-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2018; 8(5): 93-97
doi:10.5923/j.nursing.20180805.03

A Tool for Evaluation of Nurses Handover: Validity and Reliability Study of the Handover Evaluation Scale
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAyşe Demiray, Ayla Keçeci, Ayşegül Açıl, Nagihan İlaslan
Düzce University Faculty of Health Sciences, Nursing Department, Düzce, Turkey
Correspondence to: Ayşegül Açıl, Nagihan İlaslan, Düzce University Faculty of Health Sciences, Nursing Department, Düzce, Turkey.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Nursing handover is the process of transferring patient care from one caregiver to another, such that this care is safe and of a high quality. A limited number of studies have assessed how this can be successfully accomplished. However, it has been stated that there are an insufficient number of tools available to evaluate the efficiency of the process and the arrangements for structuring the handover period. This study aimed to carry out Turkish validation of the ‘Handover Evaluation Scale’, developed by O'Connell, Ockerby and Hawkins. The validation of the Handover Evaluation Scale, was conducted with nurses. The size of the sample was targeted as five times the number of questions on the original scale, and 136 nurses participated. Explanatory factor and confirmatory factor analysis were used as validity methods, and test-retest, test-split techniques were used for the reliability studies. The original scale includes 17 items, six items were removed in study. The scale obtained as a result of the present study has a one-factor structure. This study provides Handover Evaluation Scale, which is a valid and reliable tool for evaluating nursing handovers in Turkey. Successful patient handover is indispensable to reduce mistakes caused by handover, providing patient safety and increasing the quality of healthcare. This evaluation of the effectiveness of the handover processes was carried out in a clinical environment in Turkey, and studies (training, counselling, etc.) to improve the delivery process can be performed using this tool, which has Turkish validity and reliability.
Keywords: Nurse, Patient, Patient delivery, Handover evaluation scale
Cite this paper: Ayşe Demiray, Ayla Keçeci, Ayşegül Açıl, Nagihan İlaslan, A Tool for Evaluation of Nurses Handover: Validity and Reliability Study of the Handover Evaluation Scale, International Journal of Nursing Science, Vol. 8 No. 5, 2018, pp. 93-97. doi: 10.5923/j.nursing.20180805.03.
Article Outline
1. Introduction
- In order to ensure safety and quality, nursing handover is of great importance in transferring patient care from one nurse to another [1]. Patient handover includes verbal, written, and voice recordings in terms of communication, which is performed in three shifts at the nursing room and at the nurse's desk in the morning [1-5]. The aim of patient handover, an indispensable element of patient care, is to share short and up-to-date information regarding the patient's life, as well as to increase the accuracy/validity of clinical information, in order to avoid repeated applications, ensure the applicability of information submitted on handover and provide holistic care [1-6]. Patient handover often includes provision of the patient's name, age, gender, life history, and other pertinent events in the patient’s life, in a particular manner. However, the time allocated to nursing care plans at the time of handover of a patient does not exceed 1% of the total duration, and therefore no necessary updates can be made to patient care plans, as a result of the limited information delivered. Moreover, patient handover is often interpreted as a waste of time by nurses [4]. Nevertheless, it is also known that ensuring patient safety and increasing the quality of care are indispensable for successful patient handover.A limited number of previous studies have assessed how to perform a successful handover [1, 4, 7]. Furthermore, there are no standards/procedures in Turkey, with regard to implementing an effective nursing handover. According to the Regulation on the Amendment of the Nursing Regulation, published by the Ministry of Health on 19 April 2011, nurses must submit nursing records related to care and treatment applications / observations to the departmental nurses / associates in written and verbal exchanges during shifts. Unfortunately, there is no standard as to how this process should be carried out, although there is a nursing handover structure at the national level.A handover with the participation of health professionals with different areas of expertise and different levels of education means that both patients and nurses face more complex handover processes. Ineffective patient handovers may lead to disruptions in care, mistakes in drug dosing, surgeries on the wrong side of the body and patient deaths [8]. On the basis of this information, the present study was designed to provide a scale for use in assessing the suitability of nursing handover in a university hospital in Turkey.
2. Methods
2.1. Aim
- The aim of was to conduct Turkish validity-reliability studies of the Handover Evaluation Scale developed by O'Connell, Ockerby and Hawkins.
2.2. Sample and Population
- The nurses of a university hospital participated in this study, for which the permission of the ethics committee was granted. In the scale studies, the aim was to reach a total of 85 nurses, corresponding to five times the 17 items in the Handover Evaluation Scale, considering that at least three or 5–10 people should be considered for each scale item. The total number of the participants in the sample was 136.
2.3. Data Collection Tools
- A questionnaire developed by researchers and the Handover Evaluation Scale were used to determine demographic characteristics.
2.4. Handover Evaluation Scale
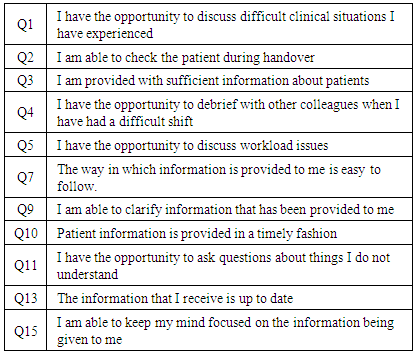
- The Handover Evaluation Scale is a measure of a total of 17 items, with three questions being optional, and exploratory and confirmatory factor analyses were performed. The scale was initially composed of 20 questions, and when the factor analysis was performed, it was determined that the questions should be aggregated in five dimensions. The scale was subsequently reduced to four factors and 18 items because only one item was included in one dimension, and the explanatory power was low. In accordance with the DFA results, another item was removed, and there were ultimately 17 items in the scale, which consisted of four factors: knowledge quality, interaction and support, efficacy and patient participation. Correlations of the four dimensions were evaluated, and strong correlations between the first three of were observed. Therefore, it was decided that the scale consisted of three basic dimensions; however, the items regarding patient participation remained in the scale as optional items.
2.5. Data Collection
- The nurses participating in the study were provided with the necessary information regarding the purpose of the research, as well as with data collection forms. During data collection, the researchers accompanied the nurses and allowed them to ask questions. The nurses completed the data collection forms in approximately 15–20 minutes.
2.6. Procedure
- Beverly O'Connell was asked for permission to adapt the Handover Evaluation Scale, via e-mail. In order to prevent any problems that may have arisen due to cultural differences, English–Turkish and Turkish-English translations were performed, and the consistency was evaluated in terms of meaning and grammar. Following translation, the scale was sent to seven specialists who were asked to make an assessment in terms of content validity. The scores given by the experts varied between 1 and 4, and, according to expert opinion of the scale, the content validity index was designated as .92. After obtaining the expert opinions, descriptive factor analysis and confirmatory factor analysis were carried out.
3. Results
3.1. Socio-Demographic Characteristics
- A total of 55.1% (n=75) of the nurses were aged 30–39 years; 80.9% (n=10) were females, 64.7% (n=88) were undergraduates, 78.7% (n=107) were staff nurses, 33.1% (n=45) had 1–5 years of experience, 62.5% (n=85) had received handover training and 58.8% (n=80) were satisfied with the level of handover.
3.2. Validity
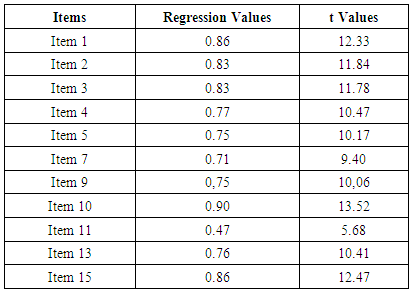
- In order to determine the reliability of the Handover Evaluation Scale, t-test and test split techniques were used, while explanatory factors analysis (EFA) and confirmatory factor analysis (CFA) were used to determine the construct validity of the scale.Explanatory Factor Analysis An EFA technique was used to statistically determine the construct validity of the scale. The Kaiser-Meyer-Olkin (KMO) and Bartlett tests were performed, primarily to determine whether the scale was appropriate for factor analysis. In this context, the results of the KMO test should be .50 and above, and the Bartlett test for sphericity result should be statistically significant [9]; the KMO test result was .90 and the Bartlett sphericity test result was significant (p <0.01). Accordingly, there was a high correlation between variables, in other words, the data set was suitable for factor analysis. The first analysis showed that three factors were higher than the eigenvalue of 1. However, when Figure 1 is observed, it can be understood that the factor with the highest eigenvalue and with the higher explained variance was predominant.
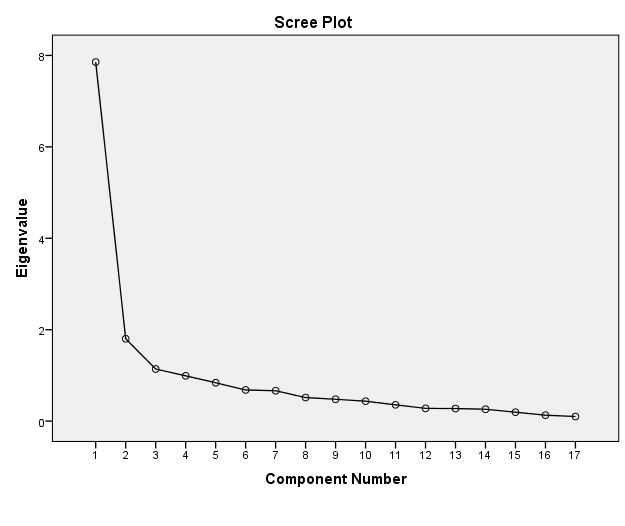 | Figure 1. A scatter diagram of the eigenvalues of the factors |
|
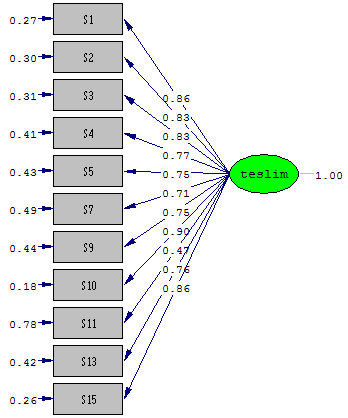 | Figure 2. A Scale Path Diagram |
|
|
3.3. Reliability
- In the reliability study, the Cronbach’s alpha coefficient of the scale increased to .94, with the removal of certain items in the Turkish version. The scale was also analysed using the test splitting technique; a minimum of 100 and a maximum of 400 participants are recommended for Spearman-Brown and Guttman analysis methods [11]. The size of the study sample met the pre-condition for these analysis methods, with the Spearman-Brown coefficient being r = 90, and the Guttman coefficient being r = 88.A paired t-test was carried out approximately 30 days later, in order to assess the time-invariance of the Handover Evaluation Scale. When the pre-test and post-test results were examined, no significant difference between the results was observed, which demonstrates the reliability of the respondents (Table 5).
|

|

4. Discussion
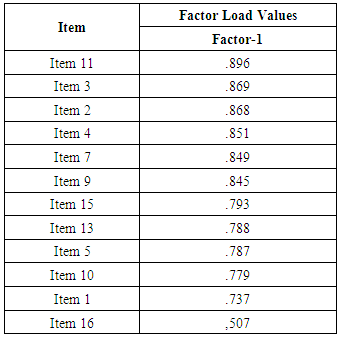
- This study aimed to adapt the Handover Evaluation Scale developed by O'Connell, Ockerby and Hawkins to Turkish. The EFA and CFA validity results showed that the scale consists of 11 factors in a one-factor structure, and it is considered that the scale is of a sufficiently strong structure to enable evaluation of the handovers. First, EFA was applied to the scale and three factors greater than an eigenvalue of 1 were found. However, it was understood that one factor that had a higher eigenvalue and a higher explained variance than the other factors was dominant.After the number of factors was determined, another factor analysis was conducted and two items in both the patient participation and efficiency dimensions, as well as one item in the quality of knowledge dimension, were removed because these three items were below the factor load value of .30. During the study period, the nurses verbally stated that the items regarding the dimension of patient participation were not relevant to them, and that they did not include patients in the handovers. In this scale, the items in this dimension are optional, and it is believed that in analysing the scale in other cultures, the analysis should be performed by taking preliminary information about patient participation before including it in the analysis process. O'Connell, Ockerby and Hawkins also considered the items in this dimension as problematic for their own sample, and used the items in this dimension as optional. However, the item ‘I am able to check the patient during handover’ has a high factor load and is included in the scale in this study. This can be attributed to the fact that nurses maintain their observations of the patients until the end of handovers [12].In the CFA analysis, a further item that was included in the interaction and support dimension of the scale, and which had an insignificant t value, was removed, thus achieving the final form of the scale. As a result, a total of six items, two in the patient participation dimension, two in the efficiency dimension, one in the interaction-support dimension and one in the quality of knowledge dimension, were removed from the scale. There were no inverse coded items. The increase in scores indicates that the assessments were positive.
5. Conclusions
- Patient handover, an indispensable part of patient care, is an important nursing function that must be effectively carried out in order to provide holistic care [1, 6]. In our country, although there are some regulations regarding the administration of hospital services in the framework of the Ministry of Health's quality applications, there are no arrangements for patient handover from one nurse to another [13]. It is thought that this condition has created/will create a lack of effectiveness and quality in patient handover. However, irrespective of whether patient standards are being developed for nurses, the lack of an evaluation tool for the effective administration of the procedure is also a major drawback. Therefore, it is believed that the Turkish adaptation of the Handover Evaluation Scale will fill a significant gap.
ACKNOWLEDGEMENTS
- We sincerely express our appreciation to the participants who generously provided their time and invaluable contribution.