-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2017; 7(2): 49-56
doi:10.5923/j.nursing.20170702.03

The Relation between Psychological Well Being and Coping Strategies of Cancer's Relatives
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMona A. Elnagar1, Nahid F. El Gahsh2
1Psychiatric Nursing Department, Faculty of Nursing, Shebin El-kom, Menoufia University, Egypt
2Medical Surgical Nursing Department, Faculty of Nursing, Shebin El-kom, Menoufia University, Egypt
Correspondence to: Nahid F. El Gahsh, Medical Surgical Nursing Department, Faculty of Nursing, Shebin El-kom, Menoufia University, Egypt.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cancer causes changes in the family's identity, roles, and daily functioning. Serious illness of a loved one can disrupt a caregiver’s sense of self and relationships. The aim of the study was to determine the relation between psychological well being and coping strategies of cancer's relatives. Descriptive design was utilized for the current study. The study was conducted at outpatient clinics of Shebin Elkom University hospital In Oncology Department Menoufia Governorate. All cancer's relatives who came to the out patients clinic for follow up of their patients were selected during the period of data collection to be included in this study (100 person). Three instruments were used for data collection (1): Structured interview questionnaire to assess demographic and clinical data (2): The Coping Process Scale (3): Burden Interviews Scale. The results revealed that, there was significant correlation between duration of care giving and feeling burden of the relatives this means when the duration of care giving increases the relative feeling of burden increase. There is significant relation between mental disengagement as emotion focused coping and burden this means when the relative use mental disengagement as emotion focused coping the level of burden will increase. The most coping strategies used was exert of restrain (98%) followed by positive reinterpretation (92%) and 77% for seeking out information. Conclusion: There was negative non significant relation between coping strategies and burden. It means that when coping increase the burden will decrease. Recommendation: Relatives need supporting programs to establish real doctor- patient relationship .Stress management technique can be helpful to relief the family tension.
Keywords: Psychological Well being, Coping Strategies, Cancer's Relatives
Cite this paper: Mona A. Elnagar, Nahid F. El Gahsh, The Relation between Psychological Well Being and Coping Strategies of Cancer's Relatives, International Journal of Nursing Science, Vol. 7 No. 2, 2017, pp. 49-56. doi: 10.5923/j.nursing.20170702.03.
Article Outline
1. Introduction
- Cancer causes changes in the family's identity, roles, and daily functioning. Serious illness of a loved one can disrupt a caregiver’s sense of self and relationships [1]. Relatives usually concern with fear of cancer and its spread, helping patients deal with the emotional ramifications of the disease, and managing the disruptions caused by cancer [2]. They are become the most important caregivers for major disorders especially cancer, the relatives wellbeing and mental health may become seriously impaired. Relatives play an important role in supporting people with cancer [3].Cancer as a disease is often associated with distressing images of treatments and of suffering and death [4]. Especially family involved in caring for patients with cancer who are involved in caring for patients who are dying or have a terminal stage and are faced with the process of dying. Working with these patients and their families can be emotionally demanding and challenging [5]. The costs that families incur in terms of economic hardship, social isolation and psychological strain are referred to as family burden [6]. Many families' member experience significant stress and subjective burden. Not only is such likely stress to affect the well being of the relatives and ability to support the patient but it may also have an impact on the course of illness itself and on outcome of the client [7]. Cancer affects the quality of life of family caregiver or relatives, and feel overwhelmed and this leads to negative effect on psychological well being and physical well being as well and loss of control and difficulty in coping [8, 9] Serious illness of a loved one can disrupt a caregiver’s sense of self and relationships. A loved one’s diagnosis of a chronic or serious illness can create new communication challenges for caregivers [10].The care giver who have cancer's patients may have high level of burden related to caring. The level of burden experienced by caregivers of persons with cancers equivalent to that of caregivers of persons with other neurological and physical disorders such as Alzheimer's disease, mental retardation, diabetes [11]. Caregiver illness identity is useful for understanding patient and caregiver outcomes because the influence of caregivers is now widely accepted as a factor influential in patient treatment decision making [12]. Some families may respond to these identity changes by integrating illness into their relational identity [13]. Families in which a loved one is diagnosed with cancer also experience changes in their roles, identities, and daily activities [14].Discussion regarding the burdens of family caregivers and ways to reduce care giving burden become an important issues in psychiatric and medical and surgical nursing and care giver of relative with cancer as target in support and as planning intervention for cancer patients [15]. Serious illness, such as cancer, affects not only patients but also the family system [16]. The International Council of Nurses, stress that the nurses’ role is important when dealing with terminally ill patients in reducing suffering and improving the quality of life for patients and their families in the management of physical, social, psychological, spiritual and cultural needs [17, 18]. Nurses play an important role in developing a caring and supportive environment that acknowledges cancer in order to help patients and their family members to understand and deal with symptoms. Discussion regarding the burdens of family caregivers and ways to reduce care giving burden become an important issue in psychiatric nursing [19].
2. Methodology
2.1. The Purpose of the Study
- The purpose of the study was to determine the relation between psychological well being and coping strategies of cancer's relatives.
2.2. Research Question
- -Is there a relationship between psychological wellbeing and coping strategies of cancer's relatives.
2.3. Definition of Terms
- Psychological well-being was defined in this research as to what extent the individual will be free from burden feeling. Relatives were defined in this research as people with whom the patients lived and had to have some responsibility with respect to the patient's treatment but also to their daily living needs.
2.4. Design
- Descriptive design was utilized for the current study
2.5. Setting
- The study was carried out at outpatient clinics of Shebin Elkom University hospital In Oncology Department at Menoufia Governorate.
2.6. Subjects
- All cancer's relatives who came to the outpatient clinic for follow up of their patients were selected during the period of data collection to be included in this study. The total number of participants was 100 cancer's relatives (one for each patient who lives with the patient at home).
2.7. Tools
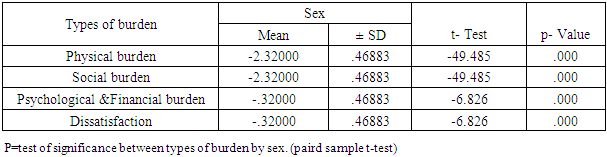
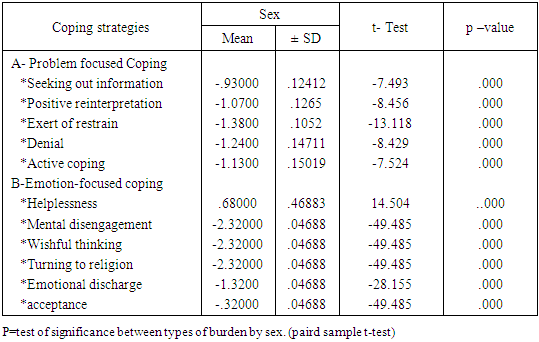
- The data of this study was collected by using the following tools:-2.7.1 Tool (1): Structured interview questionnaire sheet was developed by the researcher based on pertinent literature and guidance of expertise including three parts:-2.7.2 Part one: to assess socio demographic data as age, sex, gender, duration of care giver, degree of kinship and educational level.2.7.3 Tool (2) the Coping Process Scale: It is an Egyptian, standardized scale developed by Ibrahim (1994). It is consisted of 42 items divided into two coping methods: - a) problem focused coping b) Emotion focused coping.A- problem-focused coping (18 items): distributed as the following seeking out information and social support (3 items), positive reinterpretation (5 items), exert of restrain (4 items), denial (3 items), and active coping (3 items). B- Emotion-focused coping (24 items): distributed as the following helplessness (6 items), mental disengagement (5 items), wishful thinking (4 items), and turning to religion (3 items), emotional discharge (3 items) and acceptance (3 items).-The response will be in the form of 4 point rating scale where 1=do not agree, 2=agree to some extent, 3=generally agree, 4=totally agree.2.7.4 Tool (3) Burden Interviews Scale: This tool was adopted from Abd Elsalam (2002) which was translated and validated from the version of Zarit et al., (1986) Burden interviews Scale. Abd Elsalam (2002) burden interview scale: is consists of 22 items divided into 4 categories, physical (8 items), social (5 items), psychological and financial (6 items), and dissatisfaction burden (3 items). Five point Likert type scale was used where 0= Never, 1=Rarely, 2=Sometimes, 3=Alot, 4=Always.In addition to socio demographic data of the patient's relative gender, age, birth order, family income, level of education, occupation and duration of care giving.
2.8. Method
- - Before starting the study an official permission was obtained from the directors of the identified study setting to conduct the study. The aim and the nature of the study were explained to the subjects to obtain their oral consent.- The data was collected from June (2016) to December (2016).
2.9. Tools Developments
- Tools was translated by the researcher to Arabic language and tested for its content validity by group of five expertises in the psychiatric nursing staff. - The required modification was carried accordingly. Reliability, test retest reliability was applied. The tool Proved to be strong reliable. - A pilot study was carried out on 10 cancer's relatives to determine the applicability of study tool and the time needed to complete the tool.- Data collected through individualized interview with patient's relatives. Each interview took approximately 30 minutes per each patient's relatives.
2.10. Statistical Analysis of Data
- Results were collected, tabulated, statistically analyzed using statistical Package SPSS version 11.
2.11. Analytic Statistics
- - Chi-square test (χ2): was used to study association between two qualitative variables. Student t-test: is a test of significance used for comparison between two groups having quantitative variables. Mann-Whitney test (nonparametric test): is a test of significance used for comparison between two groups not normally distributed having quantitative variables. Pearson correlation (r): is a test used to measure the association between two quantitative variables. A P-value of < 0.05 was considered statistically significant.
3. Results
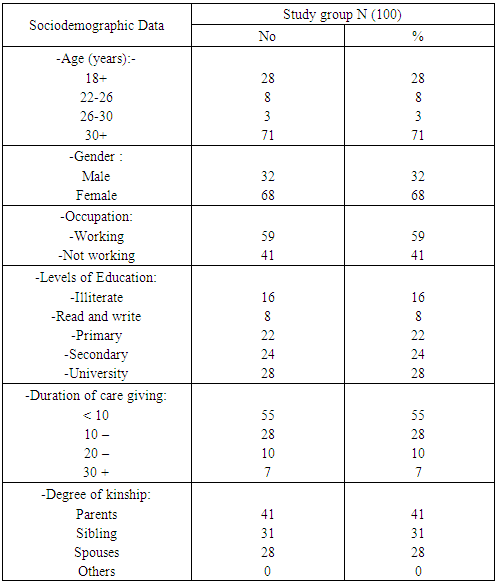
- Table (1): As shown in the table, the majority of the sample was (71%) who had the age more than 30 years old, (59%) of relevant were working, while (8%) of them were red and written, care giver about (7%) over 30 years ago while (28%) taken care giver less than 10 years and the majority of the subject (41%) in degree of kinship were parents while (28%) were spouses.
|
|
|

|
|
|
|
|
|
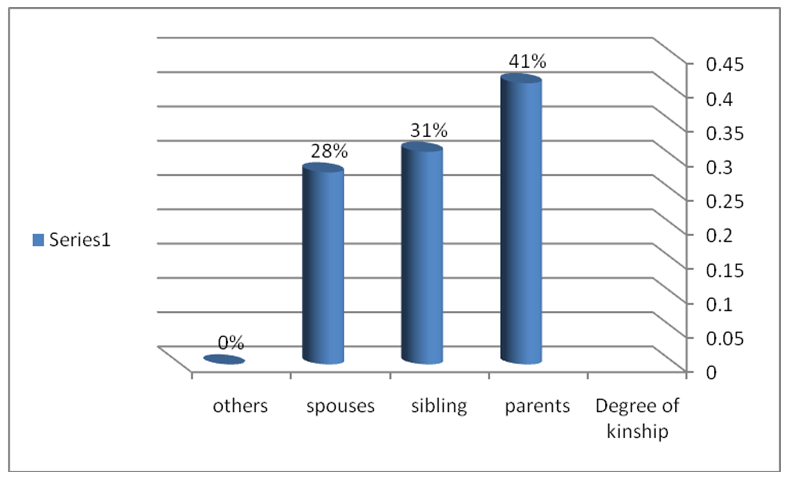 | Figure (1). Showed that the degree of kinship to cancer's relative |
4. Discussion
- Cancer affects the quality of life not just the patients but also for their relatives and leads to feeling of burden due to providing complex care. The relatives feel overwhelmed and suffer from significant stresses and high level of burden, psychological wellbeing become negatively, increased emotional distress, anxiety, and/or depression; feelings of helplessness and loss of control; and difficulty in coping with care giving roles.So, this study aimed to determine the relation between psychological well being and coping strategies of cancer's relatives.Regarding main types of kinship to patient the majority of the relatives were parents, followed by sibling (figure 1). This may be due to the patient most of time live with their parents and or with their sibling. This is congruent with, Lyer etal., (2014) who mentioned the family represents the largest group of care giving and the relatives were mostly parents and sibling of the patient [21]. Also Roughley, (2013) stated that the family spent most of time with their loved ones [22].
4.1. Level of Burden of Cancer's Relatives
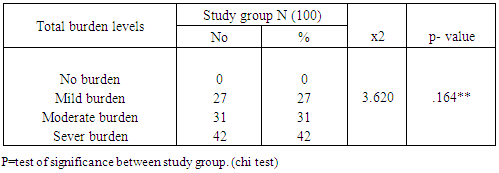
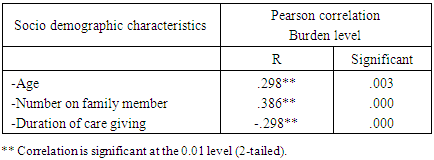
- Concerning level of burden, the results of the present study clarified that (75%) of the cancer's relatives had moderate and sever level of burden due to care giving responsibilities. This result was in accordance with Harris et al., (2013) who mentioned that all relatives of cancer's patient suffer from significant stresses and experiences high level of burden [23] and in consistent with Given et al., 2012, [24] Cora et al., 2012 who found that many relatives reports of the care giving burdens of living with someone with cancer are negative and psychological wellbeing decreases. This may be due to those patient need special care most of time so, the relative wellbeing and mental health become seriously impaired [25]. The finding of this study indicated that there was significant difference between demographic characteristics and burden level. This result is consistent with Ferrell & Mazanec, 2009 who found that relative age and socioeconomic status was associated with burden [26], and also consistent with Cuijpers and Stam, (2000) who found that the age of relative significantly correlated with burden [27].The current study results revealed that there was positive significant relation between duration of care giving and burden, it means that when duration of care giving increased the burden increased, this is due to the patient is not improving all time and most of time distressed and deteriorated and role in life become improper. But the finding of Murray etal., (2010) revealed that there was significant negative relation between family burden and duration of care giving [28], and Martens and Adding ton, (2001) found that shorter duration of care giving was associated with high relative burden [29].
4.2. Coping Strategies of Cancer's Relatives
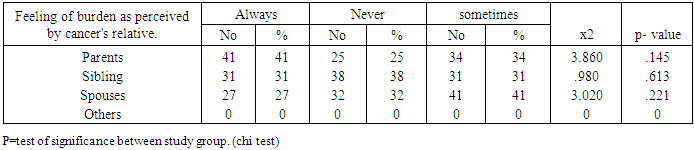
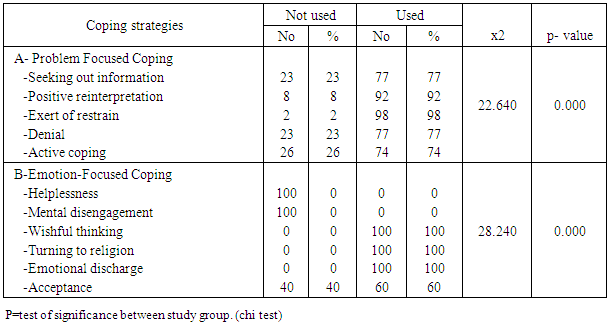
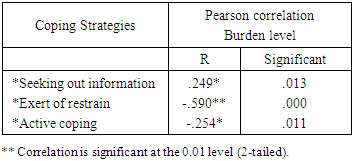
- Regarding coping strategies used by the cancer's relatives to deal with their problem, the current study results clarified that the majority of cancer's relatives use problem focused coping. This is may be due to the majority of the subjects were parents and siblings and it is difficult for them to accept the reality of their patients illness and this they hope that their parent's will be completely cured and take his chance and role in life. This was in accordance with the findings of Lazarus and Folkman, (1984) (Folkman & Moskowitz, 2000), reported that relatives used more problem –focused strategies [30, 31], while the findings of Chandrasekaran, Sivaprakash and Jayestri, (2002) reflected that two thirds of relatives did not attempt to use problem solving strategies as (information seeking, positive communication and patients social involvement) [32].The finding of this study indicated that the cancer's relatives use mental disengagement as coping strategies. This result was congruent with Phillips et al., (1998) who found that the caregiver chose to become emotional disengages from the patient this coping strategy does not seem desirable that is why the relatives may still feel trapped by care giving obligation [33], and Stone, (1998) who found that there was significantly greater proportion of caregivers that coped by trying to do one's mind off things by, watching T.V, sleep, smoke, use drug to relax [34], moreover, Mueser et al., (1997) shows that high emotional love and intimacy with the patients is related to low burden and high satisfaction in care giving [35].The result of the present study showed that there was a negative but not significant relation was found between coping strategies and burden of cancer's relatives this means that when relatives coping abilities increase the perceived burden of the relatives will decrease. Also due to the small number of the sample. This was consistent with Elsaid, (2008) who found negative relation between coping and burden.It can be concluded that, the majority of cancer's relatives reported that they always feel burden, and the relatives cope with their problems using wishful thinking followed by exert restrain and positive reinterpretation. Also the finding showed that coping strategies are negatively correlated with burden with no statistical significance. This means that when the coping increase the burden level decrease among relatives [36].
5. Conclusions
- • There was significant relation between mental disengagement as emotional –focused coping and burden this means when relative use mental disengagement the level of burden will increase. • There was significant correlation between duration of care giving and feeling of burden of the relatives this means when the duration of care giving increase the relative feeling of burden will increase. • The coping strategies used most of them was wishful thinking (100%) followed by exert restrain (98%) and 92% for positive reinterpretation.• All of this refer to that the families need Caring and monitoring of well being, exploration of their needs, assessing effectiveness of family support are relevant to focusing and improving care.
6. Study Recommendations
- 1- Relative support programs should be establish, support are relevant to focusing and improving care for the family.2- Stress management technique establish to help family to cope with their burden.