-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2019; 9(3): 53-64
doi:10.5923/j.nursing.20190903.01

Effectiveness of a Multimedia Educational Package for Cancer Patients with Colostomy on Their Performance, Quality of Life & Body Image
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShereen Ahmed Ahmed Qalawa1, Maha Moussa Mohamed Moussa2
1Assistant Professor of Medical-Surgical Nursing, Faculty of Nursing, Port-Said University, Egypt
2Assistant Professor of Community Health Nursing, Faculty of Nursing, Port-Said University, Egypt
Correspondence to: Shereen Ahmed Ahmed Qalawa, Assistant Professor of Medical-Surgical Nursing, Faculty of Nursing, Port-Said University, Egypt.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

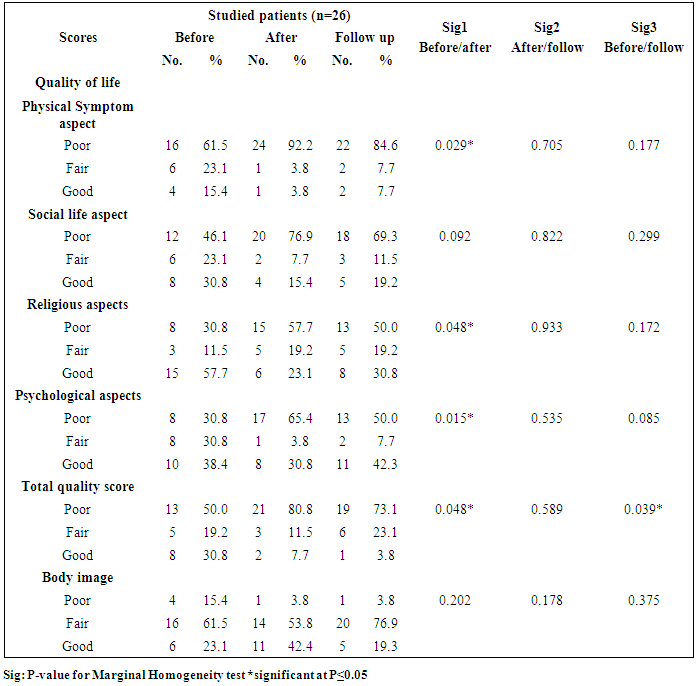
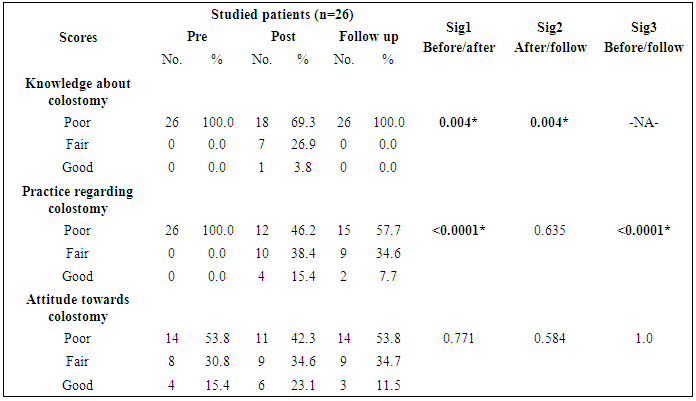
Background: Colostomy is considered as an artificial opening of the colon onto the abdominal surface. Conversely, the person with an ostomy may point up on the negative aspects of the stoma rather than its function to the loss of self-image, acceptance of a new lifestyle, and ability to self-care. Aim: To evaluate the effect of a multimedia educational package for patients with colostomy. Subjects and methods: The design: Quasi experimental design was utilized in this study. Setting: It was conducted at outpatient clinic of oncology institute in Damietta. Purposive sample included (26) patients with colostomy. Tools: used for data collection included fifth tools as follows: the first tool; socio-demographic of colostomized patient's and knowledge assessment regarding colorectal cancer, colostomy indication, types, duration, the second tool; for assessment of patient's attitude and actions towards colostomy care and positive actions in various situations while the third tool; for patient's Observational checklist of colostomy care practice, the fourth tool; for patient's quality of life assessment, the last tool; for patient's body image perception assessment questionnaire. Results: reflected that there is a statistically significant difference in patient's level of knowledge regarding colostomy between pretest and posttest and between post -test and follow-up phase with p-value of 0.004. While there are no statistically significant differences was found in colostomized patient's attitude among all phase of educational. On the other hand, there are a statistically significant difference in patient's practice of colostomy care were found only between pretest and follow-up phases with p-value of 0.0001. additionally, there are a statistically significant difference were found among colostomized patient's regarding all quality of life domains between post-test and follow-up phases in comparing with pre-test phase except for social domain with p-value of 0.092. While there are no statistically significant difference was found among colostomized patient's regarding their perception of body image between post-test and follow-up phases in comparing with pre-test phase with p-value of 0.202. Conclusion &recommendations: Based on study results the implementation of multimedia educational pakage for colostomized patients showed a remarkable increase and improvement of the patient 's level of knowledge and acquiring the ultimate positive and noticeable improvement in the patient's positive actions towards colostomy care, prevention of complications that has direct effect on their quality of life and body image, also, there are obvious needs for instructional scheme or guidelines accessible on simple media to those patients to minimize complications postoperatively and increased patient's coping and adherence with their cancer treatment modalities and colostomy care. Efforts should be carried out to design and implement interventions that outfit oncology centers and institutes with field evidence and increased facilities, patient's education approach, and documentations of noncompliance cancer patients withier disease, self-care and follow-up appointments.
Keywords: Effectiveness, Multimedia, Educational package, Colostomy, Performance, Quality of life, Body image
Cite this paper: Shereen Ahmed Ahmed Qalawa, Maha Moussa Mohamed Moussa, Effectiveness of a Multimedia Educational Package for Cancer Patients with Colostomy on Their Performance, Quality of Life & Body Image, International Journal of Nursing Science, Vol. 9 No. 3, 2019, pp. 53-64. doi: 10.5923/j.nursing.20190903.01.
Article Outline
1. Introduction
- Colorectal cancer is considered as one of the frequently common cancer diagnoses and undergoing colorectal cancer surgery is reported to be linked with physical symptoms and psychological reactions. [1]. According to Cancer Research UK, 2014 Colorectal cancer (CRC) is predictable approximately 41,000 cases in the UK annually and considered the fourth most common cancer in the UK with 95% of cases occurring in people aged 50 and over. An ostomy refers to the surgically produced opening in the body for the discharge of body wastes. For cancer, ostomies are most commonly placed for rectal cancers (colostomy, ileostomy), followed by bladder cancers (urostomy) [2]. Ostomies may be required in other cancers for the management of huge, metastatic disease or for emergencies such as perforation or obstructions. In 90% of low-mid rectal cancers, an anastomosis is accompanied by a temporary (“protective”) diverting ileostomy; this is later reversed in a second surgery [3]. A temporary ostomy allows the anastomosis to heal, and prevents catastrophic complications. In some cases, temporary ostomies may become permanent long-term as a result of chief co-morbidities and complications, such as anastomotic leaks orstrictures. The treatment decision making method for ostomy surgery is complex. (Fig 1) [4].
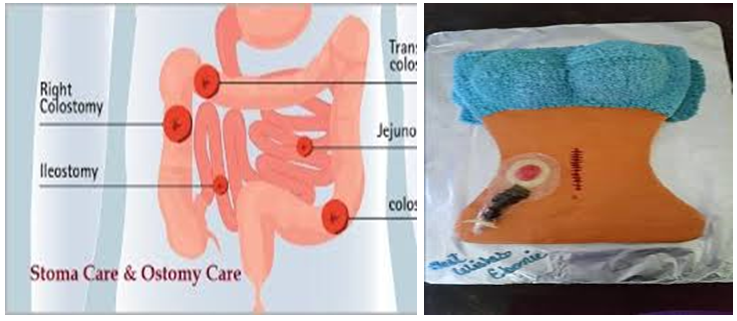 | Figure 1. (Sun et al, 2018) |
2. Subjects and Methods
- A-Technical Design:Include description of the research design used, the study setting, the subject, and the tools of data collection.1-Research Design:A quasi experimental research design was utilized in this study.Setting:This study was conducted inoutpatient clinic at Institution of Oncology in Damietta.Subject:The purposive sample of this study included (26) patients of all available newly both sex adult colostomized patients. They enrolled in this study according to the following inclusion criteria; adult patient males and female, accepted to participate in the study, able to realize and communicate, free from other chronic diseases such as hypertension and diabetes mellitus. They were interviewed by the researchers.Study tools:Data collected by using five validated adapted tools from Rattanajarana [17] & Youngberg [18] after translation to Arabic language and make some modifications to be suitable for population, beliefs, values, culture. Structured interview questionnaire for assess patient’s knowledge, practice, and attitude regarding colostomy and it's care. Fifth tools were used for data collection. The following tools were used to collect data related to this study:Tool I: Structured interview questionnaire sheet; this tool includes two parts.The first part includes 9 items to assess patient's socio-demographic characteristics such as age, sex, educational status, marital status, types and duration of colostomy, residence, family numbers.The secondpart includes 37 items to assess patient's knowledge and perceptions regarding colostomy indications and care as proper diet, suitable caring for colostomy.Tool II: (Assessment of colostomy patient's attitude scale: This tool was used to assess the patient's attitude towards colostomy care and positive action, preventive measures in various situations as bathing, dressing, exercises, warning signs. There was a total of 12 items in the attitude scale using 3 point likert scale of (poor, fair and good).Tool III: patient's practice assessment sheet. It includes adopted validated observational checklist based on Medical Surgical Nursing Critical Thinking for patient centered care, 2014 to assess the patient practice of colostomy care, irrigation, bags changes.Tool IV: Quality of life – Model for Ostomy Patients. It includes nine items related to clinical manifestations that interference with good quality of life as rashes, itching, pain, diarrhea, constipation, exhausted etc,,,, then the quality of life scale based on (City of Hope Quality of Life Model for Ostomy Patients, 2004) [19] it contains 39 items used to assess four domains as Physical, Social, Psychological, and Spiritual Well-Being.Tool V: An Imagery Profile for body image sheet derived from Pilarski [20], it Includes 25 items to assess patient's perception of body image after colostomy.Scoring system:The scoring systems for Toolsclassified as good for above 75%, fair 75-50%, poor ≤ 50% (City of Hope Quality of Life Model for Ostomy Patients, 2004) [19].Multimedia educational packageThe multimedia educational package is an intervention was developed in a simple Arabic language. The objective of the educationalThe aim of the educational was to improve knowledge, practices, quality of life and body image of colostomy patients by using a multimedia educational package.The content of the multimedia educational:In the present study, the multimedia educational program had two sections. The first consisted of knowledge about the process of stoma formation, including anatomy and physiology of stoma, definition, complications and the clinical indications for stoma formation through PowerPoint. Furthermore, the second section focused on the practices related to the various central elements of stoma care, medication, diet, exercises and self-examination of stoma through the researchers using graphics, posters, video and pictures to demonstrate and reinforce the information and skills.Procedure:-Educational package of colostomy care implemented through using three phases involves the preparatory phase, filed work and evaluation phase.First phase preparatory or assessment phase:- A review of advanced national and international related literature Guideline and available published information using books, articles, magazines, and internet to develop the study tools for data collection. Development of multi educational package program using developed standardized instructional guidelines based on Varghese [21], Basiony [22] & Prince sultan medical military city for health education [23], Hooper [24].- Study tools were revised by five professors from Medical- surgical nursing and Community health nursing, oncology expertise as a jury to test its content validity and feasibility and necessary modification were done.- The tool reliability was tests through Cronach alpha coefficient as follows: Split half method was used for both knowledge and attitude tool. Reliability coefficient ‘r’ was calculated using Karl Pearson’s coefficient. The reliability coefficient was 0.89 and 0.92 for knowledge and perception tool and attitude scale respectively. Reliability for attitude scale was established with Inter rater Intra rater method. The correlation co-efficient ‘r’ was calculated using inter class correlation. The reliability co –efficient was 0.90. Hence the structured knowledge and attitude scale was considered to be reliable for the present study.- A pilot study will be carried out on 10% (3) of patients to test clarity feasibility and applicability of the tools then necessary modifications were done according to the finding results of the pilot study and expertise opinions. Otherwise, these patients were then excluded from the sample of research work to assure the stability of answers.Filed work:- The researchers visit the outpatient clinic of oncology institute in Damietta for reviewing health records to recognize colostomy patients and insure of study criteria.- Assessment of the patients was done through visit at outpatient clinic by using all structured interview questionnaires for assess patient’s knowledge, practice, and attitude regarding colostomy and it's care pretest. The questionnaire was initially prepared in English then translated in to local language (Arabic) by researcher and other person then it was translated back to English by a different person to ensure consistency. The researcher first collect data regarding patient's demographic data, then ask about medical history after that the researcher assess ostomy self-care by using observational checklist about ostomy self-care practices. The duration of assessment for each one tool took about 15 to 20 minutes.- Planning and development: Patient's practice and self-care educational was planned and designed by researcher based on the result of the assessment phase. Determining teaching and learning activities include the following: Creating interest by motivating and reinforcing participatory discussion and conduct program according to the available facilities in the outpatient clinic of institute in Damietta as meeting or classroom / waiting patient's room which considered adequate to conduct the program. Also, prepare the multimedia allows researchers to integrate or using to easy teaching the patient such as computer, data show, graphics, audio, video, internet, animation, posters and other media into one package to present comprehensive information. Prepare the booklet of information about colostomy and self-care practice was designed in Arabic.- Implementation: participants the subjects of the study group were divided into small groups and the education groups comprised of 6 to 7 participants are taken in each visit. The implementation of the self-care program was done for each group separately. This phase using simple clarified multi media of education previous above mention as pamphlets and posters, videos….etc. when the patient absent the session the researchers demonstrated the component of the program in the presence of one of the family members of the patient and asked them to act as patient's reminder, support provider and help the patient in performing ostomy care. Also, practice assessed by using the observational checklist to assess the patient practice of colostomy care, irrigation, bags changes.- The study was conducted over a period of 11 months beginning at March 2016 until the end of January 2017 according to availability of patient's follow-up schedule, purpose of the study was explained prior to get the questionnaire, and needed time to answer ranged from 30 - 45 minutes. The researcher visited the outpatient clinic of oncology institute in Damiettain morning shift from 9:00 AM to 12.00 AM for two days / weekly (Saturday and Tuesday). The time was suitable for the researcher. The researcher at a suitable place in the outpatient class room to educational multimedia package was conducted in three sessions (1 educational and 2 practical / training sessions) program was implemented over 4 weeks period, 2 sessions per week; the duration of each session was 30 minutes; the first session describe the colostomy definition, indications, types, proper foods; the second session regarding caring of colostomy bag and bathing, suitable dressing, exercises, the last session for corrective action when facing discharge, itching and warning signs as a preventive measures.Ethical ConsiderationsVerbal informed consent was taken from all patients join in the study. Names of respondents were not being use in the study results. The confidentiality of the information gather was assured. Their right of refusal to participate in the study was respect and letter submitted to the director of oncology institute at Damietta and written permission was taken from Management Committee of oncology institute for data collection.Evaluation of the program:This was done immediately after implementation of multimedia educational. This phase includes evaluation of effectiveness of educational multimedia program after one month through using the same structure interview sheet which used in pre-test phase regarding knowledge, practice, attitude, body image and Quality of life assessment sheet (Post test phase). Then, another test (Follow-up phase) was carried out after 6 months to evaluate retention of gaining knowledge, practice, attitude, body image and quality of life assessment sheet after6 months through using the same structure interview sheet which used in pre and post-test phase.Statistical Design:Data were revised, coded, entered, analyzed and tabulated using SPSS version 20. Both descriptive statistics (frequency, percentage) and inferential statistics (chi-square test, Pearson Correlation Coefficient test were used according to type of variables. Statistical significance was considered at P-value ≤ 0.05.
3. Results
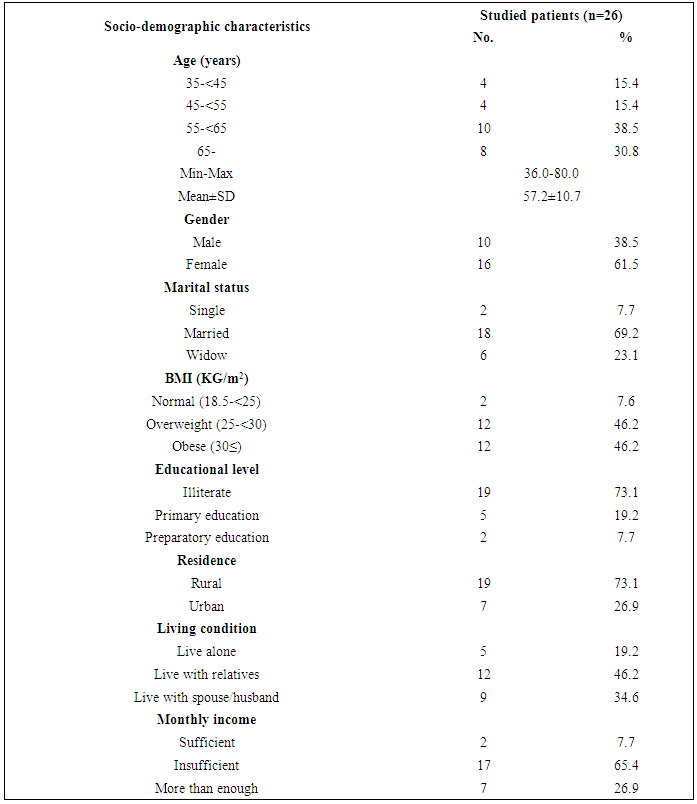
- Table (1) shows that more than one quarter of patients (38.5%) were male in age group 45-65 years. Also, (69.2%) were married, (73.1%) were illiterate, (73.1%) residence in rural region, (46.2%) of them living with their relatives and (65.4%) of them had insufficient income.
|
|
|
|
|
|
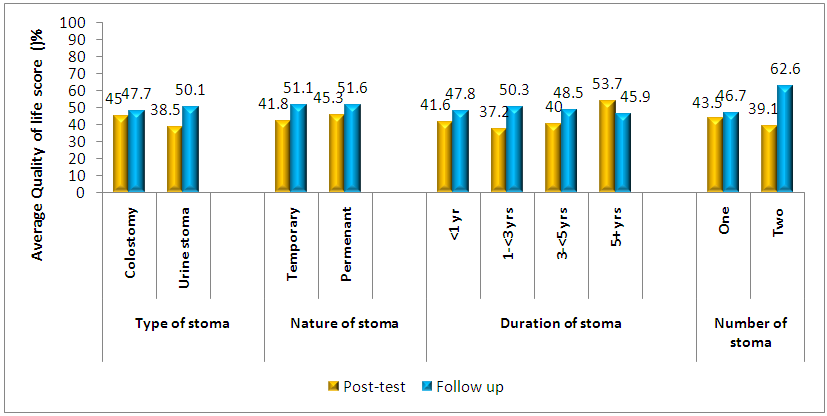 | Figure (2). Correlation between charcteristics of the stoma and the average Quality of life score in post and follow-up implimentation of programme phases |
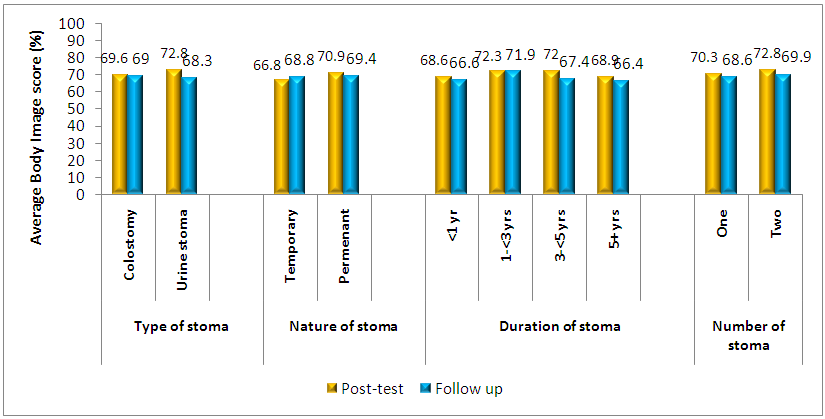 | Figure (3). Correlation between charcteristics of the stoma and the average Body image score in post and follow-up implementation of programme phases |
4. Discussion
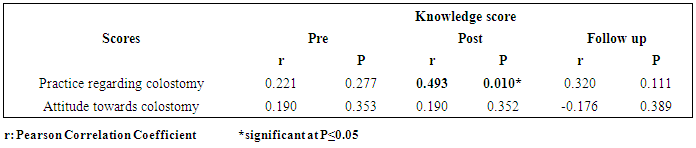
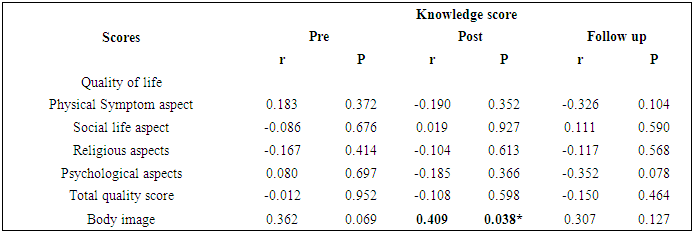
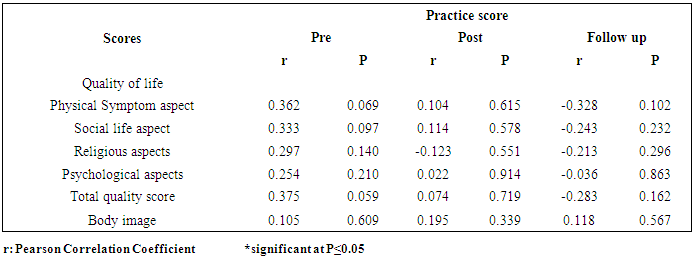
- A colostomy is not a disease, but a change in the approach body works. Every year there are many people who undertake ostomy surgery that alters their normal passage of elimination which needs direct care to patients with abdominal stomas, fistula, draining wounds, drains, and incontinence as an educator, consultant and researcher with extra knowledge, exacting skills and attitudes.Browne [25] mentioned that improving the practice and support for cancer survivors are the major priorities and concentrate on personalized care planning, self-management, and adapted support. However, there is little research about the care of long-term cancer survivors in primary care and suggests the preventative and chronic care is enhanced for long-term colorectal cancer survivors.Concerning socio-demographic characteristics of studied sample, the present study revealed that more than one quarter of nurses of patients more one third were male in age group 45-65 years. Also, more two thirds were married, the most of studied sample were illiterate, also residence in rural region, less half of them living with their relatives and more two thirds of them had insufficient income.Regarding the effectiveness of multimedia educational package on quality of life and body image among patient with colostomy, the present study revealed that there are a statistically significant difference were found among colostomized patient's regarding all quality of life domains at post-test and follow-up phases in comparing with pre-test phase except for social domain. While there are no statistically significant difference was found among colostomized patient's regarding their perception of body image at post-test and follow-up phases in comparing with pre-test phase. These findings goes in the same way with Zhang et al [26] who Concluded that the general health condition and dimensions of QOL among Chinese people were significantly correlated with ADS and all of QOL dimensions (P <0.05). Which the health condition related QOL include recognition of disability, and social relational quality of colostomy patients were exactingly related. So, the patient should work to form rational morals and close bonds with families and friends to achieve a better QOL.On the other hand, Maydick [27] discovered in Long Island, USA that living with an ostomy influences patient's QoL which a significant difference in QoL was dependent on who manifest the site; the surgeon-marked group and (WOC) nurse-marked group had the highest QoL scores when compared to the “other” group. As well, Liao and Qin [13] Concluded that QOL among Beijing patients with a stoma was not ideal. So that, stoma implantation, improvements in self-care and interesting wish in patients played a vital role in bettering their stoma-QOL. Concerning effectiveness of multimedia educational package on colostomized patient knowledge, attitude and practice, the present study revealed that there are a statistically significant difference in patient's level of knowledge regarding colostomy between pretest and posttest and between post -test and follow-up phases. While there are no statistically significant differences was found in colostomized patient's attitude among all phase of educational programe. On the other hand, there are a statistically significant difference in patient's practice of colostomy care were found only between pretest and follow-up phases. These findings supported with Mohamed et al [28] who accomplished that there was a highly significant statistically improvement in all items of knowledge, practices and self-efficacy at pre/post program of self-care management among egyptian colostomy patients and reported that Self-care management program is critical to verify of clients’ knowledge; practical and emotional requirements are met. In Turkey, owing to lack of stoma care nurses, clinical nurses have chief duties and responsibilities about education of patients in process of getting used to living with stomas. These duties and tasks are giving self- care education about technical skills related to wound care and incontinence (skin cleansing, bag / adapter replacement, changing dressings, making the proper position etc.), giving support and handling individuals in taking a correct decisions related their treatment and care, organizing instructional programs for daily activities to make confident compliance with the social life of patients, developing training materials and suitable media, teaching support systems and so on. [29] While, In Australia, Waller et al [30] highlighted on that Pre-operative education can improve satisfaction, knowledge and decrease anxiety.Concerning relationship between colostomized patient's knowledge and quality of life domains, the present study revealed that there are a negative Correlation were found between patient's knowledge scores and the religious domain of quality of life between all phases of program implementation, also there are negative correlation were found in physical symptoms and psychological domain between post and follow-up multimedia package implementation while there are no correlation was found in social domain between post and follow-up implementation of program while there are a positive correlation was found between patient's knowledge and their body image scores only in post multimedia package implementation phases. These findings goes in the same line with Sivakumar [31] in Chennai who found that that ostomy affects one’s religious activities because the society do not accept a person to enter in to the temple with fecal matter in the bag. Accordingly, patients themselves restrain from these type of activities. In our study 90% of patients do not participating in the religious activities, only 10% of patients continue to participate in the religious activities. While, In Indonesia, The overall quality of life of the patient is affected which positively affect colostomized patients quality of life and the obtainable knowledge of ostomy-related harms. [32]Regarding the relationship between colostomized patient's practice with their quality of life and body image, the current study revealed that that there are a negative correlation were found between colostomized patient's practice scores and the religious domain of quality of life between post and follow-up multimedia educational implementation while there are no correlation was found in social and psychological domain between pre and post implementation of program while there are no correlation was found between colostomized patient's practice and their body image scores in all phases of program implementation. These findings goes in the same way with Sun et al [4] who recommended from USA that the Ostomy Self-management Training (OSMT) program OSMT program has high likely to make a positive impact on the cancer patient's acceptance of their physical changes, psychological, social, and spiritual needs to let them living with a permanent ostomy. Besides, In Turkey, Culha et al, [29] meaningful of that stoma management, planning of health, self-care competence and patient centered education with using evident stoma Care and Management Guideline. Also, stoma care nurses; clinical nurses have major duties and responsibilities about education of those patients in process of getting used to living with stoma.Concerning stoma characteristics, the present study revealed that there are a positive correlation were found between characteristics of the stoma and the average Quality of life score between post and follow-up implementation of educational in items related to types, nature, and numbers of stoma. these findings goes in contrast with Youngberg and Rita [18] who painted on that preoperative stoma site marking was not significantly associated with QOL total scores among Columbian patients above and beyond other variables; increased ratings of financial adversity were associated with decreased QOL total scores after controlling for age and time in view of the fact last surgery; respondents with irritant contact dermatitis as a complication reported significantly lower QOL total scores than those without irritant contact dermatitis; the number of complications was negatively associated with QOL. Thus, there are a significant improvement for individuals with a permanent ostomy with ideal nursing practice in order to help of climbing some issues facing ostomypatients.Moreover, Gao [33] in Chennai stated that the new stoma patients’ concerns in post – operative rehabilitation includes occupational complexity that can lead to economic stress, fear for social inequality that is caused by lack of social support, fear for stoma appearance, and fears for daily life. Moreover, the pre-operative education has significant effects for the stoma patients’ rehabilitation. Concerning the educational strategies, the respondents mentioned that both individual education and group counseling have their strengths and weaknesses in order to make psychological support, family and friends’ support has been mentioned as the most significant part that can release stoma patients’ anxiety, followed by support from other stoma patients. In relation to correlates with body image, the present study revealed that there are a positive correlation were found between characteristics of the stoma and the typical body image score between post and follow-up implementation of educational in items related to types, nature, and numbers of stoma. these findings goes in distinguish with Ciorogar et al, 2016 in California (USA) who concluded that Ostomy still has a largely negative impact on patients’ quality of life as their mindset is the main issue. The idea of having to live with a stoma bag remains a significant problem for this group of patients. While, Benedict et al, 2016 mentioned that Long-term bowel and GI dysfunction are upsetting and affect how women recognize and relate to their bodies, exacerbating survivorship difficulties. Interventions to improve adaptation post-treatment should concentrate on treatment side effects, target body image problems to ease depressive symptoms, and reducing anxiety which may require other program strategies. Thus, body image may be considered as a key modifiable factor to progress well-being in this understudied population.Therefore, Chennai people who have had stoma surgery are not only contended with immediate physical changes that the surgery brings out but also familiar to the psychological impact of stoma configuration, also complete understanding of having a gastrointestinal illness resulting in stoma surgery represents a major change in patient’s life. Nevertheless, Patients have to cope with difficult emotional feeling, social and physical problems associated with newly created stoma. Due to these progression life occurrences, patients can become very anxious and depressed plus get worse of their life quality. [33]Based on Radcliffe [17] from England the significance of appraisals appears supported by the qualitative data suggesting that body image disturbances are due to changes in perceptions of the body compared to their own internal concept of the ideal self-image. Stoma patients without helpful managing around them receive less external support for adjusting internal images of “normal” and concerns about other appraisals of their stoma and demanding to cover up their stoma bags which may affect patient's adjustments. In Turkey, Aktas and Baykara [14] painted on stoma patients who consulted their partners’ opinions on stoma establishment and participation in care had significantly higher BCS scores (P <0.05), and BCS scores of patients whose partners thought the stoma had a negative effect on their relationship were significantly lower (P = 0.040); patients’ perceptions toward their bodies were equivalent to their partners’. Mean BCS score of patients experiencing physical and psychosocial problems was significantly lower than those of patients who did not experience such problems. Also, a number of factors concerning patient partners before surgery which has benefits in change patient's perception of their body following stoma surgery.
5. Conclusions & Recommendations
- From the foregoing discussion, it can be seen that the implementation of multimedia educational programme for colostomized patients showed a remarkable increase and improvement of the patient 's level of knowledge and acquiring the ultimate positive and noticeable improvement in the patient's corrective actions towards colostomy care, prevention of complications which has direct effect on their quality of life and body image, also, there are evident needs for instructional scheme or guidelines offered on simple media to those patients to minimize complications postoperatively and improved patient's coping and adherence with their cancer treatment modalities and colostomy care. Efforts should be carried out to design and implement interventions that suit oncology centers and institutes with field evidence and increased facilities, patient's education approaches, and documentations of noncompliance cancer patients within disease, treatment modalities and follow-up appointments.