-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2020; 10(1): 25-32
doi:10.5923/j.nursing.20201001.03

Effect of Evidence-based Counseling on Improving Rural Patients' Information, Health Behavior and Their Satisfaction Regarding the Habitual Abortion
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMirfat Mohamed Labib El-Kashif 1, Howaida Amin Hassan Fahmy Elsabaa 1, Mageda Abdelaty Soliman 2
1Assistant Professor, Department of Maternity, Obstetrics and Gynecological Nursing, Faculty of Nursing, Port Said University, Port Said, Egypt
2Assistant Professor, Department of Nursing Administration, Faculty of Nursing, Benha University, Egypt
Correspondence to: Mirfat Mohamed Labib El-Kashif , Assistant Professor, Department of Maternity, Obstetrics and Gynecological Nursing, Faculty of Nursing, Port Said University, Port Said, Egypt.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Habitual abortion is one of the most critical debated reproductive issues which its underlying mechanisms are poorly understood. Aim: To investigate the effect of evidence-based counseling on improving rural patients' information, health behavior and their satisfaction regarding the habitual abortion. Setting: The obstetric and gynaecological inpatient departments and outpatient clinics in Benha university hospital and ministry of health hospital, Qaliubiya governorate. Study Design: A Quasi-experimental (an interventional pre and post-test study). Sample size: 119 patients, five were excluded for participation in the pilot study. Sample type: Purposive sample. Tools: Two tools were used: 1) A structured interviewing questionnaire; 2) Patients’ Satisfaction tool. Results: The result of the present study had revealed a highly significant improvement in total patients’ information, health behavior among the studied subject's pre-intervention compared to four weeks' post-intervention. Additionally, 86.0% of the studied subjects were satisfied with participating in the counseling sessions due to improvement of their mis-conceptual information of health behavior. Conclusion: In essence, the present study concludes that a significant improvement among rural patients' information, health behavior and their satisfaction as a result of their participation in counseling sessions. Recommendations: Generalize the results of this study to all maternity health services all over Egypt.
Keywords: Abortion, Habitual abortion, Counseling, Satisfaction, Health behavior
Cite this paper: Mirfat Mohamed Labib El-Kashif , Howaida Amin Hassan Fahmy Elsabaa , Mageda Abdelaty Soliman , Effect of Evidence-based Counseling on Improving Rural Patients' Information, Health Behavior and Their Satisfaction Regarding the Habitual Abortion, International Journal of Nursing Science, Vol. 10 No. 1, 2020, pp. 25-32. doi: 10.5923/j.nursing.20201001.03.
Article Outline
1. Introduction
- Abortions are considered a serious reproductive issue with a higher incidence in developing countries than in developed one [1]. Globally, the incidence of early pregnancy loss after implantation is 31%. The most common cause of early pregnancy loss is a spontaneous miscarriage [2]. Habitual abortion (HA) is one of the spontaneous abortions and an important reproductive issue that affects the emotional and physical aspects of the couple in addition to that it is a problematic situation for the obstetrician to handle [3,4,5]. HA refers to two or more loses of pregnancy conceptus before the 20th weeks that confirmed by ultrasound or histopathology of pregnancy products [6]. The habitual abortion affects 5% of couples trying to conceive and does not include biochemical, ectopic pregnancies and pregnancies of a specific place [2]. Also, HA occurs simultaneously and almost at the same stage of pregnancy [7,8]. However, habitual abortion is one of the most critical debated reproductive issues which its underlying mechanisms are poorly understood. The known etiologic factors for HA are fetal genetic factors, anatomical uterine factors, endocrine factors, thrombophilic factors, autoimmune factors, and maternal infection factors. However, approximately 50% among couples do not manifest a clear cause which is referred to as unexplained habitual abortion [9].Infection, incomplete evacuation of the products of conception, haemorrhage and injury from the surgical procedures itself are the most common complications of habitual abortion [10]. The management of habitual abortion is individualized, considering couples' history and the presence or absence of risk factors, reassurance, psychological and emotional support, and post-abortion counseling [11].Nurses play multidisciplinary roles as direct care provider starting from history taking, physical examinations, considering causes of habitual abortion, and finally immediately intervention to utilize best evidence research findings as a base for her/his competent immediate care providing for a patient with habitual abortion to avoid complications and minimize maternal mortality and morbidity [12]. The nurses, as a counselor and health educator, must implement post habitual abortion counseling for each aborted patient. The counseling is defined as face to face communications and the application of mental health, psychological or human development principles, through cognitive, affective, behavioral or systemic interventions strategies that address wellness, personal growth, or career development as well as pathology. Also, counseling is a principled relationship characterized by the application of one or more psychological theories and a recognized set of communication skills, modified by experience, initiation and other interpersonal factors, to clients’ intimate concerns, problems or aspirations. Its’ predominant ethos entails facilitation rather than an advice-giving or coercion exercised. Counseling may take short or long duration, take place in an organizational or private practice setting and may or may not overlap with practical, medical and other matters of personal welfare. To complete the counseling steps; the counsellor should take informed consent from the client as the client should recognize the complete process of counseling and provide agreement to it [13,14,15].Moreover, post habitual abortion counseling becomes extremely important for promoting patients' mental health because nurse counselor has a critical effect on how the women feel after habitual abortion and correcting patients' misconception and belief related to unhealthy daily habits regarding habitual abortion [16]. Additionally, nurse as counselor and administrator establishes post-abortion counseling group while nurse as a researcher must design, implement, and collaborate with other researchers to implement evidence-based research [17]. The counselor role is to support women feelings and emotions and encourage them in planning for care needed.Patient satisfaction is an essential and significant indicator for measuring the quality of health care and the success of care providers and facilities. Evaluating client satisfaction with health care services and counseling provided after experienced abortion is clinically relevant, and it is the responsibility of higher authorities and staff in the health care system.Significant of the study: -Habitual abortion is considered as a confusing multifactorial reproductive disorder which is a stress state that leads to emotional and psychological distributions among couples. According to 2010–2014 global statistics, the average of abortions incidents is estimated 56 million abortions occurred worldwide each year, 49.3 million in developing regions and 6.6 million in a developed one. Overall, 35 abortions occur each year per 1,000 women aged 15–44 worldwide. 25% of all pregnancies ended in abortion [18]. In Egypt, it was estimated that 2,542 maternal deaths due to unsafe abortions [19].The counseling provision should be a complementary part of comprehensive post-abortion care. However, most post-abortion counseling focuses mainly on post-abortion family planning and don't cover virtual client needs to handle other reproductive health needs, both of which are critical elements of post-abortion counseling. This study is intended to provide the proper information and counseling needs of the post-abortion client. Moreover, the present study depends on the active client participation approach. Active client participation is a significant component of patient-centred care. The literature has found that active clients call for information more effectively, discuss with health providers more about their health status, and prove the information they gained from health providers as well as assisting with decision-making regarding their treatment. Furthermore, the results of this study will guide the post portion care providers to use the decision making based on evidence-based intervention to set treatment priorities regarding the phenomenon of habitual abortion and its impact of family life.Research hypothesis: women who received post habitual abortion counseling, her information improved, she followed daily health behavior and felt more satisfied.
2. The Aim of the Study
- This study aimed to investigate the effect of evidence-based counseling on improving rural patients' information, health behavior and their satisfaction regarding the habitual abortionDesign: - Research design: A Quasi-experimental involves intervention pre and post-test study.Sample/Participants: - The study was conducted at obstetric and gynaecological inpatient departments and outpatient maternity clinics in Benha university hospital and ministry of health hospital, Qaliubiya governorate. 119 patients, five were excluded for their participation in the pilot study; the final total is 114.Sample type: A purposive sample was employed.Inclusion Criteria:• Rural aborted females with more than two consecutive abortions. • Age more than 18 and less than 40 years.• Free from medical and gynaecological problems. • Literate female.Tools of data collections: -- Standardized tools were used to collect data after obtained informed consent from all participants. The tools were collected from five of the target sample of the study who has fulfilled the inclusion criteria to test applicability and clarity. Appropriate modifications were made to the research tools according to the results of the pre-test. The standardized tools were divided into the following:First tool: Concerning with women' level of education, area of residence and cause for attending hospital. Second tool: adopted from ESHRE guidelines tools about recurrent pregnancy loss (The European Society of Human Reproduction and Embryology), 2018 [20]: The guideline includes 38 recommendations on habitual abortion risk factors, prevention and investigations, and 39 recommendations on treatments of habitual abortion. This guideline provides 60 evidence-based recommendations; – of which 31 recommendations were recognized as strong; and 29 as conditional; and 17 points of good practice. This tool assesses the following;1- Patients' information regarding habitual abortion as (the definition of habitual abortion, risk factors of habitual abortion, complications, investigation and management as well as their immediate intervention and the consulted person for habitual abortion. Also, the participant information regarding female and male reproductive systems.2- Health behaviour relevant to the risk of habitual abortion as (Cigarette smoking, smoking shisha, drinking coffee, hard activities, sitting in hot water for relaxation, perineal hygiene from down to up, eating spicy food and salted fish, avoid the daily bath post-abortion, sleep 8-9 hours and Practicing daily walking exercise). Identify patients 'learning needs, mis-concepts and problems.The third tool: Assesses patients’ misconception and believes related to habitual abortion as; habitual abortion leads to (losing femininity, loss of family trust, lead to divorce, God punishment). The women are practicing breast self-examination or not. The preferable place of delivery for the women; (at home by uncertified midwives or hospital delivery). The immediately consulted person for habitual abortion called by women; (uncertified midwives, old senior women in the family, health care provider and close friends).The fourth tool: follows up card, including researcher' telephone number, schedule of follow up visit, as well as hospital discharge information such as medication administration and laboratory investigation.The information scoring system:- for answering all questions, each correct answer was given"1 score" and "0 scores" for an incorrect answer. The total information correct score was (≥60%) while the total information for the incorrect score was (<60%). The "Patient Satisfaction tool" Scoring system: a 5-point Likert scale include complete satisfaction, somewhat satisfied, neutral, relatively un- satisfaction, and completely un-satisfaction. These will respectively score 5,4,3,2 and 1. While; higher scores indicate greater satisfaction with the procedure is ≥60%, and the lower scores <60% indicate un-satisfaction with the process. Cronbach’s alpha coefficient (0.75) used to evaluate the reliability of the tool.Content validity and reliability:All tools of data collections were developed and sent to six specialized university Professors in the field of maternity nursing and nursing administration. According to their comments, modifications were made.Ethical consideration: -The Ethical Committee approved the present study at the Faculty of Nursing; Port Said University. After clarifying the aim of the study to the participants, all of them were given informed consent according to the Declaration of Helsinki II, the second version. Fieldwork or Operational design: The study was implemented through three phases, including preparatory, implementation and evaluation phase:Phase one (preparation phase):The researcher had reviewed the current advanced national and international literature related to the study topic and then prepared the tools for data collection. All tools of data collection utilize pre-intervention then four weeks' post-intervention except satisfaction tools which were utilized four weeks' post-intervention only and finally implemented the pilot study on five patients who were excluded from the total number of participants.Phase two (implementation phase):The researcher interviewed one to three patients (as a group) every day according to the sequence of their attendance in the hospital registration book and explained the aim of the study to obtain their oral consent. The interview was conducted in a separate place to maintain the confidentiality of the study. The duration of each interview is a half-hour. The counseling sessions were implemented through 9 sessions for each patients group with a duration of 20 minutes for each session. Four sessions were devoted to theoretical learning, and five sessions were implemented for women training. The methods of teaching include group discussion, lectures, brainstorming, demonstration, role play and bedside teaching. The training sessions involved media use, such as a lab-top computer, flip chart, audio-visual aids, and data show presentation.- The researchers follow the elements of counseling for women with habitual abortion miscarriage which include: - recognition of the patient as an individual, selecting a time for questions, good listening, respect: for the patient, her husband and their circumstances, precise and sensitive language, honesty and avoid false reassurance, shared planning, supportive care in the next pregnancy and kindness Musters et al. [21].- The contents of the counseling were given to the participants after asses their information and health behavior relevant to the risk of habitual abortion. The researchers explain any queries with them through counseling elements. Then participants knowledge, health behavior were assessed immediately after counseling. Finally, the participants' satisfaction was assessed after counseling implementation to investigate the level of participants satisfaction regarding the counseling process.Phase three (evaluation Phase):In this phase, the nurse administrator researcher was responsible for collecting data pre, and four weeks' post-intervention, but patient' satisfaction was utilized four weeks' post-intervention only. The researcher conducted this phase using the pre-intervention tools.Data analyses:The collected data were tabulated and statistically analyzed using an IBM computer and the statistical package for social science (SPSS) advanced statistics, version 23 (SPSS Inc., Chicago, IL). Numerical data were expressed as mean and standard deviation. Qualitative data were expressed as frequency and percentage. Bivariate correlation (two-tailed Pearson correlation) was used to test the correlation between numerical variables. The observed differences and associations were considered as the following: Not significant (NS) P>0.05, Significant (S) P<0.05*, High significant (HS) P<0.001**.
3. Results
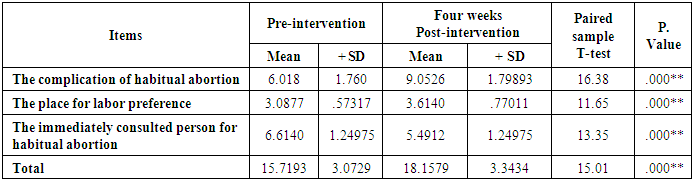
- Table (1) reveals that there is a marked improvement in patients' information four weeks' post-implementation of post habitual abortion counseling sessions compared to pre-intervention related to habitual abortion. The studied sample` information includes the definition of habitual abortion, complications of habitual abortion, investigation and management of habitual abortion—also, the information regarding male and female reproductive systems post-intervention.
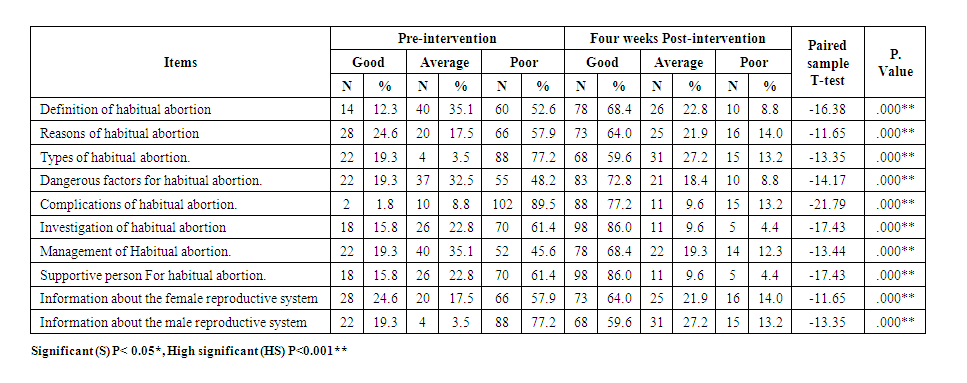 | Table (1). Frequency distribution according to the studied subjects' information related to habitual abortion pre and four weeks' post-intervention. (n=114) |
|
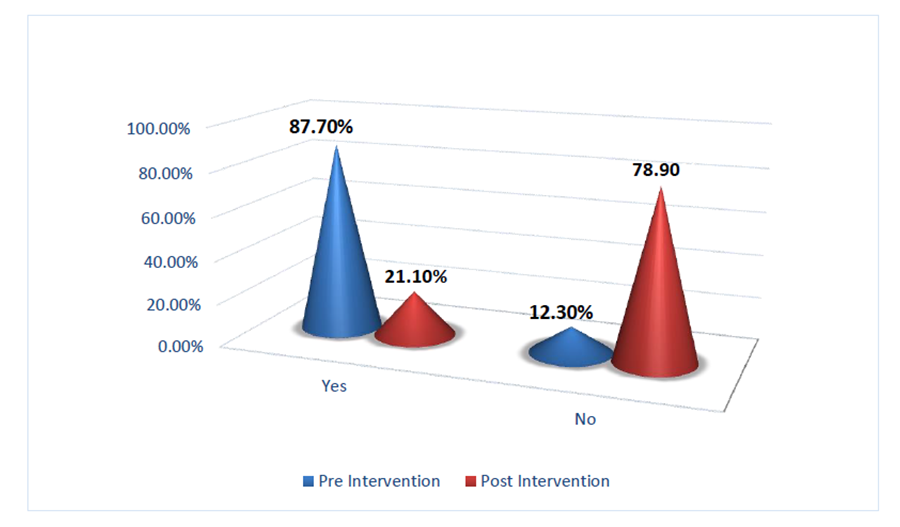 | Figure (1). Percentage distribution according to the studied subjects' total health behavior related to habitual abortion pre-intervention compared to four weeks' post-intervention. (n=114) |
|
|
|
4. Discussion
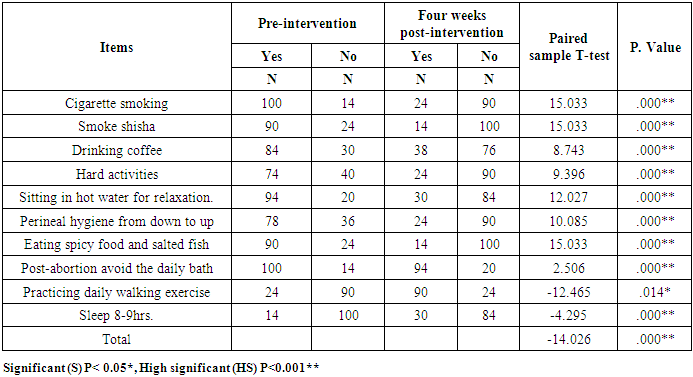
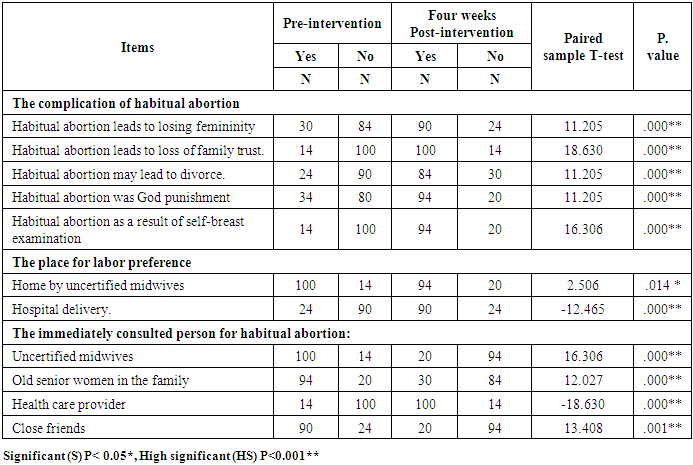
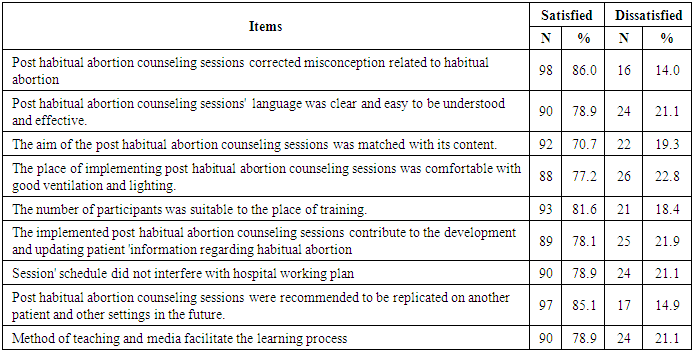
- Unexplained habitual miscarriage is considered a stressful situation. Nowadays, supportive care is the only evidence-based assistant cares that can be given to couple complain from habitual miscarriage. Counseling and systemic monitoring have a beneficial effect in increasing live birth rate and assess the potential risk of habitual miscarriage [21,22,23]. As mentioned earlier, this study aims to investigate the effect of evidence-based counseling on improving rural patients' information, health behavior and their satisfaction regarding the habitual abortion. This aim was significantly approved within the framework of the present study's research hypothesis, which suggests that women, who received post habitual abortion counseling her information improved, she followed health behavior. She felt more satisfied compared to women who did not receive counseling. The results of this study reveal that there is a highly statistically significant improvement of patient's information four weeks' post-intervention compared to pre-intervention. This is in agreement with Saad et al. [8] who pointed out that, there was a highly statistically significant difference between pre and post-intervention among patient' knowledge regarding habitual abortion. Also, according to Rehnström et al. [10], who illustrated that there was a highly significant improvement among patient' knowledge regarding habitual abortion post habitual abortion counseling sessions.The Couples with habitual abortion should be counselled about the negative effect of alcohol use, smoking, obesity and strenuous exercise on pregnancy and could harm their likelihood of live birth. So that stopping of tobacco, maintain healthy body weight, give up alcohol intake and a follow the regular pattern of exercise is recommended [24-28]. In compliance with the previous approach, the present study found highly significant improvement among the participants’ unhealthy behavior pre-intervention compared to four weeks post counseling sessions Wu et al. [29] support this result who reported that the effect of post-abortion counseling on women health behavior which found that a highly significant improvement among studied subjects post -counseling sessions. It was also recommended in the previous study to replicate these sessions in other regions of the country, especially rural areas, because women in rural areas had lack knowledge related to habitual abortion. Additionally, this result was in the same line with the study of Fetters et al. [30] who illustrated that the counseling sessions lead to improvement and correction of unhealthy daily habits among the studied subjects. It is evident in the present study that the correction and improvement of patient' information related to post -habitual abortion counseling which is reflected in the alteration of unhealthy behavior four weeks' post-intervention.Additionally, the present study brings our attention toward correcting the participants’ misconception related to their habitual abortion because the majority of the participants have misconceptions such as habitual abortion may lead to loss of motherhood, loss of femininity and may lead to divorce. Habitual abortion is associated with the feeling of low self-esteem, hopeless and loss of family trust. Also, habitual abortion is associated with God punishment. This result supported by Stewart et al. [31] who illustrated that the majority among patients who had misconception around reasons related to habitual abortion as some women feel that they are being punished related to demonic activity and eating forbidden foods. It is immoral in our rural Egyptian areas to discuss issues related to reproductive health among married and unmarried young rural females. Therefore, nurse administrator and midwives must design and implement programs to correct misconception and unhealthy behavior among young rural females concerning the promotion of female reproductive health. The counsellor should show understanding, good listening skills, honestly, awareness of the patient’s obstetric history and respect towards her previous pregnancy losses. It is appreciated that the counsellor should recognize the patient as a unique individual, recognize the time of questions, information, repetition and discussion. The counsellor should use a clear and sensitive language and provide supportive care with kindness manner [21]. In line with the previous context, the majority among the participants in the present study were highly satisfied with the implemented post -habitual abortion counseling sessions, which self-reported that the post- habitual abortion counseling sessions 'language was easily understood, and the aim was matched with its content'. Also, the place of implemented post habitual abortion counseling sessions was comfortable with good ventilation and lighting. Additionally, the implemented post habitual abortion counseling sessions contribute to correct misconception related to habitual abortion and contribute to the development and updates with the innovative information regarding habitual abortion with the method of teaching and media facilitate the learning process.Furthermore, the majority among the participants suggested replicating the present study post- habitual abortion counseling sessions on another setting to other broader subjects in the future to enhance women' information and unhealthy daily habits. It was surprising to find a highly positive satisfaction among the studied subjects; this was due to the effectiveness and efficacy of the implementation of counseling sessions because counseling was conducted face to face which easily facilitate correction of unhealthy behavior and misconception among the participants which are seen highly effective in changing unhealthy behavior among the clients. So, the present study stresses the importance of replicating counseling sessions for another setting on larger subjects.
5. Conclusions
- The present study concludes that a significant improvement in rural patients' information, health behavior and their satisfaction due to the implementation of counseling sessions.
6. Recommendations
- Based on the results of the present study, the following are recommended:1- Design and implement a post-abortion counseling program for rural women who are undergoing a habitual abortion. 2- Generalize the present study results to all maternity health services all over Egypt. 3- Nurse administrator must establish a counseling support group unit to correct patient' mis-concept and unhealthy daily habits.Further study:4- Investigate the effect of counseling sessions on improving women in childbearing age quality of life.
ACKNOWLEDGEMENTS
- The authors would like to thank all women who enthusiastically participated in this study.