Nimnual Chuyingsakultip1, Pennapha Koolnaphadol2, Pracha Inang2
1M.N.S., APN Adult Nursing, Ph.D. Student Counseling Psychology, Burapha University, Thailand
2Ph.D. Professor of Counseling Psychology, Burapha University, Thailand
Correspondence to: Nimnual Chuyingsakultip, M.N.S., APN Adult Nursing, Ph.D. Student Counseling Psychology, Burapha University, Thailand.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The purposes of this research were to study and develop family burden management and family happiness of stroke patient through assimilative integrated family counseling. The participants were stroke patients and their couple, who were treated in hospitals in the Sixth National Health Service of Thailand. There were two steps in this research. The first step aimed to developed research instrumentals for measured the family burden management, by using 776 participants from 388 families for study the components of family burden management and to study influence of family burden management to family happiness on stroke patients. The second step aimed to study effectiveness of the assimilative integrated family counseling program on family burden management and family happiness of stroke patients. The participants using 40 persons from 20 families, consisted of patients and their couple at Rayong Hospital. The participants in the second step were selected from 83 families who had the means score of family burden management at lowest sort for 20 families and had completed inclusion criteria. Matching group was done for prevention bias and then simple random sampling for control and experimental group. The experimental group received the intervention based on assimilative integrated family counseling program (12 sections, 60-90 minutes in each section). The research instrumentals were the questionnaire for measured family burden management, family happiness and the assimilative integrated family counseling program for enhancement family burden management and family happiness. Data were analyzed by LISREL program for confirmatory factor analysis, descriptive statistics and MANOVA. The results of this study were as follows: 1. The secondary confirmatory factor analysis showed that the family burden management of stroke patients in Thailand context consisted of four components 1) family strain management, 2) family conflict management, 3) family guilt management and 4) family attitude. The four components had a moderate to high factor loading score at .05 level, and its could be able to measure the family burden management of stroke patients. 2. The influence of family burden management to family happiness on stroke patients could predicted family happiness about 71 percentages with coefficient of influence was .89. The mean score of the family burden management in 388 stroke patients was 2.77, and their couple was 2.76 which considered in the moderate level. The mean score of family happiness in the 388 stroke patients was 3.00, and their couple was 3.04 which considered in the regular level. 3. The assimilative integrated family counseling program was effectiveness that the mean score of family burden management and family happiness of stroke patients at the end of program (after sections), and the follow up phases were higher than before start the program with statistically significance at .05 level. 4. The experimental group had the mean score of family burden management and family happiness higher level than the control group with statistically significance at .05 level.
Keywords:
Family burden management, Family happiness, Assimilative integrated family counseling
Cite this paper: Nimnual Chuyingsakultip, Pennapha Koolnaphadol, Pracha Inang, The Enhancement of Family Burden Management and Family Happiness of Stroke Patient through Integrative Family Counseling, International Journal of Nursing Science, Vol. 7 No. 6, 2017, pp. 115-122. doi: 10.5923/j.nursing.20170706.01.
1. Introduction
Family are important institutions to start cultivating ideas, beliefs, values, and attitudes towards the members. Family members are different roles and responsibilities. Incidence risk made family members changes in their roles and responsibilities. This is the cause of the problems members may feel more burdensome responsibilities especially when a member of the family is sick. In particular, illness with chronic disease, the family will affected by the impact on the system of work in the body and mind including roles in the family. Stroke is the disease that is a major public health problem. World Stroke Organization: WSO report in 2017 found that stroke accounted for 6.5 million deaths worldwide, and was the second leading cause of death in the population over the age of 60 and the fifth leading cause of death in the population aged 15 – 59 years (WSO, 2017). In Thailand, the death rate per 100,000 population is likely to increase by 330.60, 354.54 and 366.81 in 2011-2013 (The Office of Ministry of Public Health, 2014), and the remaining 60 percentage of patients have moderate to severe disabilities that affect family happiness. Family counseling is a psychological process that helps to developed the relationship of family member from one step to the next step, appropriately according to the developmental stage of the family. Helping family members to think and decided to solve problems with their family. The assimilative integrated family counseling program developed by using the conceptual model of Transgenerational theory for the main theory which emphasizes the family system. The assimilative integrated family counseling will result in family adaptability and live happily in society, good quality of life, reduce problems in families, communities, society, and the national.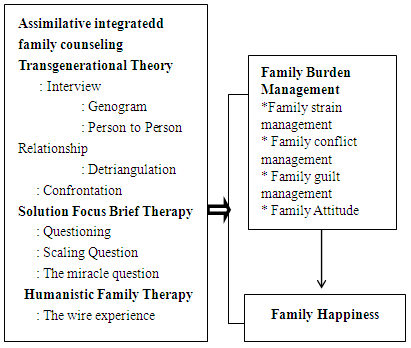 | Figure 1. The conceptaul framework |
Research purposes1. To study the components of family burden management of stroke patients.2. To study the influence of family burden management to family happiness in stroke patients.3. To enhancement family burden management and family happiness in stroke patients.Hypotheses1. The composition of family burden management consists of four components: family strain management, family conflict management, family conflict management and family attitudes.2. Family burden management influences to family happiness of stroke patients.3. The experimental group had higher mean score of family burden management and family happiness at the end of program (after sections), and the follow up phases.4. The experimental group had higher mean score of family burden management and family happiness than the control group at the end of program (after sections), and the follow up phases.
2. Methods
In this research was conducted in 2 steps.Step 1-1: Confirmatory Factor Analysis: CFAResearcher studied theoretical concepts from both domestic and international research to obtain the composition of the family burden management by using the conceptual framwork of family burden of Steven H. Zarit and Judy M. Zarit (Zarit & Zarit, 1986, 1990) Evaluate the family burden management as 4 components in Thailand context: family strain management, family conflict management, family guilt management and family attitudes. The family burden management instrumental survey form was created by the researcher to measure the family burden management in the four components, researcher examined the validity of the questionnaire with 32 completed questionnaires. Five experts were invited to comment on the consistency of the questionnaires and the researcher improved the questionnaire as the experts provided feedback and the IOC was .84. Researcher tryout with 30 stroke families at Rayong hospital, Rayong province, Thailand. The reliability of the family burden management by cronbach's coefficient (α-Coefficient) was .95 and the family happiness was 0.94. In the survey researcher used a completed family burden management and family happiness measurement for collected data. The sample, consisting of 776 members from stratified random sampling in the Sixth National Health Service of Thailand.Step 1-2: Researcher using the Path analysis for study family burden management influence to family happiness of stroke patients by using Structural Equation Model: SEM by LISREL.Step 2: Assimilative integrated family counseling program development.The researcher studied journal and research related to family counseling. Conduct an integrated family counseling model, theory and technique. The care model designed to enhancement on family burden management that involves four components: family strain management, family conflict management, family guilt management and family attitude. Twelve sections of assimilative integrated family counseling were conducted about 60-90 minutes per section.Advocacy groupsReceived approval from the Ethics Committee in humans at Burapha University in May, 2017.Received approval from the Ethics Committee in humans at Rayong Hospital in July, 2017.
3. Result
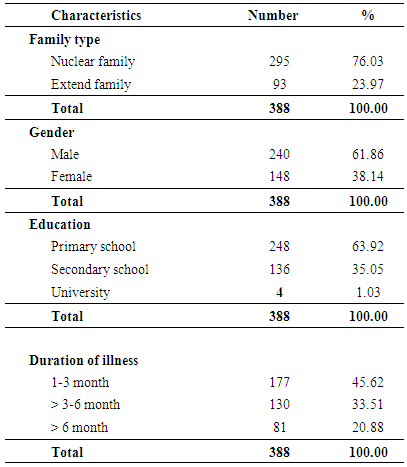
Table 1. Description of demographic of stroke patients
 |
| |
|
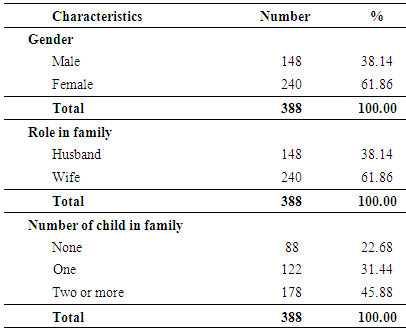
From Table 1 could explained Family characteristics of stroke patients the most were nuclear family about 76.03%, the most were males about 61.86%. There education the most were primary school about 63.92% and had duration of illness were 1-3 months about 45.62%.Table 2. Description of demographic of couple of stroke patients
 |
| |
|
From Table 2 could explained family characteristics of couple of stroke patients the most were female about 60.82% these were wife role in family and there were children two or more about 45.88%.1. Factor analysis of family burden management in Thailand contextThe Adjust Model was fit with empirical data at an acceptable level: Chi-Square = 411.28, df = 214, p-value = .000; Chi-Square / df = 1.92; RMSEA = .047; RMR = .042; SRMR =.041; CFI= .98; GFI = .92; AGFI = .91; CN = 205.86. The family burden in Thailand context consists of 4 elements (1) family strain management the Standardized Solution was .96 that statistically significant at .05 (t = 20.57) R2= 0.92 (2) family conflict management the Standardized Solution was .95 that statistically significant at .05 (t = 26.67) R2= 0.90 (3) family guilt management the Standardized Solution was .96 that statistically significant at .05 (t = 23.12) R2= 0.60 (4) family attitudes the Standardized Solution was .96 that statistically significant at .05 (t = 8.60) R2 = 0.23.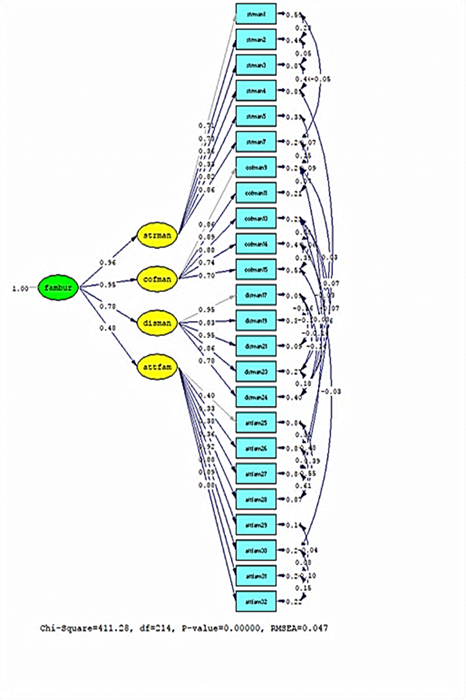 | Figure 2. The Adjust Model of family burden management in the Sixth National Health Service of Thailand (n = 776) |
2. Path analysis of family burden management to family happiness of stroke patients by using Structural Equation Model: SEM by LISRELThe Adjust Model was fit with empirical data at an acceptable level: Chi-Square = 5.63, df = 3, p-value = .131, Chi-Square / df = 1.87; RMSEA = .034; RMR = .0028; SRMR = .0079; CFI= 1.00; GFI = 1.00; AGFI = .99; CN = 1516.16.The family burden influence to family happiness on stroke patients with coefficient of influence was .89 and could predict family happiness about 71 percentages.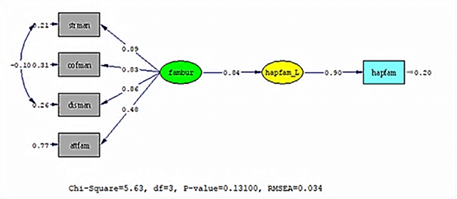 | Figure 3. The Adjust models family burden management affects family happiness in the Sixth National Health Service of Thailand (n = 776) |
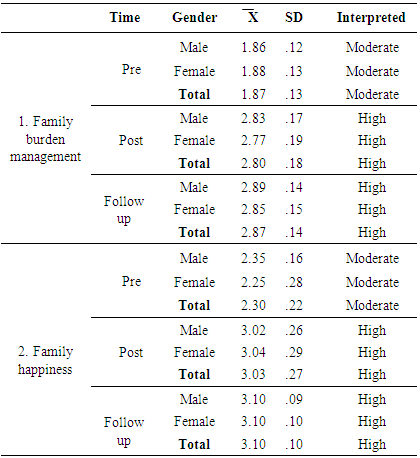
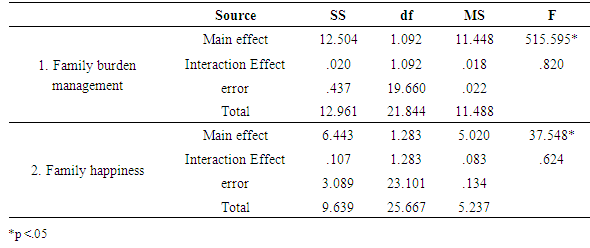
3. Outcome of assimilative integrated family counseling program for enhancement family burden management and family happiness of stroke patientResearcher using factorial experiment or complex designs and had a control group and measured family burden management and family happiness in 3 phased: pre sections measured family burden management and family happiness before start assimilative integrated family counseling program. In the end of program (post sections) measured family burden management and family happiness after completed 12 sections and in the follow up phase measured family burden management and family happiness in 4 weeks after the post sections. The statistics used MANOVA repeated measurement.From Table 3 - Table 5 could explained 1. Family burden management no Interaction effect with time and gender (F = 018, p > .05) but had the main effect in time at pre sections, post sections and follow up sections (F = 515.595*, p < .05) so researcher run post hoc test and found that family burden management at post sections was higher than at pre sections and family burden management at follow up sections was higher than at pre sections and post sections that statistically significance at .05 level. 2. Family happiness no Interaction effect with time and gender (F = .624, p > .05) but had the main effect in time of pre sectionn, post sectionn and follow up sectionn (F = 37.548* p < .05) so researcher run post hoc test and found that family happiness at post sections was higher than at pre sections and family happiness at follow up sections was higher than at pre sections and at post sections that statistically significance at .05 level.Table 3. Description of Mean and Standard Deviation of family burden management and family happiness in experimental group
 |
| |
|
Table 4. Family burden management and family happiness of experimental group (Two-Way MANOVA Repeated Measurement)
 |
| |
|
Table 5. Post hoc test of family burden management and family happiness of experimental group
 |
| |
|
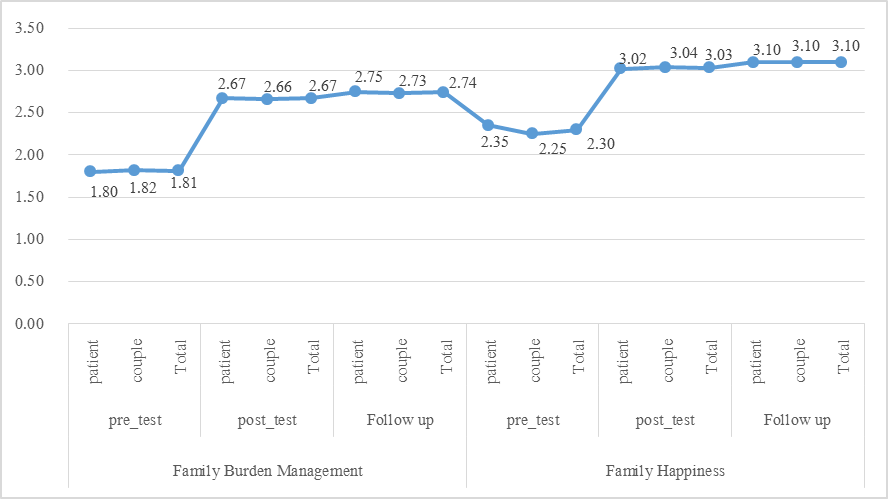 | Figure 4. Mean, Standard Deviation of family burden management and family happiness in experimental group |
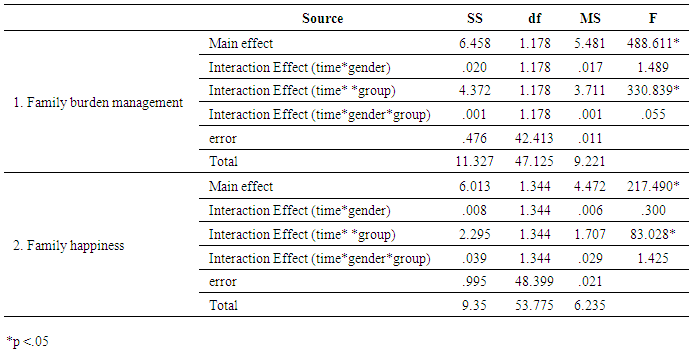
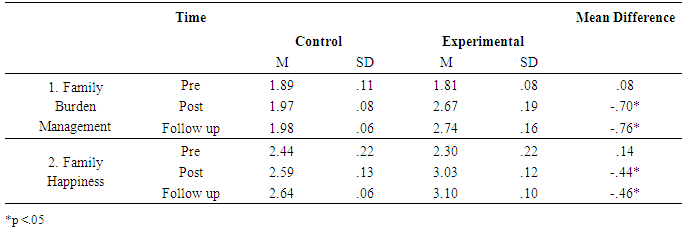
From Table 6 - Table 7 could explained1. Family burden management no Interaction effect with time and gender (F = 1.489, p > .05) and no Interaction effect with time, gender and group (F = 0.55, p > .05) but had the main effect in time of pre sections, post sections and follow up sections (F = 488.611*, p < .05) and had Interaction effect with time and group (F = 330.839*, p < .05) so researcher run post hoc test and found that family burden management of experimental group at post sections and follow up sections was higher than control group that statistically significance at .05 level.2. Family happiness no Interaction effect with time and gender (F = .300, p > .05) and no Interaction effect with time, gender and group (F = 1.425, p > .05) but had the main effect in time of pre sections, post sections and follow up sections (F = 217.490*, p < .05) and had Interaction effect with time and group (F = 83.028*, p < .05) so researcher run post hoc test and found that family happiness at post sections and follow up sections was higher than control group that statistically significance at .05 level.Table 6. Family burden management and family happiness of control and experimental group (Three-Way MANOVA Repeated Measurement)
 |
| |
|
Table 7. The post hoc test of family burden management and family happiness of control and experimental group
 |
| |
|
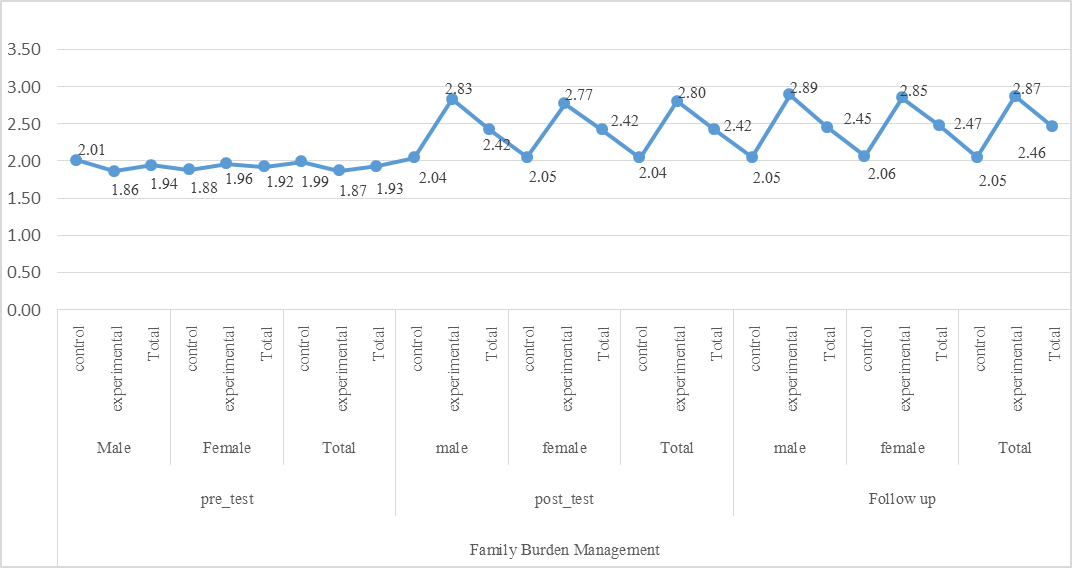 | Figure 5. Family burden management of control and experimental group at pre sections, post sections and follow up sections |
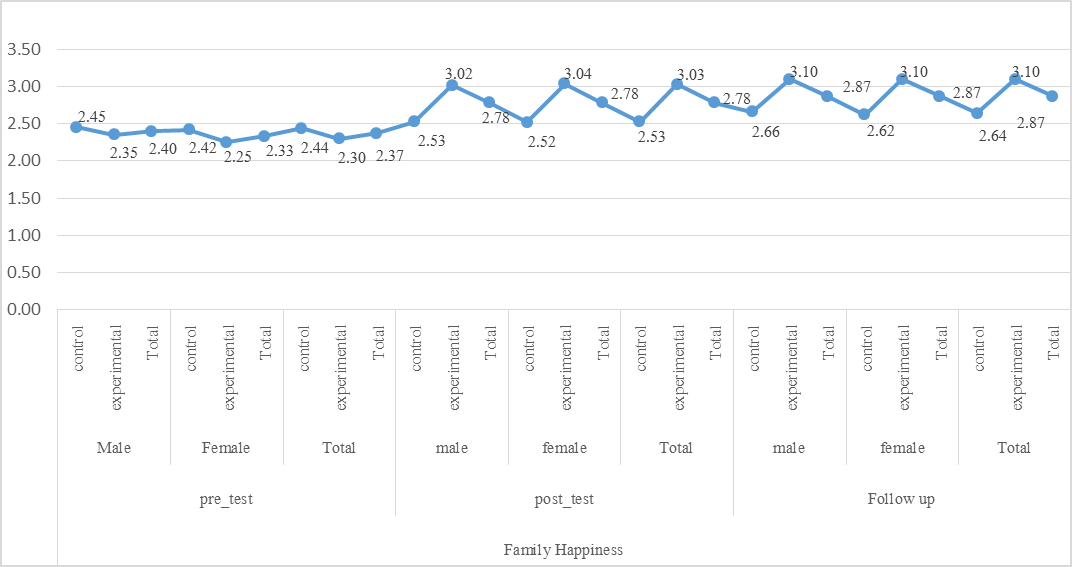 | Figure 6. Family happiness of control and experimental group at pre sections, post sections and follow up sections |
4. Discussion
The secondary Confirmatory factor analysis of family burden management of stroke patients in the Sixth National Health Service of Thailand shows that family burden management consist of four components1) family strain management2) family conflict management3) family guilt management4) family attitudeEach component can estimated the factor loading score of family burden management of stroke patients. This study found that four components are related, according to the family burden theory of Zarit, River, and Bach-Peterson (Zarit, Reever, & Bach-Petersons, 1980). In this study participants were stroke patients and their couple in the Sixth National Health Service of Thailand. The study found that the family burden management model developed by the researcher was based on the conceptual framework of Zarit, River and Bach-Peterson (Zarit, Reever, & Bach-Petersons, 1980) had a Cronbach's alpha coefficient of .935. Each questionair of the family burden management in Thai version for evaluated patients and their couple with stroke correlated moderate to high scores. The correlation coefficients are from .41 to .72 each component had Cronbach's alpha coefficients of .800, .809, .917, and .869, respectively.The family burden management influence to family happiness on stroke patients with coefficient of influence was .89 and could predict family happiness about 71 percentages.The assimilative integrated family counseling program consist of 12 sections and each section will take time about 60-90 minutes. It will schedule the appointment, date and time for families, individual counselors. During the section of 1 month, 2 months and 3 months, there will be a follow up by telephone every 2 weeks. In each encounter, the technique of Transgenerational theory was used: Interview, Genogram, Person to Person Relationship, Detriangulation, Confrontation and used Questioning, Scaling Question and the miracle question from SFBT and The wire experience from Humanistic Family Therapy for integrated to provide the most effective integrated family counseling from the one step to the next steps. The effects of assimilative integrated family counseling program of the experimental group had the mean score of overall components family burden management in post sections and follow up sections higher score than pre sections. The result show that because the assimilative integrated family counseling program that developed by researcher in the process of developing of assimilative integrated family counseling program for adult patient because in this group had impact on the patient itself and the family will have a severe impact such as in adulthood it is the age of built stability for the family, it is a time for take care of children in school age. The patient with stroke illness that requires continuing care lifelong for the patient and their couple is required to perform all four aspects of care, including direct care, activities daily living, prevention complications, rehabilitation, and economics. In addition, the research was developed assimilative integrated family counseling program was a psychological process for help to developed family relationships and communications for continuous improvement.Chulvith Rattanapolen (2006) studied family counseling to improve the marital quality of life in married spouses. The results of this study revealed that after family counseling, the experimental groups that focus on thinking married spouse Quality of Life Change to a better way significant at .05 level.Michael Robert Knerr (2008) studies on differtiation and power in couples therapy the sample was a client in counseling clinic and families in Ohio, USA. Measure the level of self-esteem, satisfaction in the relationship of life and the ability to handle family problems. The study indicated that after receiving the counseling program. spouses who are female have the ability to differentiation of themselves, satisfaction in the relationship of life, the ability to manage family problems was higher than before the counseling program.The result of assimilative integrated family counseling the experimental group had a mean score of family burden management higher level than control group. The mean score of family happiness was increased than control group due to assimilative integrated family counseling program patient and their couple have the opportunity to join together in the counseling sessions. The husband and wife have talked about what they might not be able to talk before from the consultative activities, they both have the opportunity to face talk, consult more, understand each other more, have been drawing family tree, watch a video, listen to music, make the wire experience and these activities families was not done before. At the end, these activities have improved the family burden management and family happiness with this assimilative integrated family counselling.
5. Conclusions
The family burden management in Thailand context consist of four components: family strain management, family conflict management, family guilt management and family attitude.The assimilative integrated family counselling could be applied to improved and especially helpful for families with chronic illness. The twelve sessions of counseling program focus on the family member emotional unit where each family member interrelates in thinking, feeling, and behaviors within the family relationship system. Attention to the relationship inherited from many generations, because the belief that the relationship of each generation of inherited ancestors' behaviors patterns will help to understand and predict the performance of contemporary generations. It helps the counselor and family to understand and discover alternatives and suitable way. They can decided together: the counselor is responsible for helping, promote and help family, the family member: Self-awareness and effective decision-making could handle the tension, conflict, guilt that happen in the family and have a positive attitude towards the family.
Suggestion
Research1. Develop tools for measuring family happiness that it can measure the happiness level of family members as a whole.2. It should be study and develop counseling model that can use with many recipients at one time.3. A follow-up study on family burden and family happiness in long-term of stroke patients should be conduct. The research next time should be follow up in long term of care for correct program that can maintain family burden management and family happiness at 3 months and later.Chief ExecutiveThis study will be useful for hospital administrators, medical personnel, healthcare team, caregivers, and patients.
ACKNOWLEDGEMENTS
This dissertation researcher: Thank you all health personnel, patients and their families thank worship Asst. Prof. Dr. Pennapha Koolnaphadol, Prof. Dr. Pracha Inang, Prof. Dr. Rungnapa Panitrat, that approved and made the study was well done.
References
| [1] | Department of Mental Health, Ministry of Public Health. (2016). The Happiness Indicator (TMHI-15). Department of Mental Health, Ministry of Public Health. |
| [2] | Koolnaphadol P. (2016). Family counseling. Chonburi: Natikul Printing. |
| [3] | Guiwan Y. (2013). Analysis of structural equation models: AMOS. Bangkok: V-PRINT (1991). |
| [4] | Chuyingsakultip N., Chyvimol R., Purananon D., & Srichannil C. (2016). Family Burden of Stroke Patients in Rayong Hospital Thailand. International Journal of Applied Psychology 2016, 6(1): 15-19. |
| [5] | Corey, G. (2009). Theory and Practice of Counseling and Psychotherapy. Eight Edition. USA. |
| [6] | Diener, E. (1984). Subjective Well-Being. Psychological Bulletin 1984, 95: 542-575. |
| [7] | Diener, E., Emmons, R., Larsen, R., & Griffin, S. (1983). The Satisfaction with Life scale. Manuscript submitted for publication, University of Illinois at Urbana Champaign. |
| [8] | Goldenberg H., & Goldenberg I. (2013). Family Therapy. 8th edition. Cengage Technology Edition. For use in Asia only. Singapore. 205-238, 422-423. |
| [9] | Gray, R. (2012). Happiness in Thailand. In H. Serin, & G. Davey (eds.). Happiness across Cultures. Volume 6 of the series Science across Cultures: the History of Non-Western Science 137-148. |
| [10] | Howell, D. C. (1999). Fundamental Statistics for the Behavioral Sciences (4th ed.). Pacific Grove, CA Brook/Cole. |
| [11] | Howell, D. C. (2013). Statistical Methods for Psychology (8 th ed.). Cengage Learning, ©2013. |
| [12] | Michael, R. K. (2008). Differtiation and Power in Couples Therapy. Dissertation the Ohio State University. |
| [13] | Rattanapolen C. (2006). Family counseling for improving the quality of married life. Dissertation. Srinakharinwirot University. |
| [14] | World Stroke Organization. (2015). World Stroke Day Toolkit For Healthcare Professionals. Available from: URL http://www.worldstrokecampaign.org/get-involved/world-stroke-day-2015.html. |
| [15] | World Stroke Organization. (2017). World Stroke Day 2017 What’s your reason for preventing stroke?. Available from: https://0x9.me/fNWIy. |
| [16] | Zarit, S.H., Reever, K.E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feeling of burden. The Gerontologist, 20(6), 649–55. |
| [17] | Zarit, S.H., Todd, P.A. & Zarit, J.M. (1986). Subjective burden of husbands and wives as caregivers: A longitudinal study. Gerontologist, 26: 260-266. |
| [18] | Zarit S.H., Zarit J.M. (1990). The Memory and Behavior Problems Checklist and the Burden Interview. Gerontology Center, Penn State University. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML