-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2015; 5(3): 110-121
doi:10.5923/j.nursing.20150503.04
The Effect of Birth Order and Socio Demographic Characteristics on Anxiety and Depression among Adolescents
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaaly Ibrahim Elalky1, Zenab Abed Elhaliem Othman2, Lamia Hassnin Eita3, Karema Ibrahim Eldemerdash4
1Assist. Prof. of Psychiatric and Mental Health Nursing, Faculty of Nursing, Minofya University, Egypt
2Prof. of Psychiatric and Mental Health Nursing, Faculty of Nursing, Cairo University, Egypt
3Lecturer of Psychiatric and Mental Health Nursing, Faculty of Nursing, Minofya University, Egypt
4Clinical instructor of Psychiatric and Mental Health Nursing, Faculty of Nursing, Minofya University, Egypt
Correspondence to: Lamia Hassnin Eita, Lecturer of Psychiatric and Mental Health Nursing, Faculty of Nursing, Minofya University, Egypt.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Birth order and socio demographic characteristics play a substantial role in individual life because the family is the first social system to which an individual is exposed. The aim of this studywas to assess the effect of birth order and socio demographic characteristics on anxiety and depression among adolescents. Design: descriptive correlational design was utilized. Setting: The study was conducted at two secondary schools at El-Batanoon, Shebin EL-Kom Menoufiya Governorate. Sample: convenience sample of all available adolescents from the two mentioned schools. Tools of data collection: (1) A semi – structured interview schedule to assess sociodemographic data, (2) Beck depression scale to assess depressive symptomsand (3) Taylor anxiety scale to assess anxiety. Results: The resultsrevealed that twenty three percent of the study adolescents have severe anxiety while a slightly more than half (53.25%) have mild depression. There is positively significance correlation coefficient between anxiety and depression. There is significant relation between socio demographic characteristics of study adolescents and both anxiety and depression. There is no statistically significant relation between adolescents’ birth order and their level of anxiety and depression. Conclusion: It was concluded thatthere is no relation between birth order and both anxiety and depressive symptoms while there is significant relation between socio demographic characteristics and both anxiety and depression among adolescents. Recommendation: An educational program for adolescents at schools should be provided to increase their awareness about the needs and problems of adolescents and how to satisfy their needs and adapt with their problems.
Keywords: Birth order, Anxiety, Depression, Adolescence
Cite this paper: Maaly Ibrahim Elalky, Zenab Abed Elhaliem Othman, Lamia Hassnin Eita, Karema Ibrahim Eldemerdash, The Effect of Birth Order and Socio Demographic Characteristics on Anxiety and Depression among Adolescents, International Journal of Nursing Science, Vol. 5 No. 3, 2015, pp. 110-121. doi: 10.5923/j.nursing.20150503.04.
Article Outline
1. Introduction
- Adolescence, a sensitive period marked with events such as puberty and identity crisis, on its own, can play a significant role in the development of an individual’s self-perception. Adolescence marks a period of not only dramatic hormonal and biological maturation, but social and identity manifestations tend to occur as well. Adjustment during adolescence can be challenging and unpredictable. With various factors such as family dynamics and intimate relationships, individuals may process adjustment in this stage differently from others. In fact, the family environment can be considered to be the initial setting in which adolescents are influenced to establish a unique family position and subsequently develop their personality based on that position in the family [1].The environment not only provides the basis and foundation of role development for adolescents, but it also shapes the initial and basic characteristics, by which adolescents seek to be identified within the family environment. Adolescents rely heavily on their family environment and interaction to shape and create their own unique personality because these are the initial stimuli to which adolescents are exposed. Adolescents tend to develop their own personalities, based on their roles in the home, which manifest into social roles. Additional external changes and factors, such as the birth of a new sibling or introduction of a step sibling that accompanies a second marriage, may also influence the actual or psychological birth role of an adolescent [2].Birth order is rather significant in different cultures all over the world. In some cultures the most preferred position was and still is the position of the eldest child. Some cultures consider the youngest child to be the dominant one. Different positions of birth order create certain differences between children belonging to this or that position. These differences explain why siblings are not alike. The birth order of a child is the predictor of his or her future characteristics. The true reason for such differences between and/or among siblings is the “fight for power”: the desire to control the situation, the desire to be different, to be individual, and to get the love of the parents [3]. Birth order is the chronological order of sibling births in a family.". Within the definition, birth order is classified into four main categories; first-born, middle-born, last-born and only children [4, 5].Each birth order comes with its own set of personality traits. Some children may possess all the traits while some others will only possess a few. First born children, after the birth of the second child, are left feeling inferior, questioning their position in the family, and desperately trying to gain back the attention they suddenly lost. First born children are known to be reliable, conscientious, cautious, controlling, and achieving. The middle child is competitive, making him/her entrepreneurs later in life. He/she tends to be more flexible than other members of the family, eager for parental praise, and develop musical or academic gifts. The second born described as people pleasers, somewhat rebellious, thrives on friendships, has large social circle, and a peacemaker. The last-born child is pampered throughout his childhood by all members of the family and grew-up trying to please his family members [6].Parental influence has a large impact on siblings' birth order and their characteristics that they will establish for themselves. The parents of the siblings are the final influence upon a sibling's depiction of his/her family and environment. Parents are the main providers of the interpersonal relationships and influence the roles that males and females play. In addition, "the difference in character, temperament and interest between the first and second child often seems to be based on inherited capacities, especially if each of the children appears to take after a different parent" [7].The nurse should help and encourage the parents to deal with their children effectively without causing any psychopathology as anxiety and depression through do not compare children, help them to find and develop their unique talents and skills, give them responsibilities appropriate to their age, do not give the oldest too much responsibility, make sure the middle child gets his/her share of positive attention, do not baby the youngest too much, praise the behaviors you want to encourage, help the only child to integrate with his peers, develop a working relationship with teachers, help children become independent and communicate with each child [8].
2. Significance of the Study
- Anxiety is one of the most common disorders among young people [9], and higher rates of anxiety disorders have been reported in adolescence relative to childhood. Anxiety is a psychological and physiological state characterized by somatic, emotional, cognitive, and behavioral components. It is the displeasing feeling of fear and concern [10]. Deardorff [11] mentioned that symptoms of anxiety in adolescents include feeling constantly agitated, a racing heart or sweating, seems very sensitive to criticism, always expects the worst to happen, avoids difficult situations and is withdrawn. There are some risk factors that might make a young person more vulnerable or sensitive to experience anxiety. These include genetic factors as a family history of mental health problems, environmental factors such as stress or a very stressful event in your child’s life, personality factors such as being very sensitive that may be due to birth order [12].Anxiety has a major effect on adolescents and makes them vulnerable to many problems such as substance abuse, academic problems, relationship problems with friends and family, physical problems and depression [13]. It is estimated that between 4 and 8 percent of adolescents are depressed. Depression is a serious medical problem that causes a persistent feeling of sadness and loss of interest in activities. It affects how an adolescent thinks, feels and behaves, and it can cause emotional, functional and physical problems. Adolescent's depression is not a weakness or something that can be overcome with willpower. It can have serious consequences and requires long-term treatment [14].Symptoms of adolescent depression include irritable mood, loss of interest in sports or activities, changes in appetite, excessive late-night activities, physical agitation or slowness, loss of energy, social withdrawal, making critical comments about themselves, behavioral problems at school or at home, overly sensitive to rejection, poor performance in school, frequent complaints of physical pain (headaches, stomach) and writing about death [15]. Psychological research has made additional discoveries about the psychological effect of birth order where it influences personalities and can lead later to psychiatric illness as depression, anxiety, obsessive-compulsive disorder and schizophrenia [16]. Studies have found that there are associations between birth order and various forms of psychopathology, including depression and anxiety [17].Each of the birth orders has its own feeling of anxiety and depression. These types of depression are based on hidden fear, sadness, shame, feeling stupid and loneliness. Because these feelings are hidden from themselves the birth orders experience them as depression. The only child learns to hide fear as a child. The child comes to believe that fear is unacceptable so it has to be hidden when it cannot be turned off. The fear goes into the subconscious where it becomes only child depression that keeps him/her from doing things .The first born learns to hide sadness as a child when the baby comes home. Losing mother’s attention to the baby makes the first born feels sad, a feeling he or she soon learns is unacceptable because the mother has to take care of the baby. Inability to turn the sadness of the first born makes him/her learns to hide the sadness not only from others but from self. The sadness goes into the subconscious where it becomes first born depression that keeps him/her from being happy [18].Children who sit in this middle position often feel that they are not as important as the first child, yet not as doted upon as the last. This perception may make children who sit in the middle more prone to depression and sadness. Many middle children feel as if their voice gets drowned out by the louder voice of the elder child within the family. This may lead the depressed middle child desperate for attention and cause him/her to act out in aggression or engage in negative behaviors as a method of seeking attention [19]. The birth order is considered an important factor among adolescents. It is an important tool in shaping how an adolescent turns out to be an adult. It determines how he sees the world, how he expects the world to treat him, and how he/she treats others. Thus, it is important to take birth order in adolescents seriously and do what to be done to prevent or stop the negative consequences from happening or getting worse.
3. Subjects and Method
3.1. The Aim of the Study
- The present study was carried out to assess the effect of birth order and socio demographic characteristics on anxiety and depression among adolescents.
3.2. Research Questions
- 1. What is the relationship between birth order and anxiety among adolescents? 2. What is the relationship between birth order and depression among adolescents?3. What is the relationship between socio demographic characteristics of adolescence and their level of anxiety and depression?4. What is the relation between parental style as it perceived by adolescences and their level of anxiety and depression?
3.3. Research Design
- A descriptive correlational design was utilized to achieve the aim of the study.
3.4. Setting
- This study was conducted in two secondary schools at El-Batanoon, Shebin EL-kom, Menoufyia Governorate, one school was for boys and the other was for girls secondary school.
3.5. Subjects
- Two secondary school students were randomly selected. Firstly, Shebin EL-kom city was selected randomly from a container containing names of all cities in Menoufyia Governorate, then El-Batanoon village was selected randomly from a container containing names of all villages in Shebin EL-kom city. The resulting selection is El-Batanoon village. El-Batanoon village contains two secondary schools, one school was for boys and the other was for girls. The sample size was a convenience sample of 400 out of 580 adolescence that were available from the two mentioned schools and fulfilling the following inclusion criteria: Acceptance to participate in the study, both sex, their age ranges from 15-18 years, first and second year of secondary school, free from any chronic physical and psychiatric illness, free from any history of substance abuse.
3.6. Tools for Data Collection
- Three tools were used to collect data for this study.Tool (1):- Structured interview schedule.The structured interview schedule sheet was developed by the investigator. It Includes items related to socio- demographic characteristics of the adolescents as age, gender, birth order, income, parental style, home atmosphere e.g. family size, income, family relationship, etc as perceived by adolescents.Tool (2):- Soueif and El Sayed's depression scale:This scale was originally developed by Beck et al, [20] as a screening technique for measuring the symptoms of depression. It was translated into Arabic and tested for its validity and reliability by Soueif and El Sayed [21]. It consists of 21 items, each item is categorized in 4 to 5 levels of intensity of symptoms and the person is asked to estimate at which level he is. The scoring system is categorized as follows:-21-29 not present, 30-44 mild, 45-69 moderate, 70-105 severe. Tool (3):- Taylor anxiety scale:This scale was developed by Taylor [22] and used to measure the severity of anxiety symptomatology. It consists of 50 yes/no questions. This scale was translated into Arabic and tested for its content validity and reliability by the investigator. The scoring system is categorized as follows: (17-19) mild anxiety, (20-24) moderate anxiety, (25-29) above moderate, (30-34) severe anxiety, (35-50) very severe anxiety.
3.7. Methods
- Preparation:This phase included reviewing the relevant literature and different studies related to the topic of research, using text books, article magazines, periodicals, and internet research was conducted to get clear picture of all the aspects related to the research topic.
3.8. Content Validity
- Before starting, the data collection tools were translated into Arabic and tested for their content validity by group of experts in the psychiatric medicine and nursing staff to check the relevance, coverage of the content and clarity of the questions. The required modifications were carried out accordingly.
3.9. Reliability
- Test- retest reliability was applied. The anxiety scale proved to be reliable at 0.82 while depression scale proved to be reliable at 0.91.
4. Pilot Study
- A pilot study was undertaken after the development to the tools and before starting the data collection. It was conducted on (40) secondary school students using tools (1), (2), (3). The purpose of the pilot study was to test the applicability, feasibility and clarity of the tools. In addition, it served to estimate the approximate time required for interviewing the students as well as to find out any problems that might interfere with data collection. After obtaining the result of the pilot study, the necessary modifications of tools as (excluded questions, added questions & revised) were done then the final format was developed. These students were excluded later from the main study sample.
5. Procedure of Data Collection
- Before starting any step in the study, an official letter was addressed from the faculty of nursing, Menoufiya University to the director of the secondary schools of El-Batanoon and El- Mosher El-Gamsy School, requesting their cooperation and permission to conduct the study. Once the official permissions was obtained from the principal and the other authorized personnel from the various settings the researcher started the data collection. All of the authorized personnel were provided by the needed information about the study from the researcher. All students fit to the inclusion criteria were approached by the investigator to fill in the questionnaires according to the following steps: The investigator started data collection by introducing herself to the participant. Oral informed consent was obtained from each participant. Then brief description of the purpose of the study and the type of questionnaire required to fill was given to each participant. Data collected were done through interviewing with the students at classroom. The researcher started to collect the data from students two days/ per week for each school from 15 to 20 student \ day. Each interview lasted for 15-20 minutes, depending on the response of interview. The process of data collection took a period of 3 months.
6. Ethical Considerations
- An oral consent was taken from each student in the study after explaining the purpose and the importance of the study. The subjects who agreed to participate in the study were assured about confidentiality and anonymity of the study. They were informed about their right to withdraw from the study at any time without giving a reason.
7. Statistical Analysis
- Data entry and statistical analysis were done using the statistical package for social sciences (SPSS version 21). Data were presented using descriptive statistics in the form of frequencies and percentages for qualitative variables, and mean and standard deviation for quantitative variables. Qualitative variables were compared using chi-square test and correlation coefficient is used to measure the direction and strength of the correlation between variables. A significant level value was considered when P-value <0.05 and highly significant level value was considered when P value < 0.001 while P value of >0.05 indicated non-significant.
8. Results
- Socio-demographic characteristics of the study adolescents (n=400): The results revealed that half of the study adolescents were males and the mean age was 16.1±0.55. Three quarters of the study adolescents (74.8%) are first year students, the majority of adolescent (96.8%) live at villages. The majority of them (90.7%) live with both parents.Figure (1): Birth order of study adolescentsThis figure reveals that more than one third of studied adolescents (36%) are in middle birth order students while only 1% is alone.
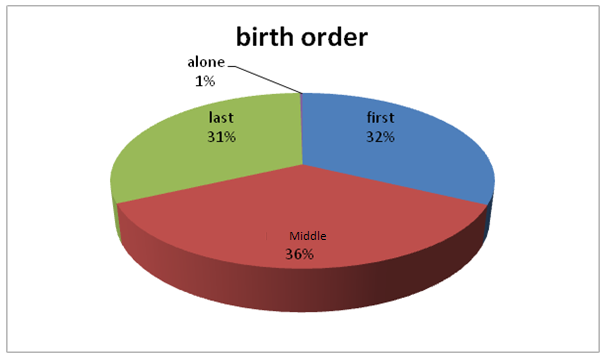 | Figure (1). Birth order of study adolescents |
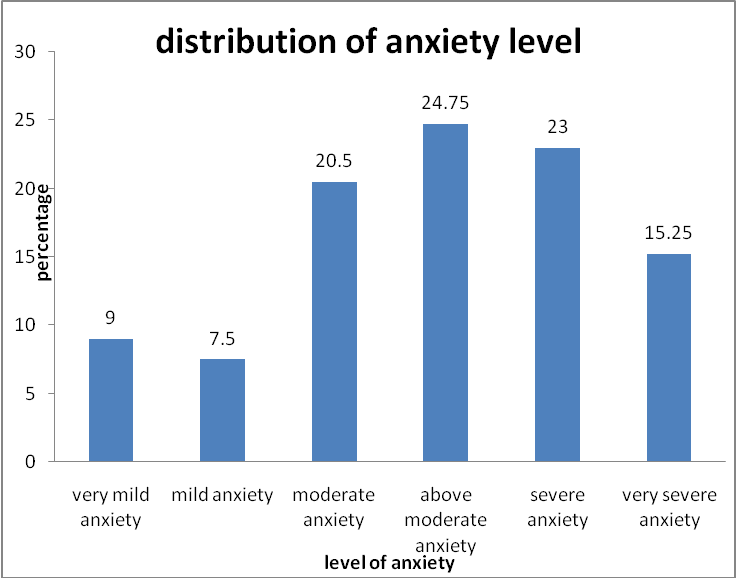 | Figure (2). Level of anxiety among the study adolescents |
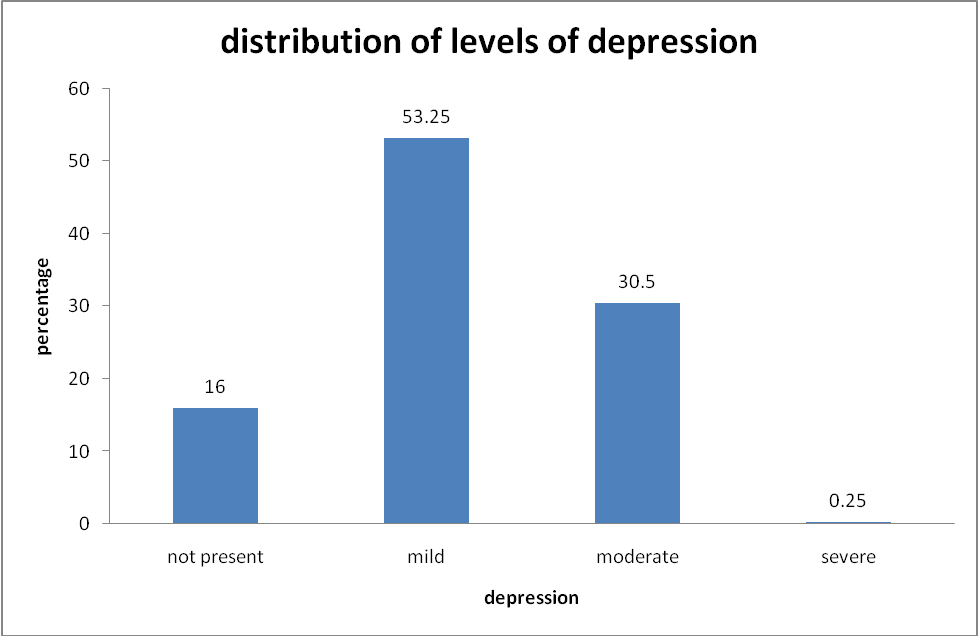 | Figure (3). Level of depression among the study adolescents |
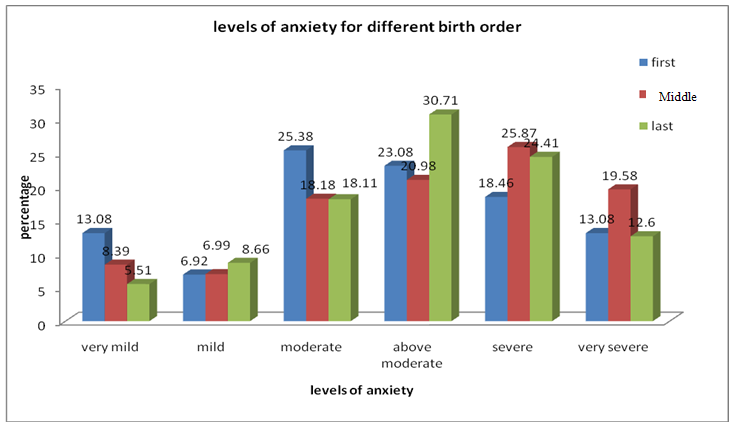 | Figure (4). Anxiety levels among the study adolescents’ according to their birth order |
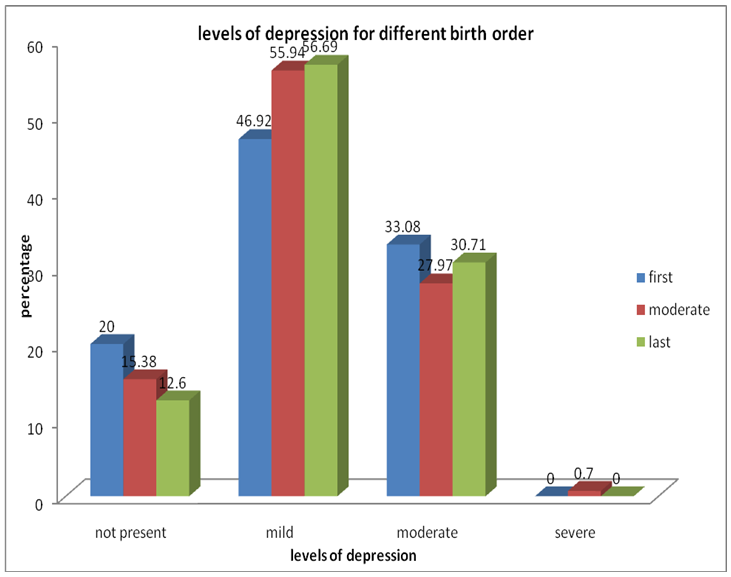 | Figure (5). Levels of depression among the study adolescents’ according to their birth order |
|
|
|
|
|
9. Discussion
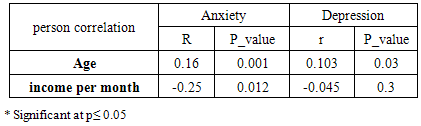
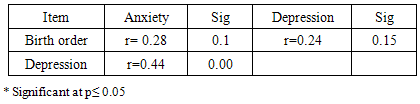
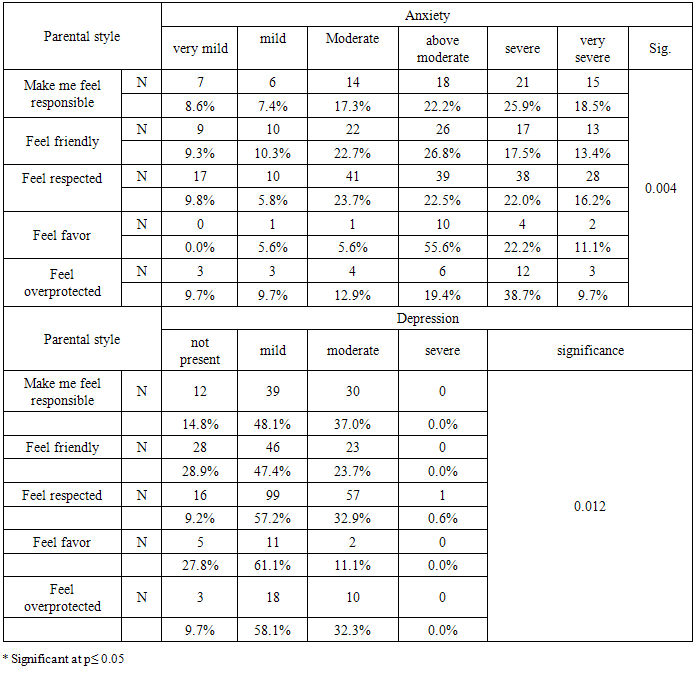
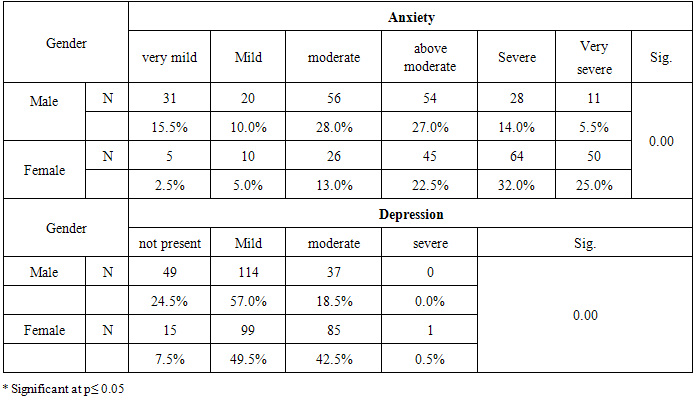
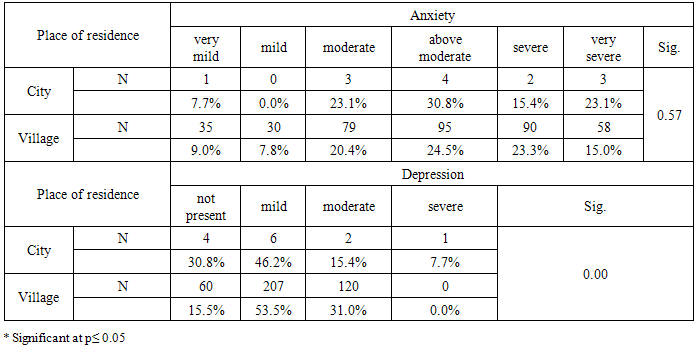
- Being different is something everyone wants to be. Each person wants to have a unique trait that makes him/her diverse. Labeling a person, such as, “the quiet one”, “the rebel”, or “the wise one”, describes the personality traits one may obtain. Research has showed that birth order may possibly have a connection to personality. Alfred Adler believed that people’s birth order was one of the most important factors in their life and that the position they have had in the family was one of the best predictors of the kind of person they would become. The only child has a need to be the focal point, the eldest takes on the role of a surrogate parent, and the youngest takes pleasure in being the baby of the family [23]. Therefore, this study aimed at assessing the effect of birth order on anxiety and depression among adolescents.The current study reveals that almost two third of the study adolescents have severe anxiety. This result was consistent with Dalbudak [24] who reported that most of his study adolescences have higher scores of anxiety. Also Lotf [25] who found in his study that the majority of study adolescents have severs anxiety. This might be because of the beginning of puberty or the social pressures put on them, for example, romantic relationships and pressure to be "popular". The current study showed that more than half of the students have mild depression and about one third have moderate depression. This result was inconsistent with the study of Kaltiala-Heino et al., [26] who found in his study that 17.2% of students have mild depression. This might be due to the monotony of the style of education in Egypt which negatively influences the students' psychological status, or could be due to parental style difference or culture differences. The current study showed that there was a positively significance correlation coefficient between anxiety and depression. This result was on the same line with the study of Alansari [27] who reported that the depressive scores are significantly correlated with the anxiety scores on linear regression.The current study showed that more than one third of the study sample was in middle birth order. This result was on the same line with the study of Vahid [28] who found that (16.8%) of his study sample was the only child, (28.6%) were first child, (34.2% ) were second child and ( 20%) were third child or later.The current study showed that there is no statistically significant correlation between birth order and both anxiety and depression. This result was inconsistent with Risal and Tharuur [29] who stated that there are associations between birth order and various forms of psychopathology including anxiety and depression. The present study revealed that the middle birth order position adolescents have higher anxiety level than first and last one. This result was supported by Leun and Justine [30] who stated that middle child feels that the world pay less attention to him/her, may not feel they have special place in the family and feel more anxiety. This is contraindicated with the study of Puri [31] and Tramontana [32] who found that first born student had more anxiety than later porn student. This could be due to parents tending to see more of themselves in their first child and therefore project their own aspiration on to them. The pressure put on eldest children would be the most likely source of anxiety for first born one. The current study showed that slightly more than one third (33.08%) of first birth order students are in contrast to (27.97%) of middle birth order students how have moderate depression. This result was supported by the study of Isaacson [18] who reported that losing mother's attention to the baby makes the first born feel sad; feel he is unacceptable because mother has to take care of the new baby. The sadness goes into the subconscious where it becomes first born depression. This result was contraindicated with the study of Schreiner and Media [19] who reported that children who are in middle position often feel that they are not as important as the first child, yet not as doted upon as the last. This perception may make children who sit in the middle more prone to depression and sadness. This might be due to the fact that in village the parents delegate more responsibility on the first child which may lead him to feel burdened and sad. The result of the current study showed that the mean age was 16.1± 0.55 and there is highly positive statistically significant correlation coefficient between a student's age and his level of depression and also level of anxiety. This result was supported by Crowe et al., [33] who reported that the prevalence of depression rises gradually with age and pubertal development. This might be because of the start of puberty or the social pressures put on adolescence, for example, romantic relationships and pressure to be "popular". This result was contradicted by a study performed by Mores and Takau [34] who found that there was no significant relationship between age and anxiety among adolescents. This might be due to differences in culture, parental style and style of education.The current study showed that there is a highly statistically significant difference between parental style and students' level of anxiety and also level of depression. This result was supported by Healey and Ellis [35] who reported that there is a significant association between parental style, anxiety and depression. The current study showed that there is highly statistically significant difference between gender and level of anxiety. This result was supported by Reese-weber and Khan [36] who concluded that girls have a higher tendency to acquire psychological disorder as anxiety than boys. Also, this was on the same line with the study of Angold et al., [37] who reported that higher depressive and anxiety symptom levels in female adolescents as compared to males from adolescence onward and generally stable or decreasing symptom development for boys, and increases for girls. This result is contraindicated with the study of Faleye [38] and study of Oludipe [39] who found that there is no significant difference in anxiety level between male and female adolescents. This might be due to females might have a genetic or biological predisposition in developing internalizing disorders or the sex differences in anxiety and depressive disorders are linked to differences in the experiences and social roles that males and females endure.The current study showed that there is highly statistically significant difference between gender and level of depression. This result was supported by study of Fröjd et al., [40] who found that the rate of depression was found to be 18.4% among girls and 11.1% among boys. It was also supported by Kessler et al., [41] who found that depression is more common among females (21%) than males (13%). Kaltiala-Heino et al., [42] also found that the prevalence rate of mild depression among girls was found to be 11.2% and 5.9% among boys. Moderate depression was found to be 9.0% among girls and 4.7% among boys, while severe depression among girls and boys were found to be 2.1% and 1.5%, respectively. This might be due to poor social support from the community, culture in rural areas, decrease of recreational areas in villages, adverse experiences in childhood, sociocultural roles with related adverse experiences, and psychological attributes related to vulnerability to adverse life events and coping skills are likely to be involved. Genetic and biological factors also might be due to women are much more prone to diagnosing themselves as depressed, or reaching out for help. Women in village have less freedom than men do, and cannot always do as they please. This might cause an increased need for emotional support that if women do not get, they feel depressed. Furthermore, women have higher chance of depression right after childbirth. This has been explained socially by the fact that after childbirth women realize that they cannot aspire to do anything else, but care for their children. The current study showed that there is a highly statistically significant negative correlation between family income and students' level of anxiety while there is no statistically significant corelation between family income and students' level of depression. This result was contradicted by the study of Fleitlich-Bilyk and Goodman [43] who reported that higher rates of depression in adolescents were among low-income and middle income. It was also contradicted by the study of Pine et al., [44] who reported that there was association between depression and environmental factors such as exposures to acute stressful events as personal injury, bereavement and poverty. This might be due to the fact that in village, the income is not appropriate with the student's needs as a result of poverty so it leads to anxiety. Also, in village the people are more religiously and satisfied with simple living which protect them from gaining depression.The current study showed that there was no statistically significant difference between the place of residence and students' level of anxiety while there is highly statistically significant difference between place of residence and students' level of depression. This might be due to the fact that in rural areas there are no recreational areas and the culture in the rural areas is so restricted and controlled by rigid discipline than the culture in the urban areas.The current study showed that there was a highly statistically significant difference between parental style and students' level of depression. This result was supported by the study of Pargas et al., [45] who reported that children and adolescents with a high familial risk of depression tend to have better mental health if their relationships with their parents are characterized by warmth, acceptance, low hostility, and low parental control. This result was also supported by the study of Restifo and Bogells [46] who reported that negative family relationships especially through mother is a common risk for depression. The current study showed that there were statistically significant differences between parental style and students' level of anxiety. This result was supported by the study of Seif El Din, Okasha and Maj [47], Eckstein et al., [48] who reported that bad home atmosphere which includes lack of communication within the family, presence of child-parent conflict, parental conflicts and parental separation rather than death ranked the highest among predisposing factors in the Egyptian adolescents who demonstrated moderate anxiety on Taylor anxiety scale.
10. Conclusions
- It can be concluded that more than one third of students had severe anxiety symptoms and one third of them had moderate depression symptoms. There is significant relation between anxiety and socio demographic characteristics of study adolescents as age, gender, income and their perceived parental style. There is significant relation between depression and socio demographic characteristics of study adolescents as age, gender, place of residence and their perceived parental style. There is a positively significant correlation between depression and anxiety while no significant correlation between birth order and both anxiety sand depressive symptoms among adolescents.
11. Recommendations
- Based on the findings of the present study, the following recommendations are suggested:1- Continuous assessment, screening and discovery should be done for all adolescents to determine the high risk for any psychological problems. 2- Support, counseling and appropriate referral should be provided to adolescents who have any psychological problems. 3- Providing an educational program for adolescents at school to help them understand their normal growth and development and how to adjust with this stage and increase their ability to interact with other and constructively express their needs and problems.4- Providing an educational program for parents of adolescents helps them increase their awareness about the needs and problems of their adolescents, how to adjust with their problems and ways of effective parental strategies to minimize adolescences psychological problems.
ACKNOWLEDGEMENTS
- First of all, deepest thanks go to "Allah" for giving us the power to complete this work. Also, gratitude is extended to all volunteers who participate in this study. Respect goes to all those who assisted us in accomplishing this work.
Suggested Further Study
- Further psychological research should be focused on the gender influence on a child's birth order and how this affects development and a child's future.