-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2016; 6(1): 19-23
doi:10.5923/j.nursing.20160601.03

A Descriptive Study to Assess the Coping Strategies among Elderly Patients with Heart Failure in a Selected Private Hospital, Malaysia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNg Sook Ting , Yang Yuen Hong , Mini Rani Mary Beth
Division of Nursing, International Medical University, Kuala Lumpur, Malaysia
Correspondence to: Mini Rani Mary Beth , Division of Nursing, International Medical University, Kuala Lumpur, Malaysia.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

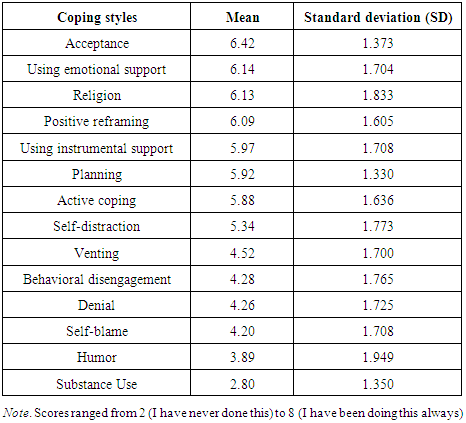
The Center for Disease Control and Prevention (2013) reports that there are about 1.5 million people in the United States have heart failure and half of them who develop heart failure die within 5 years of diagnosis [1]. The objective of this study is to assess the coping strategies among elderly patients with heart failure in a private hospital, Malaysia. The theoretical framework used is Sister Callista Roy’s Adaptation Model. Methods: A descriptive design was used. Convenient sampling technique was used to select 135 elderly participants with heart failure. Coping strategies among the elderly patients with heart failure were determined by using Brief COPE questionnaire. The results were analyzed by using Predictive Analytics Software (PASW) version 18 and presented in tables and figures. Results: The results indicated that the most frequently used coping strategies were acceptance, using emotional support, religion, positive reframing, using instrumental support, planning, and active coping. Whereas, the less frequently used coping strategies were self-distraction, venting, behavioral disengagement, denial, self-blame, humor, and substance use being used least frequently. Conclusion: Elderly patients with heart failure used adaptive coping strategies and emotion-focused coping strategies to cope with the illness in this study.
Keywords: Coping strategies, Elderly patients, Heart failure
Cite this paper: Ng Sook Ting , Yang Yuen Hong , Mini Rani Mary Beth , A Descriptive Study to Assess the Coping Strategies among Elderly Patients with Heart Failure in a Selected Private Hospital, Malaysia, International Journal of Nursing Science, Vol. 6 No. 1, 2016, pp. 19-23. doi: 10.5923/j.nursing.20160601.03.
Article Outline
1. Introduction
- The American Heart Association (2013) reports that most half of the patients with heart failure die within 5 years of the diagnosis [2]. Even though there are advances in the medical treatment, the prognosis of heart failure is still poor. According to the Health Informatics Centre of Malaysia (2011), cardiovascular disease (CVD) is the commonest cause of deaths [3] in Malaysia. The annual report by the Ministry of Health Malaysia (2009) also shows heart failure is one of the main causes of death in Malaysia. Heart failure accounts for 6%-10% of all acute medical admissions in the hospital. This shows that heart failure is also one of the health problems that should be paid more attention to reduce the mortality and morbidity rates [4]. The objective of this study is to assess the coping strategies among elderly patients with heart failure in a selected private hospital.According to a heart and stroke statistics report from the American Heart Association (2013), one out of nine deaths included heart failure as a contributing cause in the United States 2009 [2]. Heart failure seriously affects patients and their family caregivers’ quality of life [5]. Farcas and Nastasa (2011) reported that patients with heart failure mainly use emotional-based coping (acceptance, seeking emotional support, religion) [6]. A better understanding of coping styles among the population can help clinicians and researchers in developing interventions and thus improving heart failure outcomes [7]. Molloy, Johnston, and Witham (2005) found that high levels of emotional distress were relatively identified among caregivers of congestive heart failure patients [8]. Most couples experienced a shift in roles and responsibilities within their partner relationship and distress following being afflicted with cardiac disease [9].The study is guided by the theoretical framework developed by Sister. Callista Roy’s adaptation model (RAM). The use of this conceptual model is to facilitate adaptation of elderly heart failure patients with this chronic illness, to recognize the realities imposed by the illness and restructuring self and the environment amid the new experience [10]. The reason for choosing this model as a framework of this study is due to the application of the three environmental stimuli defined by Roy adaptation model. The focal stimulus in this study is the diagnosis of heart failure; the contextual stimuli are the demographic data and the residual stimuli are the unknown factors that may affect coping strategies of the elderly patients.
2. Methodology
- A non- experimental descriptive design was used. Convenient sampling method was used to select 135 participants who fulfilled the inclusion criteria.
2.1. Inclusion Criteria
- Ÿ Both male and femaleŸ Age 60-80 years oldŸ Have been diagnosed with heart failure Ÿ Able to read and understand English and Bahasa Melayu.
2.2. Exclusion criteria
- Ÿ Unable to read and understand English and Bahasa MelayuŸ Aged less than 60 years old or more than 80 years old
2.3. Instrument
- The instrument used in this study is “Brief COPE” which was developed by Dr. Charles S. Carver (1997) from University Miami, Florida. Permission was obtained to use the instrument. The instrument consists of part A: demographic data and part B: Brief COPE questionnaire. The brief COPE comprised of 28 items, which measures 14 conceptually differentiable coping reactions. They are active coping, planning, positive reframing, acceptance, humour, religion, using emotional support, using instrumental support, self-distraction, denial, venting, substance use, behavioural disengagement and self-blame. The pilot study was conducted to determine the reliability of the original questionnaire. The Cronbach alpha value was 0.9. The validity of the questionnaire was done by a cardiologist and a nurse manager from the cardiac ward of the hospital.
2.4. Ethical Considerations
- The study design was approved by the International Medical University (IMU) Joint-Committee of the Research and Ethics Committee and also the Research Ethics Committee of the study hospital. Written consent was obtained from the participants before the questionnaire was distributed. Participants were allowed to withdraw from the study at any point of time. All data collected from the participants were kept private and confidential.
2.5. Data Analysis
- Descriptive statistical analysis was used for Part A, demographic data. The Part B, Brief COPE data were analyzed by using Predictive Analytics Software (PASW) – version 18.
3. Results and Discussion
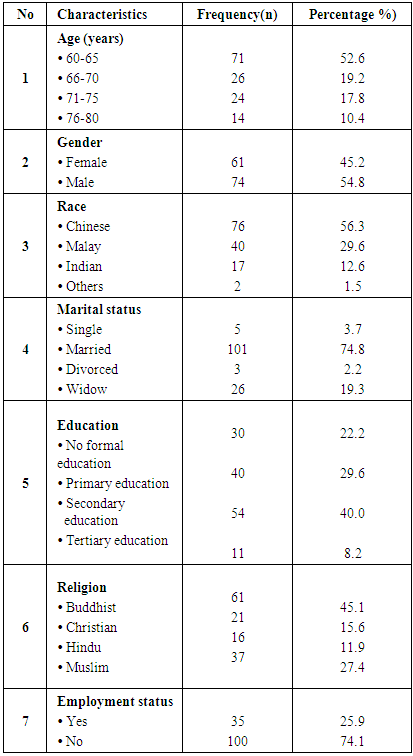
- The socio-demographic data of the participants namely age, gender, race, marital status, education level, religion, employee status and occupation were obtained as described in Table 1.
|
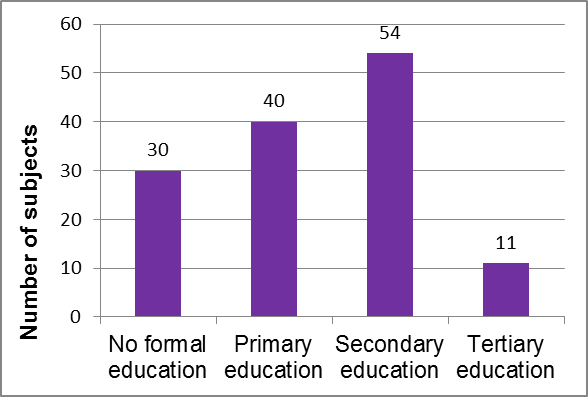 | Figure 1. Education level of elderly patients with heart failure |
|
|
4. Conclusions
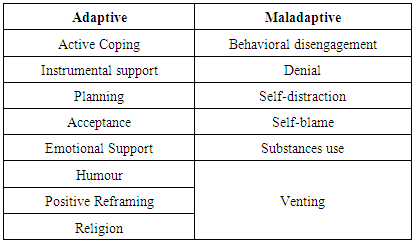
- The goal of treatment for heart failure are not focused on recovery, but mainly aim on survival rates, reduction in readmission rates and improvement of quality of life [13]. It is important for nurses as teachers and counsellors to teach and helpthem to recognize and cope with stressful psychological or social problems [14]. The findings of this study may provide information that helps nurses in future education to identify the coping strategies among the elderly patients and enable them to cope better with their health problems. Besides, the findings of the study may assist nurses or caregivers in developing interventions that can improve heart failure outcomes among the patients with heart failure. Nurses can advise patient on any necessary modification on the coping strategies to make better result for the patient to cope with the illness. Thus, the information may help the hospital management in developing future care and policy for the elderly patients in improving their coping skilled and quality of life. Each individual has a different strategy to cope with the changes in life. It is a stressful living condition for patients with chronic illnesses like heart failure suffering from significant and recurrent symptoms, repeated worsening and hospitalizations as well as the unpredictable outcomes. In the present study, patients were found using adaptive and emotion-focused coping strategies to cope with their heart failure condition. Coping can be adaptive or maladaptive. Effective coping strategies results in adaptation, whereas ineffective coping results in maladaptation. Therefore, coping is necessary for patients with heart failure to cope with the stress in their life. Elderly patients with heart failure used adaptive coping strategies and emotion-focused coping strategies to cope with the illnesses in this study.
ACKNOWLEDGEMENTS
- The researchers express their deepest gratitude to the Head of Nursing Division, International Medical University (IMU), Associate Dean of IMU Research Laboratory, and Deputy Co-Chairman, IMU Joint-Committee on Research and Ethics for reviewing the research proposal and approving the research fund. The researchers are deeply indebted to the hospital management for granting permission to conduct pilot study and data collection, respectively. The participants are highly appreciated for their cooperation throughout this study. All the friends and family members of the researchers are greatly appreciated for their constant support throughout this project.