-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2018; 8(4): 67-72
doi:10.5923/j.nursing.20180804.02

Knowledge Level and Utilization of Prevention of Mother to Child Transmission Services in Enugu, South East Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAda Nwaneri1, Adaeze Mbagwu2, Omolara Adeyemo3, Ifeoma Ndubuisi1
1Department of Nursing Sciences, University of Nigeria, Enugu Campus, Nigeria
2Nursing Services Department, ESUT Teaching Hospital, Enugu, Nigeria
3Department of Nursing Sciences, Osun State University, Osogbo, Nigeria
Correspondence to: Ada Nwaneri, Department of Nursing Sciences, University of Nigeria, Enugu Campus, Nigeria.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Mother to child transmission continues to be the major source of HIV infection among children below the age of 15 years. Objective: To determine the knowledge level of prevention of mother to child transmission services (PMTCT) and utilization of PMTCT services among HIV positive pregnant women attending antenatal clinic in two Teaching Hospitals in Enugu State. Method descriptive cross-sectional study: A researcher developed validated questionnaire was administered to 148 consenting HIV positive pregnant women who enrolled for PMTCT services in two federal tertiary institutions in Enugu. Data were analysed using descriptive and inferential statistics of Chi-square at five percent level of significance. Result: Almost all 129 (94.9%) the respondents have heard of PMTCT. Their source of information was mainly through health workers (90.7%). The respondents knew that HIV can be transmitted from mother to baby during pregnancy (85.3%), childbirth (83.7%) and breastfeeding (72.1%). Their knowledge of PMTCT services like HIV testing (80.6%) and antiretroviral drugs (93.8%) was very high while that of HIV counselling (58.9) was slightly above average. Majority 82.2% of the respondents stated that what PMTCT services entails was exclusive breastfeeding for 6months and infant testing after delivery while 80.6% feels that the services entails delivery by skilled personnel. Generally, the respondents’ level of knowledge on PMTCT revealed that 73 (53.7%) had moderate knowledge, 52(38.2%) had good knowledge while only 4(2.9%) had poor knowledge of PMTCT. Majority 127(93.4%) of the respondents utilized the services. There was a significant association between level of knowledge and utilization of PMTCT services (p<.001). HIV positive mothers have moderate knowledge of PMTCT services and majority of them utilise the services. Conclusion: The respondents have moderate knowledge of PMTCT and also utilise the service.
Keywords: PMTCT services, Utilization of PMTCT services, Constraining factor, Level of knowledge
Cite this paper: Ada Nwaneri, Adaeze Mbagwu, Omolara Adeyemo, Ifeoma Ndubuisi, Knowledge Level and Utilization of Prevention of Mother to Child Transmission Services in Enugu, South East Nigeria, International Journal of Nursing Science, Vol. 8 No. 4, 2018, pp. 67-72. doi: 10.5923/j.nursing.20180804.02.
Article Outline
1. Introduction
- Mother to child transmission continues to be the major source of HIV infection among children below the age of 15 years [1]. It increases the prevalence of HIV in infants and maternal morbidity and mortality. In 2009, it was estimated that there were 370,000 new paediatrics HIV infections with Sub-Saharan Africa accounting for about 90% [2]. At the end of 2011, Nigeria had about 470,000 HIV patients on ART with 36,716 children and 26,336 pregnant women [3] Twenty two percent (51,000) of all new child HIV infections globally in 2013 were in Nigeria with only 29% decline in child HIV infection since 2009 [4].The emergence of human immunodeficiency virus in 1980s has increased the existing heavy burden of disease and death among women and children [5]. The infant of a human immunodeficiency virus infected mother acquires the human immunodeficiency virus infection from the mother at one or more of the following stages: transplacental in the uterus during pregnancy, perinatal during the process of labour/delivery and postnatal after delivery [6]. UNAIDS, 2014 stated that mother to child transmission accounts for over 90% of new human immunodeficiency virus infection among children [7]. Since nearly all HIV infection in children (90%) is acquired through vertical transmission, the global epidemiology of HIV infection in children also reflects the prevalence of HIV in mothers. As more women get infected with HIV, so is the number of children [3].Human immunodeficiency virus infection in women of reproductive age increases the epidemic of mother to child transmission. Globally 17million women in their reproductive age (15years and above) live with human immunodeficiency virus while 1.5 million pregnant women and about 2.6 million children less than 15years are estimated to live with the virus. About 220,000 children are estimated to be newly infected with human immunodeficiency virus daily [7]. Out of this number, 150,000 cases occur through human immunodeficiency virus positive mothers transferring the infection to their children during pregnancy, childbirth and breastfeeding [8].Recognizing the need for saving many children from human immunodeficiency virus menace, the member States of the United Nations (UN) in 2001 introduced prevention of mother to child transmission [9]. Prevention of mother to child transmission is an intervention to ensure that no child is born with HIV and it is an essential step to ensuring an AIDS free generation [9]. Annually, specific goals are set to reduce the proportion of infants infected with human immunodeficiency virus. For instance, 20% reduction goal was set in 2005 and 50% by 2010 [7]. A scale up plan to raise these goals to 90% by 2015 was launched by a global plan target in 2011 to reduce the number of new human immunodeficiency virus infection through mother to child transmission [8].In addition to setting the goal of prevention of mother to child transmission by USAIDS, other International Organizations such as the World Health Organization (WHO) promote a comprehensive approach to prevention of mother to child transmission programme which includes preventing new human immunodeficiency virus infections among women of childbearing age, preventing human immunodeficiency virus transmission from a woman living with human immunodeficiency virus to her baby and providing appropriate treatments, care and support to mothers living with human immunodeficiency virus and their children [10]. Despite these comprehensive approaches and interventions to prevention of mother to child transmission, there are still some constraining factors to its utilization identified in various studies. These factors are demographic, systemic, socioeconomic, cultural, religious and knowledge. Knowledge is of paramount importance as low uptake of PMTCT services can be as a result of inadequate knowledge about the programme. The information the pregnant women receive about PMTCT services play an important role in access and utilization of PMTCT services. However, a report showed that women with no education have less knowledge about MTCT compared to those with secondary education [11]. A study conducted in Sudan sampled 53 pregnant women showed that 96% of the respondents did not know HIV infection can be transmitted from mother to child [12].Despite these interventions, approaches and global plan targeted at reducing mother to child transmission by 90% and reducing the number of new infections among women of reproductive age by 50% among 21 global plan target countries Nigeria inclusive, significant success is yet to be recorded in Nigeria. For instance, in the 2011 goal of 90% reduction in MTCT, Nigeria registered about 36% reduction in the number of new HIV among women of reproductive age and 21% reduction in mother to child transmission [9]. Nigeria was considered to be the second worst performing global plan priority country after Chad [13], whereas six priority countries which include Botswana, Mozambique, Namibia, South Africa, Swaziland and Uganda met the global plan target. Uganda recorded 86% reduction, South Africa recorded 84% reduction while Botswana, Namibia and Swaziland had fewer than 1000 new infections in 2015 [8].This can be considered an indication of very poor utilization of prevention of mother to child transmission services. This implies that, if nothing is done to improve the level of utilization of the PMTCT programmes, present and future national or international prevention programmes will not be effective in saving Nigerian born and unborn children from the increase in HIV infections due to MTCT. Identifying the key and specific factors that negatively impact the utilization of PMTCT programmes is important to prioritize strategies aimed at enhancing participation in PMTCT programme. Hence, it has become necessary through this study to find out the level of knowledge and utilisation of prevention of mother to child transmission (PMTCT) services in two Teaching Hospitals in Enugu State.
2. Methods
- Cross sectional descriptive survey design was utilized in conducting this study. The participants of study were 148 HIV positive pregnant women that enrolled for PMTCT services between January and July, 2017. The entire population was used based on the small population size.Instrument for data collection was a pre-tested researchers’ developed questionnaire. It contained twenty two items on respondent’s knowledge of PMTCT services. The responses were scored and interpreted, such that those that scored 50% and above have good knowledge while those that scored less than 50% have poor knowledge. Ethical approval and administrative permit were obtained from the two Teaching Hospitals. Verbal informed consent was obtained before administering the questionnaire to each HIV positive pregnant woman that met the inclusion criteria (i.e. enrolment in PMTCT within the period of the study) in the two Teaching Hospitals. The responses to each question were analyzed using both descriptive and inferential statistics and presented in tables. The descriptive statistics- frequency, percentage, mean and standard deviation were used to summarize the items of the questionnaire. A mean cut-off point of 2.5 was used to make decisions and conclusions, which was obtained by taking the mean of the response scores. The Chi-Square Test was the inferential statistics used to test the hypothesis, statistical conclusions were made at 5% level of significance. These statistics were done with the aid of SPSS/IBM statistical software (version 20).
3. Results
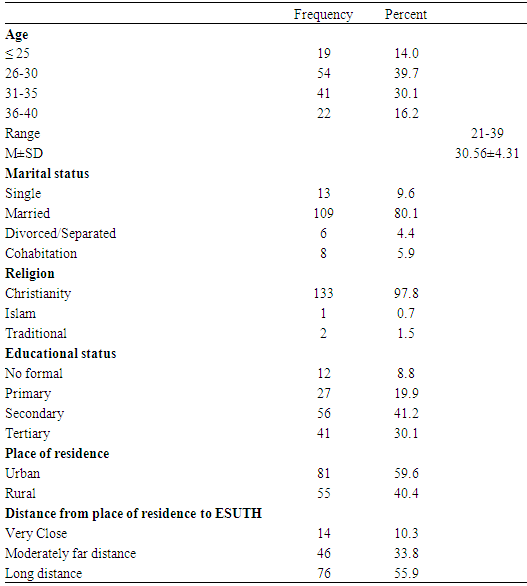
3.1. Demographic Characteristics of the Respondent
- The age of the women ranged from 21-39 years with a mean age of 30.56. Of all the respondents, 109 (80.1%) were married, majority {133 (97.8)} were Christians. Many [56 (41.2%)} of the respondents had secondary education while most {81 (59.6%)} were urban dwellers. Only 10.3% of the women lived very close to the hospital, 33.8% lived moderately far away while 55.9% lived a long distance away from the hospital. (see table 1)
|
|
 n = 136
n = 136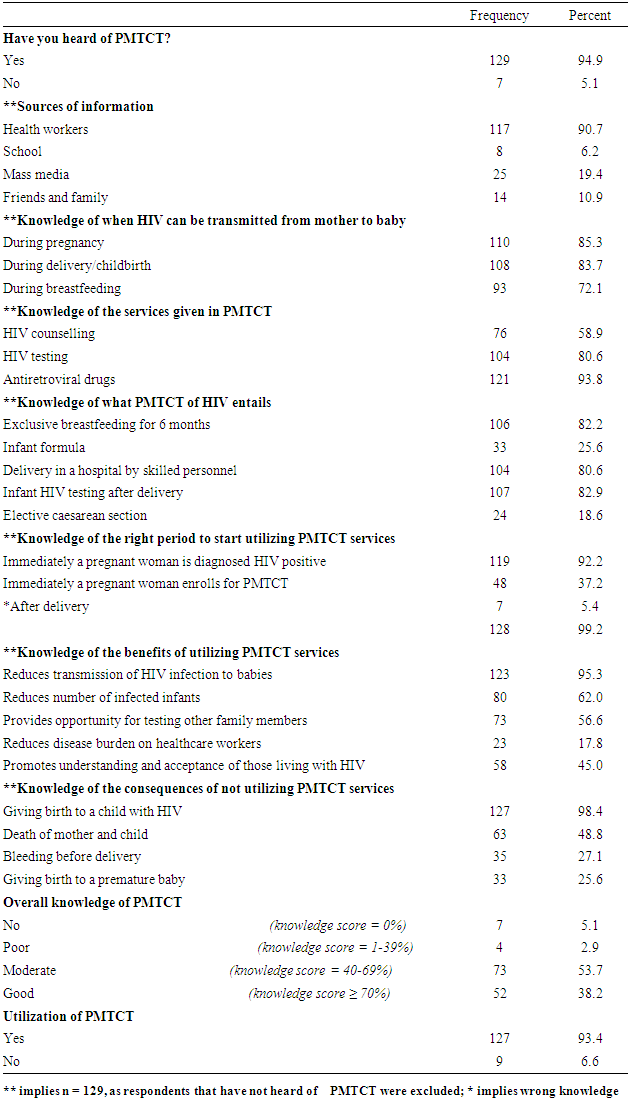
|
 n = 136
n = 136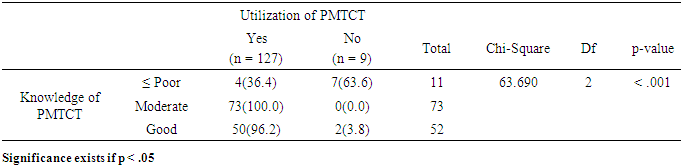
4. Discussion
- The findings in this study revealed that almost all the women have heard of PMTCT services and majority of the respondents got their information through health workers. This result shows that the awareness creation through the media regarding HIV/AIDS in general and PMTCT has yielded result among pregnant women. This also shows that the health talk given during ante natal clinic is effective considering the fact that majority of the respondents’ knowledge is from the health workers. Efforts should be geared towards ensuring that information disseminated during antenatal care are correct and emphasis should be on making it more practical. In addition, health talk and information dissemination is also done in HIV clinics to ensure that correct information is communicated to the clients and misconceptions corrected during the question and answer sessions. This must have accounted for their good knowledge about the PMTCT programme and what it entails. HIV testing and antiretroviral drugs were majorly identified by the respondents as the services provided in PMTCT programme. This result may be so because the service that those who are HIV positive and negative utilise often is the testing programme. This is usually done to confirm their status and once they are confirmed positive, they start accessing antiretroviral drugs. It is worthy to note that only few of respondents regarded counselling as part of the PMTCT programme. Counselling is a major programme in PMTCT and the users of the programme should understand that and pay attention during counselling sessions. Counselling in PMTCT is very important as it is during the session that the client understands what to do, and how to do it in order to ensure that there is no transmission of HIV from mother to child. The women’s knowledge of what PMTCT service entails was majorly on exclusive breast feeding for 6 months, delivery by skilled personnel and infant testing after delivery. This might have led to the overall outcome of most of the participants having moderate knowledge about PMTCT. In this study, the findings imply that knowledge is not a barrier as many of the respondents have moderate knowledge and 38.2% have good knowledge of PMTCT services. This is in line with the findings of a study done in Nigeria by Pclue (2011) which showed that majority of the respondents (60%) have good knowledge about PMTCT services [14]. The finding however contradicts the views of previous researchers [15], which revealed poor knowledge of MTCT and comparative low awareness of MTCT and its prevention. There is a significant association between knowledge of PMTCT services and utilization of PMTCT services (p<.001). This result suggests that utilization of PMTCT services is dependent on the women’s knowledge of PMTCT services. Non-utilization was associated more to women with poor and lesser knowledge of PMTCT than those with moderate (0.0%) and good knowledge. This might be the fact that the client attitude towards PMTCT services depends on the information and knowledge gathered from health workers, friends and anyone who gives first hand information. If pregnant women get proper and adequate information, they will utilize PMTCT services willingly. Hence, lack of knowledge may be a constraining factor to utilisation of PMTCT services.
5. Conclusions and Recommendations
- In conclusion almost all the women have heard of PMTCT of which their source of information was mainly through health workers. The knowledge that PMTCT services include HIV testing and antiretroviral drugs was very high while that of HIV counselling was slightly above average. Majority of the respondents had moderate knowledge of PMTCT. There was a significant association between knowledge and utilization of PMTCT services (p<.001). Though knowledge was not identified as a constraint in this study, health care providers should intensify efforts to disseminate effective education on PMTCT to individuals, families and communities. It is recommended that knowledge dissemination through other avenues should be encouraged to enhance wider coverage.
Limitations of the Study
- There was difficulty in data collection because of the sensitivity nature of the participants. As all administrative protocols have to be followed before having access to necessary data for successful conduct of the study.