-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2016; 6(2): 25-34
doi:10.5923/j.nursing.20160602.01

Patients' Satisfaction about Quality of Care and Aggressive Behavior in Psychiatric Hospitals
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaaly Ibrahem El Malky 1, Safaa Diab Abd El Wahab 2, Sabah Hassan El-Amrosy 2, Elham Ramzy El Fiky 3
1Assistant Professor of Psychiatric and Mental Health Nursing, Faculty of Nursing, Menoufia University, Egypt
2Lecturer of Psychiatric and Mental Health Nursing, Faculty of Nursing, Menoufia University, Egypt
3Clinical instructor of Psychiatric and Mental Health Nursing, Faculty of Nursing, Menoufia University, Egypt
Correspondence to: Sabah Hassan El-Amrosy , Lecturer of Psychiatric and Mental Health Nursing, Faculty of Nursing, Menoufia University, Egypt.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Patient satisfaction about quality of care has been found to be an important factor related to inpatient aggression. Aim: The aim of the study was to assess the relationship between patients' satisfaction about quality of care and their aggressive behavior in inpatient psychiatric hospitals. Design: descriptive co-relational study design was used. Setting: this study was conducted at Meet Khalaf and Tanta Psychiatric Hospitals. Sample: a convenience sample consisted of 100 patients who were hospitalized in the above mentioned settings and fulfilled the inclusion criteria. Data collection: Three tools were used; Structured interview questionnaire, quality of psychiatric care questionnaire for measuring inpatient opinion and the social dysfunction and aggression scale (SDAS-9). Results: The study revealed that 52% of the studied sample had low satisfaction about the quality of care. 32% of the studied sample used physical act of aggression. There was a highly statistically significant negative correlation between patient satisfaction about quality of care and their forms of aggression. Conclusions: It was concluded that when the patients had low satisfaction about quality of care, they would have many forms of aggression. Recommendations: Based on this results educational program should be given for psychiatric nurses regarding therapeutic effective communication, activity therapy and effective ways for managing aggression in order to de-escalate the patients’ emotion and behavior.
Keywords: Satisfaction, Quality of care, Inpatient aggressive behaviour
Cite this paper: Maaly Ibrahem El Malky , Safaa Diab Abd El Wahab , Sabah Hassan El-Amrosy , Elham Ramzy El Fiky , Patients' Satisfaction about Quality of Care and Aggressive Behavior in Psychiatric Hospitals, International Journal of Nursing Science, Vol. 6 No. 2, 2016, pp. 25-34. doi: 10.5923/j.nursing.20160602.01.
Article Outline
1. Introduction
- Patient satisfaction is defined as a subjective evaluation of the health service received against client’s expectations [1]. Patient satisfaction has become a frequently used tool for evaluating programmers and treating outcomes, as well as an important factor in relation to adherence to treatment and continued psychiatric care [2]. Improved patient satisfaction not only leads to an enhanced patient experience; it is also associated with improved treatment outcomes. Improved patient satisfaction was correlated with higher quality hospital care. For example, higher patient satisfaction has been associated with reduced readmission rates. Furthermore, improved patient satisfaction has even been correlated with reduced inpatient mortality [3]. Patient satisfaction is one of the barometers that reflect how well a health care system is working. There is a growing interest in the measurement of patient ratings of satisfaction as one marker of quality in psychiatric care. The quality of care in health facilities is a critical determinant of the utilization of health facilities globally, and without satisfactory quality, service users are likely to become disillusioned. This is likely to negatively affect mental health seeking behavior, treatment compliance and overall care. There is growing evidence that the perceived quality of health care services has a greater influence on patient behaviors. [2]. An association between staff experiences of violence and patient-rated quality of care has been found. Aggression often occurs in situations when patient’s needs are not fully met and anger and frustration arise. The occurrence of aggression is associated with the complex interaction of both intrapersonal and interpersonal factors. Several intrapersonal factors are related to factors within the social context in which the patients functions, such as poverty, stressful life-events and victimization. Deficits in both the intrapersonal as interpersonal factors, in combination with stressful environmental factors, may contribute to patients’ vulnerability for aggressive responses [4].In recent years, patients have increasingly been considered as consumers or customers by the health care system. It has become increasingly important for healthcare professionals to systematically measure patients’ satisfaction with their care. Health care staff awareness about the needs and wants of their patients significantly affect the patients’ satisfaction. Measuring patient satisfaction involves evaluating patient’s perceptions and determining whether they felt that their needs were adequately met [5].professional psychiatric nurses should understand that Health care should be delivered with compassion, empathy and responsiveness to the patient’s needs, values and preferences and equity: health care services should be provided on the basis of clinical need, regardless of personal characteristics such as age, gender, race, ethnicity, language, socioeconomic status or geographic location, such that health care contributes to reduced differences in health status and outcomes across various subgroups [6].
2. Significance of the Study
- Violence and aggression in inpatient units constitute a major workplace hazard for mental health nurses, who must take account of many considerations when dealing with potentially aggressive or violent patients. According to a large number of theoretical and empirical studies on violence in psychiatry, the occurrence of violent incidents, as well as their management, has to be regarded as a product of the interaction of several variables. Among them are patient variables, e.g. environmental or setting variables, e.g. ward characteristics, interactional variables, and staff variables, e.g. education and attitudes [7]. Staff surveys show that between 75% and 100% of nursing staff on psychiatric units have been assaulted by a patient at some stage in their careers [8]. Between 2011 and 2013, workplace assaults ranged from 23,540 and 25,630 annually, with 70 to 74% occurring in health care and 27 out of the 100 fatalities in health care that occurred in 2013 were due to assaults and violent acts in USA [9].Because nurses spend a lot of time with patients, they affect patient experiences of care. It seems that when patients have positive experiences of nursing care, nurses also experience a good and healthy work environment. A healthy work environment fosters a climate in which nurses are challenged to use their expertise, skills and clinical knowledge. Furthermore, nurses who work in such an environment are encouraged to provide patients with excellent nursing care [10].Patient satisfaction have been identified as an indicator for evaluating and improving the quality of care. When healthcare organizations assess patient satisfaction, professionals can use the results for internal quality improvements. Professionals use patient experiences and preferences to adjust their own practice and to make visible their contribution to patient outcomes. Measures that improve patient satisfaction with the environment and treatment and provide inpatients with meaningful activities contribute to reduction of inpatient aggression [11]. Thus, psychiatric nurses should assess patients’ satisfaction about quality of care to determine its relation to patient aggressive behavior.Theoretical definitions:Patient satisfaction: is a subjective evaluation of the health service received against client’s expectations [1].Quality of care: is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge [12].Inpatient aggression: refers to a range of behaviors that can result in both physical and psychological harm to oneself, others or objects in the environment that occurs during patient’s hospitalization [13].Operational definitions:Patient satisfaction: patient satisfaction is operationally defined as the obtained patient satisfaction score measured by quality of psychiatric care questionnaire for measuring patients’ satisfaction and opinion about quality of care given to them at inpatient psychiatric hospital by [14].Quality of care: quality of care is operationally defined as the obtained quality of care score measured by quality of psychiatric care questionnaire for measuring patients’ satisfaction and opinion about quality of care given to them at inpatient psychiatric hospital by [14].Inpatient aggression: inpatient aggression is operationally defined as the obtained inpatient aggression score measured by the Social Dysfunction and Aggression Scale (SDAS-9) developed by [15].
3. Subjects and Method
3.1. Aim of the Study
- To assess the relationship between patients' satisfaction about quality of care and aggressive behavior in patients psychiatric hospitals.
3.2. Research Questions
- - Are patients satisfied about the quality of care provided to them in psychiatric hospitals?- Are there relation between patients' satisfaction about quality of care and aggressive behavior in psychiatric hospitals.
3.3. Research Design
- Descriptive co-relational design was utilized to achieve the aim of the study.
3.4. Setting
- The study was conducted at Meet Khalaf Psychiatric Hospital that related to The Ministry of Health and Tanta Psychiatric Hospital that related to Tanta University Hospital.
3.5. Subjects
- A convenience sample of 100 adult patients from the two hospitals of the above mentioned settings who fulfilling the following inclusion criteria was recruited in the study.Inclusion criteria:Adult hospitalized patients Aware and able to interactReady to participate in the studyExclusion criteria:Acute cases early admitted for less than one month because his condition might effect on his emotion and behavior.
3.6. Tools
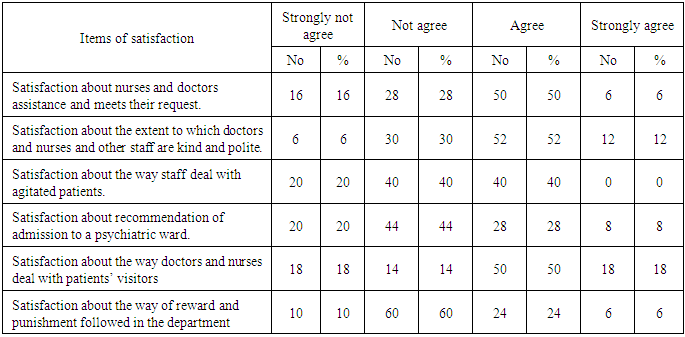
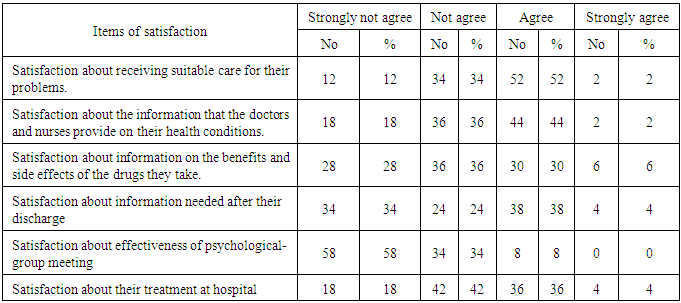
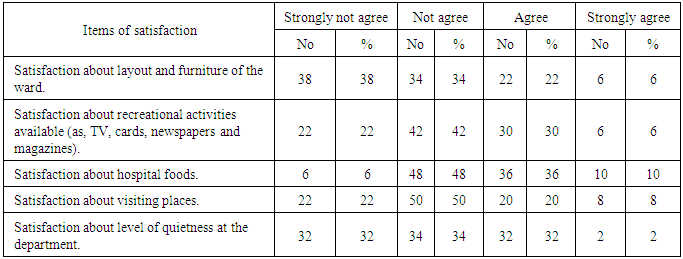
- Three instruments were used for data collection for this study.Tool (I)-Structured Interviewing Questionnaire: Socio demographic characteristic structured interview schedule which include socio-demographic characteristics including: age, sex, education, occupation, income.Tool (II): -Quality of psychiatric care questionnaire:This questionnaire was devolved by [14]. Is used to measure patient satisfaction and opinion about the quality of care given to them. It consists of 12 items modified by the researcher to be 17 items in the form of a Likert-type scale with four points (0–3), with higher numbers indicating greater satisfaction. The possible answers were: (0) ‘strongly not agree; (1) ‘not agree; (2) ‘agree; (3) strongly agree. These items cover the following aspects of care: (1) suitability of care; (2) staff availability; (3) staff kindness and politeness; (4) treatment of agitated patients; (5) information received about health conditions; (6) information about drug treatment; (7) information about care after discharge; (8) physical environment; (9) recreational activities; and (10) psychological-group activities (each morning, a cognitive-behavioral psychotherapy group was held in the ward); (11) patient's recommendation for others admission to the same psychiatric hospital; (12) patient's opinion about daily activities and treatment within the hospital. The scoring system was categorized as follows:Score (0-8) No satisfactionScore (9-25) Low satisfactionScore (26-42) Moderate satisfactionScore (43-51) High satisfaction Tool (III):- Aggression and Social Dysfunction Scale:This tool was developed by [15]. Is used to measure social dysfunction and aggression. It consists of 9 items used a Likert-type scale with five points (0–4) 0 =Not present 1 = doubtful 2 = mild 3 = moderate 4 = severe. These items cover the following aspects: irritability, negativism/uncooperative behavior, dysphoric mood, socially disturbing/provocative behavior, non-directed verbal aggression, directed verbal aggression, physical violence towards things, physical violence towards staff members, and physical violence towards non-staff. Scoring system was categorized as following:Score (0-5) No aggressionScore (6-10) Passive aggressionScore (11-17) Verbal acts of aggressionScore (18-36) Physical acts of aggression.
3.7. Content Validity
- Before starting, the data collection tools were translated into Arabic and tested for its content validity by a group of experts in psychiatric nursing to check the relevance, coverage of the content and clarity of the questions. The required modification was carried out accordingly.
3.8. Reliability of the Tools
- Test-retest reliability was applied for tool (2). The tool proved to be strongly reliable (r. = 0.8222).Test-retest reliability was applied for tool (3). The tool proved to be strongly reliable (r. = 0.80).
4. Pilot Study
- Pilot study was carried out before starting data collection; this was done to estimate the time required for filling out the sheet and also to check the clarity of the tools.
5. Procedure of Data Collection
- - Before starting any step in the study an official letter was addressed from the faculty of nursing, Menoufia University to the director of the General Secretariat of Mental Health, Meet Khalaf Psychiatric Hospital at Menoufia governorate and Tanta Psychiatric Hospital at Tanta Governorate, requesting their cooperation and permission to conduct the study.- Once the official permissions were obtained from the principal person, and the other authorized personnel from the various settings, the researcher started the data collection. - All of the authorized personnel provided the needed information about the study from the researcher. - All patients who fit in the inclusion criteria were approached by the investigator to fill the questionnaires according to the following steps: - The investigator started data collection by introducing herself to the participant. - Oral informed consent was obtained from each participant. - Then a brief description of the purpose of the study and the type of questionnaire required to fill was given to each participant.- Data collected were done through interviewing with the patients in hospital. - The researcher started to collect the data from patients two days/ per week for each hospital. - Each interview lasted for 20-30 minutes, depending on the response of the interviewer. The process of data collection took a period of six months.
6. Ethical Consideration
- An oral consent was taken from each patient in the study after explaining the purpose and the importance of the study. The subjects who agreed to participate in the study were assured about confidentiality and anonymity of the study. They were informed about their right to withdraw from the study at any time without giving a reason.
7. Statistical Analysis
- Data entry and statistical analysis were done using the statistical package for social sciences (SPSS version 16). Data were presented using descriptive statistics in the form of frequencies and percentages for qualitative variables, mean and standard deviation for quantitative variables. Qualitative variables were compared using the chi - square test and Kruskal Wallis and test correlation coefficient is used to measure the direction and strength of the correlation between variables. A significant level value was considered when P-value < 0.05 and highly significant level value was considered when P value < 0.001 while P value of > 0.05 indicated non-significant.
8. Results
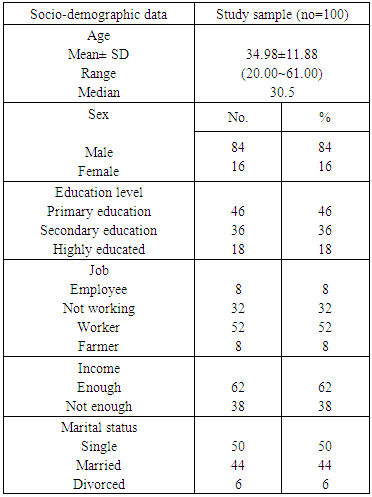
- Table (1): This table reveals that the mean age of the studied sample are 34.98±11.88, majority of the sample (84%) are males, more than half of the sample (64%) are from Tanta Mental Health Hospital, near to half of the sample (46%) are in primary education, more than half of the sample (52%) are worker, more than half of the sample (62%) have enough income and 50% are single.
|
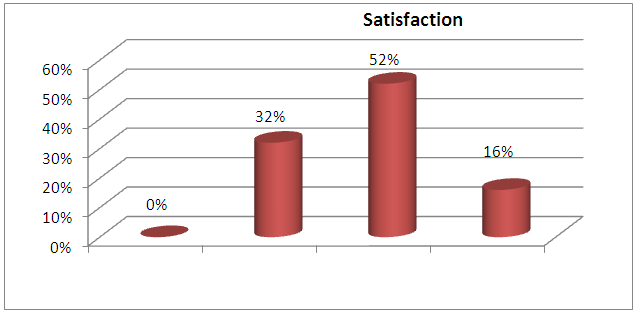 | Figure (1). Distribution of the total Levels of patients’ satisfaction about the quality of care |
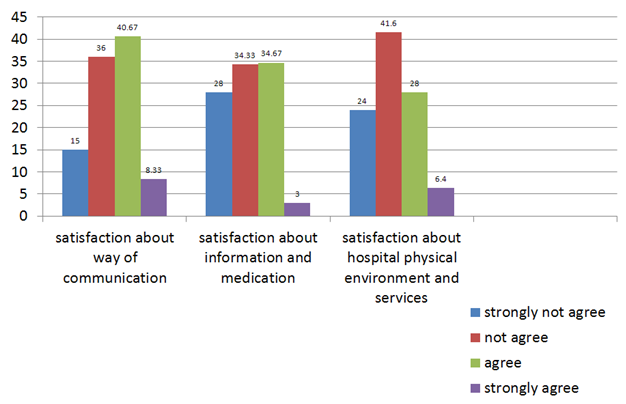 | Figure (2). Distribution of the Mean score for patients’ satisfaction about the quality of care |
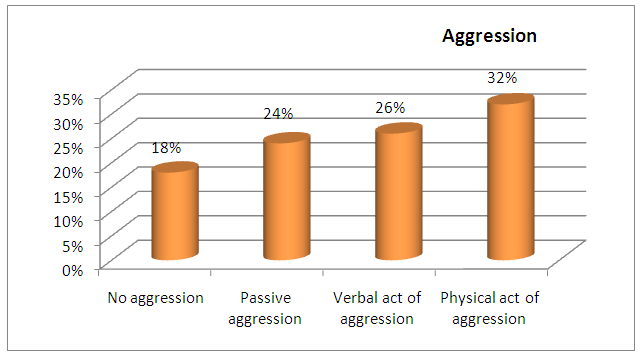 | Figure (3). Distribution of the Forms of patients’ aggression in inpatient psychiatric hospitals |
|

|
|
|
9. Discussions
- Patient satisfaction is becoming one of the most important measures that healthcare systems look at when they are judging the efficiency and effectiveness of the services being provided. Proper measurement of psychiatric patient satisfaction is essential in the evaluation of mental health services. Levels of patient satisfaction are considered to be an indicator of quality of care and are specifically related to compliance with treatment, improvement in health status, and future use of psychiatric services [16]. Aggression and violence are common in psychiatric wards [17]. Patients with a higher level of aggressive behavior were less satisfied with the ward's physical and psychosocial environment, the treatment design and the treatment program [18]. Understanding patients' satisfaction with services helps to inform the development of improved mental health programs designed to meet patients' needs [16]. So, the aim of the study was to assess the relationship between patients' satisfaction about the quality of care and aggressive behavior in inpatient psychiatric hospitals.The results of this study showed that half of the sample were agreed about meeting their request when asking for help from doctors, nurses or other staff. This was supported by [19] which showed that above two fifths of the sample agreed about availability of a member of the health care team when the patient needed one. This study showed that two fifths of the sample agreed about the way of staff dealing with agitated patients. This was inconsistent with [20] who founded that patients reported low satisfaction in the area of restrictions on movement, with near to half of the sample evaluating restrictions as negative or very negative.The current study showed that more than half of the sample agreed about doctors, nurses and other staff kindness and politeness. This was consistent with [19] who showed that half of the sample strongly agreed about a patient’s treatment with dignity and respect. The results of this study show that two thirds of the sample didn’t agree about the level of quietness at the department. This was inconsistent with [21] who reported that above two fifths of the sample were highly satisfied with the quietness in the ward. This might be due to crowding and disorganization at the time of visiting and cleaning. The current study showed that above two fifths of the sample didn’t agree regarding recommendation of admission to a psychiatric ward. This was inconsistent with [21] who reported that tenth of the sample wouldn’t hesitate to come back or to recommend people to the facility. This might be due to fixed routine, roles and way of caring or might be due to difference on hospital discipline. This study showed that above half of the sample agreed that the care received was suitable for treating their problems. This was supported by [19] who found that above half of the sample agreed about receiving appropriate treatments for any physical health needs they had. The results of this study showed that more than one third of the sample didn’t agree about receiving information about drug treatment benefits and side effects. This was consistent with [19] who reported that near one third of the sample didn’t agree about receiving acceptable explanations about the side effects of medication. This might be because most nurses working on the study setting were diploma nurses and were lacking in their information and needed education and training about medication.This study showed that near three fifths of the sample didn’t agree about information given to them on discharge. This was inconsistent with [19] who reported that two fifths of the sample were strongly satisfied with the amount of information they received at discharge about their follow-up care. This might be because staff in the study setting lacked knowledge about information that they should give to the patients on discharge. The results of the current study showed that near three quarters of the sample didn’t agree about the layout and furniture of the hospital ward. This was inconsistent with [21] who reported that above eighths of the sample didn’t agree that the environment of care met their expectations. This might be due to overcrowding, lack of supplies, old furniture and unavailability of specific places for food, changing clothes, visits and recreation e.g. (garden). The current study showed that above two fifths of the sample didn’t agree about satisfaction about treatment within the hospital. This was inconsistent with [19] who found that above two fifths of the sample agreed that they were confident with the treatments they received during their hospital stay. This might be because treatment focused only on medication and no other treatment modalities due to lack of qualified staff and supplies or differences of the setting of the study and services given. This study showed that above three fifths of the sample didn’t agree regarding satisfaction about availability of recreational activities. This was supported by [20] who found that above three fifths of the sample felt that the opportunities for meaningful activities on the ward were only moderate or poor. This might be because there is no place, supplies or qualified personnel and shortage of staff. This study showed that above half of the sample didn’t agree regarding satisfaction about hospital foods. This was inconsistent with [19] who reported that above two fifths of the sample agreed about the high quality/standard of food received, and inconsistent with [21] who reported that near to a tenth of the sample were unsatisfied about quality of food while three percent were unsatisfied about quantity of food. This might be due to lack of quality, quantity, bad taste, bad preparation and bad way of offering food. This study showed that near three quarters of the sample didn’t agree about visiting places. This was inconsistent with [19] who found that above three fifths of the sample stated that they were always satisfied with the level of privacy.The current study showed that the highest mean score for patients’ agreements regarding satisfaction about the quality of care were in the way of communication of health team members. This was inconsistent with [22] who reported that patient-staff communication ranked second after patient-staff relationship. The lowest mean score for patients' agreement regarding satisfaction about the quality of care was about hospital physical environment and services. This was in contrast to [23] who reported that the majority of the respondents were moderately satisfied about hospital physical environment and services. Also, [24] found that the highest mean score belonged to the physical environment quality. This might be due to overcrowding, lack of supplies, old furniture and lack of specific place for eating, changing clothes, for visit and recreation e.g. (Garden).Generally, patient satisfaction is a valuable and widely used indicator of the quality of care, psychiatric inpatients are quite satisfied with their care [20] This confirm the results of the current study which showed that above half of the studied sample had low satisfaction while near one third had moderate satisfaction and above eighth of the sample had no satisfaction. This was inconsistent with a study by [25] who found that near three quarters of the sample were mostly satisfied while a near fifth of the sample was mildly satisfied and near tenth of the sample were dissatisfied. This differences in the present study than the result of above study could be due to the difference of the sample setting where psychiatric services provided abroad were more advanced than in Egypt.The results of the current study showed that near to one third of the studied sample use physical acts of aggression. This was in the same line with [26] who showed that two fifths of those presenting any recent aggressive behavior were physically aggressive during the hospitalization, Also [27] founded that the most frequent form of aggression was physical and [28] illustrated that nearly fifty percent of all aggressive incidents recorded internationally in psychiatric units involved physical violence. This was in contrast to [29] who reported that near two fifths of sample had verbal, above one fifth of sample had threats and above eighth of the sample had physical aggression. This might be due to patient’s dissatisfaction about hospital environment and lack of information about his treatment.The results of the current study showed that there was a highly statistically significant negative correlation between patient satisfaction about the quality of care and their forms of aggression. This was supported by [30] who found that the strongest negative correlation was between the angry and aggressive behavior subscale and general satisfaction index and also in the same line with [31] who showed that violence was also associated with significantly lower staff ratings of the quality of care provided by the hospital. In conclusion, we can say that this result illustrated the aim and hypothesis of the study which illustrated that patients who were less satisfied with quality of care, would present great forms of aggression.
10. Conclusions
- Based on the findings of the current study, it can be concluded that: More than half of the studied sample have low satisfaction about the quality of care while about one third of the studied sample use physical acts of aggression. There is a highly statistically significant negative correlation between patient satisfaction about quality of care and their forms of aggression.
11. Recommendations
- Based on the findings of the present study, the following recommendations are suggested:1- Educational programs for psychiatric nurses about:A- Effective therapeutic communication with psychiatric patients.B- Medication and its side effects and discharge plan.C- Activity therapy and the importance of its application to psychiatric patients in improvement of patient’s symptoms and reduction of aggression.D- Effective ways of managing aggression.Further research could be done to assess the role of the care providers’ perspectives and how they contribute to the patient’s appraisal of satisfaction with the quality of psychiatric care. Further research could be done to assess relationship to voluntary and involuntary patient status. Also, look at age, and diagnosis length of stay.
ACKNOWLEDGEMENTS
- The researchers wish to acknowledge the participants who took part in the study, and the service for allowing this research to be undertaken.