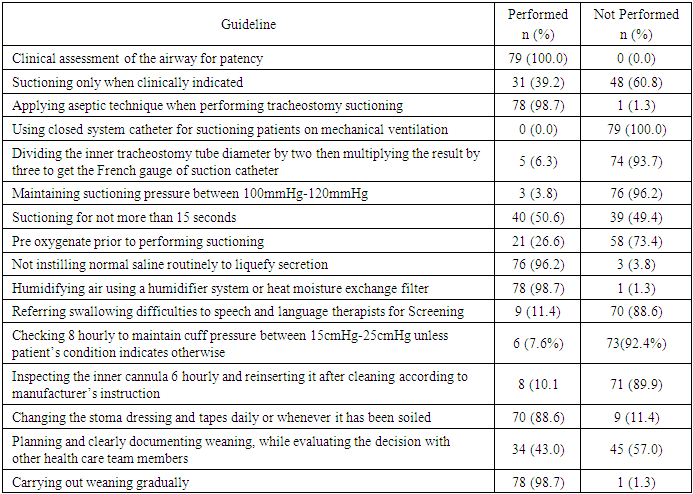
- On observation majority of the nurses did not adhere to tracheostomy care guidelines. This finding is different from a study done in Canada by Leddy who established majority of the nurses followed tracheostomy care guidelines. In this study pre-oxygenation prior to performing suctioning was performed by 26.6% of the nurses while in Leddy’s study it was performed by 60% of the sample size. Use of a closed system suction was performed by none of the nurses in this study while in Leddy’s study it was performed by 99% of the nurses [8,9]. These observations might have been influenced by different levels of technology and types of work equipments.Awareness of mechanisms by the hospital to cover nurses when an unintended risk occurs from adopting tracheostomy care guidelines was not associated with adherence to tracheostomy care guidelines. This is in contrast with Thomas in the USA who found adoption of a care bundle on tracheostomy care that had mechanisms of protection against tracheostomy related ulcers led to adherence [10,11]. The differences from the two studies could be attributed to many number of litigation because of patient awareness in the developed USA as compared to Kenya.In this study a ratio of 1:2 and below in the critical care unit was significantly associated with adherence to tracheostomy care guidelines. This is similar to other studies which find a work ratio of 1:2 and below is associated with adherence. In this study nurses who were not aware that hospital management strategies and activities regarding tracheostomy care guidelines exist were less likely to adhere to tracheostomy care guidelines. This is similar to other studies which established awareness of organizational management support among the nurses led to adherence [12,13]. These findings imply hospitals which are staffed adequately and also disseminate policies to their staff are likely to practice tracheostomy care which follows current guidelines.
5. Conclusions
- Overall based on the results majority of the nurses in the critical care unit did not adhere to tracheostomy care guidelines when observed. The health system factor associated with adherence to the guidelines was awareness of hospital management strategies or activities regarding tracheostomy care. Nurses who were aware of the hospital management strategies and activities regarding tracheostomy care guidelines were more likely to adhere to the guidelines compared to those who were not aware. Furthermore the nurses reported they did not know of mechanisms by the hospital to cover them when unintended risks occur from applying new tracheostomy care guidelines.
6. Recommendations
- The study recommends that nurses in critical care units to undergo refresher training on tracheostomy care periodically to update practice to current guidelines. Hospital policies on application of new guidelines and mechanisms to cover nurses when risks occur from application of the guidelines should be made aware to nurses.
ACKNOWLEDGEMENTS
- The authors of this study would wish to acknowledge the staff at the national referral hospital who participated in this study. Their support is greatly indebted.