-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2013; 3(2): 45-50
doi:10.5923/j.nursing.20130302.03
Predictors of Moral Distress among Jordanian Critical Care Nurses
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRabia Allari1, Fathieh Abu-Moghli2
1Al-Isra University, Faculty of Nursing, B.O. Box 11622, Elmatar Street, Amman, Jordan
2The University of Jordan, Faculty of Nursing, Amman, Jordan
Correspondence to: Rabia Allari, Al-Isra University, Faculty of Nursing, B.O. Box 11622, Elmatar Street, Amman, Jordan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Many research studies suggested that moral distress is associated with perceptions of ethical climate and is influenced by demographic variables. This study aimed to examine the ability of selected demographics and variables related to perception of hospital ethical climate in predicting the level of moral distress among critical care nurses in Jordan. A descriptive, correlation design was used in this study. Moral Distress Scale, Hospital Ethical Climate Scale and a demographic data form were administered to a random sample of 150 critical care nurses at 12 hospitals in Jordan. Data were analyzed using descriptive and inferential statistics.Factors constituting the hospital ethical climate and demographic characteristics revealed no ability to predict moral distress. However, moral distress was found to be a common encounter among Jordanian nurses though they are not familiar with the term which implies that solutions to relieve their distress are unexplored. But still the result has a clinical merit that may help in establishing implications and recommendations of further researches. The findings of this study may assist hospitals and nurse managers in identifying factors contributing to moral distress from the nurses' perspective, and assist in planning and implementing strategies to reduce moral distress among nurses in critical care units and consequently improving the quality of care.
Keywords: Moral Distress, Critical Care Nurses, Hospital Ethical Environment
Cite this paper: Rabia Allari, Fathieh Abu-Moghli, Predictors of Moral Distress among Jordanian Critical Care Nurses, International Journal of Nursing Science, Vol. 3 No. 2, 2013, pp. 45-50. doi: 10.5923/j.nursing.20130302.03.
Article Outline
1. Introduction
- Today's acute care environment presents nurses with difficult situations and ethical dilemmas that may lead them to experience moral distress. The changes in health care delivery models, new technological advances and the emotionally charged environment of the critical care units add to the complexity of the situation[1, 2]. The complexity and frequency of ethical dilemmas are the major determinants of the intensity of moral distress. Ethical dilemmas encountered by the nurses working in critical care units greatly exceed those encountered by nurses working in other acute care settings leading to more ethical distress[3].Moral distress is a phenomenon of increasing concern in nursing practice, education and research[4]. It constitutes a significant cause of emotional suffering among nurses that may result in unfavorable outcomes for both nurses and patients. Feelings labeled as stress, emotional exhaustion, and job dissatisfaction may actually be indicative of moral distress. The experience of moral distress leads to frustration, depression and absenteeism that jeopardize nursing care. These symptoms may be the reason given by nurses for leaving a specific work environment or even for departure from the nursing profession[2]. Research to date suggests that the ethical climatecontributes to moral distress, nurses’ decreasing job satisfaction, attrition and unsafe patient care[2, 5]. Perception of the ethical climate of one’s workplace is based on the relationships with peers, patients, managers, physicians, and hospital administration when encountering ethical problems [6]. These relationships, according to Olson, are influenced by many conditions such as varying levels of power, trust, inclusion, role flexibility, and inquiry that is necessary for ethical problem-solving[7]. Pauly reported that peers, physician, and hospital management In addition to patients and nursing mangers were predictors for moral distress among nurses[8].In addition to the hospital ethical climate, demographic variables of gender, education, ethics education, and work experience were listed as potentially having significant correlation and prediction of the experience of moral distress[6, 9, 10]. Conversely, many other studies found no correlation between demographic characteristics such as gender, education, age and years of experience[4, 9, 11-13]. Elpern reported that, except for the years of nursing experience in nursing, all individual characteristics, were positively correlated with the level of moral distress[2]. According to Meltzer and Huckabay nurses' age was found to be a significant predictor of emotional stress as younger nurses appeared to have somewhat more feelings of depersonalization than did older nurses. Furthermore, Meltzer and Huckabay reported a significant negative relationship between educational level and moral distress[1]. In another study done by Allari & Abu-Moghli in Jordan (2011) to describe nurses’ level of moral distress, their perception of the hospital ethical climate, and the relationship between their level of moral distress, the results showed that total moral distress and the two subscales Intensity and Frequency had moderate mean[14].When more specifically looking at the intensity subscale of the MDS in the same study, the situations that were considered the highest in intensity in causing moral distress were those related to the “suffering often seen in patients with complex, life threatening illnesses”. Also the top five items with the highest total distress scores were related to the “end of life issues”. The item regarding "Continue to participate in care for a hopelessly injured person who is being sustained on a ventilator, when no one will make a decision to turn off the life support machine." had the first place for the Total Subscale scores[14]. This study aims at examining the ability of selected demographic (age, gender, education, years of professional experience, and employment years in the same hospital) and variables related to the nurses perception of hospital ethical climate (peers, patients, managers, hospitals administration, and physicians) in predicting the level of moral distress among critical care nurses in Jordan. The findings of this study may assist hospitals and nurse managers in identifying factors contributing to moral distress from the nurses' perspective and in planning and implementing strategies to reduce moral distress among nurses in general and critical care nurses in particular.
2. Methods
2.1. Study Design
- A quantitative descriptive design was used to examine the predictors of moral distress among critical care nurses in Jordan.
2.2. Sample & Setting
- This study was conducted in critical care units in public and private hospitals in Jordan. Only hospitals with bed capacity of 150 beds or more (N=12) were selected to ensure the availability of nurses in critical care units. The stratified disproportional random sampling of (150) participants were selected. Inclusion Criteria were being a Jordanian registered nurse with a minimum a BSC degree; working in a critical care unit; and working in the current institution for at least six months.
2.3. Ethical Considerations
- Approval for conducting the study was obtained from the ethical committee at the University of Jordan, the Ministry of Health (MOH), and the selected hospitals. The selected nurses were informed that participation is voluntary, that they can withdraw from this study at any time without penalty, not to write the names to ensure anonymity, and that the completion of the questionnaire is considered as a written consent for participation.
2.4. Study Instrument & Data Collection
- The study instrument includes two self-administered Likert-type scale questionnaires; The DDS was developed by the researcher based on a review of the literature. Demographic data included gender, age, education, and experience as registered nurses, and length of current employment. The Moral Distress Scale (MDS) was developed by Corley (1995) to assess the nurses' level of moral distress. The MDS is a 38-item scale measuring moral distress intensity and frequency. Two 6-point Likert scales are included in front of each statement to assess the level of moral distress in terms of intensity (ranging from ‘none’ to ‘great extent’) and frequency (ranging from ‘none’ to ‘very frequently’). The Hospital Ethical Climate Scale (HECS) was developed by Olson (1998) to assess nurses' perception of hospital ethical climate (HEC). The HECS is a 26-item self-administered survey that asks participants to rate their responses using a 5-point Likert scale ranging from 1 to 5 (1 = almost never true to 5 = almost always true). The items of the HECS are included under five subheadings including relationships with peers, patients, managers, hospital administrators, and physicians.The questionnaires were pilot tested to determine their cultural appropriateness, clarity and the time needed to be completed. Meetings with the nursing managers in all 12 selected hospitals were conducted to inform them about the study and to gain their cooperation. Each selected nurse was met in person, received an explanation of the purpose of the study and a copy of the questionnaires, accompanied with an envelope and a cover letter attached to each envelope, these envelopes were recollected by the researcher after one to two weeks period or upon nurses' requests. Data were collection was completed over a 10 week time period.Coded information from the instrument was entered into data files using Statistical Package for the Social Sciences Version 17.0 (2007). All statistical procedures were performed at α=0.05 (2-tailed statistics). Descriptive statistics including means, standard deviations, and actual ranges were reported for the following study variables including: age, years of professional experience, variables related to HECS (peers, patients, physicians, managers, and hospital administrators). Inferential analyses including regression analysis procedure was used to answer the study question. Since the regression analysis is used to model the value of a dependent scale variables based on its relationship to one or more predictors, multiple regression analysis was used to estimate the probability of recorded variables including sample demographics namely: age, gender, education, years of experience, employment years in the same hospital and the total hospital ethical climate score, and the factors related to hospital ethical climate (peers, patients, physicians, managers, and hospital administrators) to predict moral distress level, moral distress intensity, and moral distress frequency. Enter method was used to introduce predictors in regression model, and stepping method criteria was set using probability of F entry 0.05 and removal 0.1. Gender and educational level were dummy coded (0.1) for the purpose of running multiple regression as they are at nominal level. In addition, different entry methods of regression, different values of entry and removal of predictors, and examination of colinearity, skewness, and extreme variables were conducted to elucidate valid reliable results. For the same purpose, assumptions in regard to correlation and regression were also checked again including recorded variables. Multicollinearity was also examined and reported through the final regression analysis model.
3. Results
3.1. Characteristics of the Sample
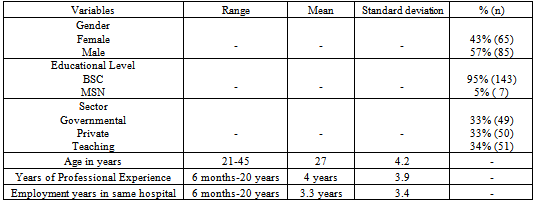
- Table (1) shows that of the sample (N=150), male and female participants were comparable with a mean age of 27 years old (SD=4.5, R=21-45). The majority of participants hold a Bachelor degree (n=143, 95%). Furthermore, participant of this study had an average of 4 years experience as registered nurses, and average of 3.3 years of employment in the same hospital.
3.2. Predictors of Moral Distress
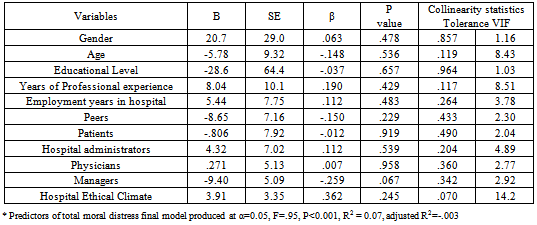
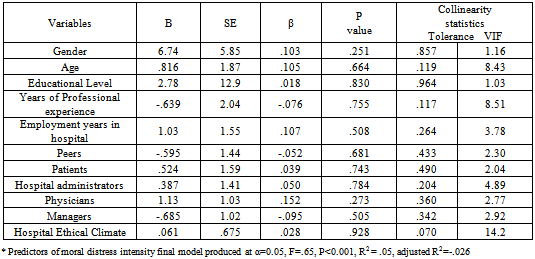
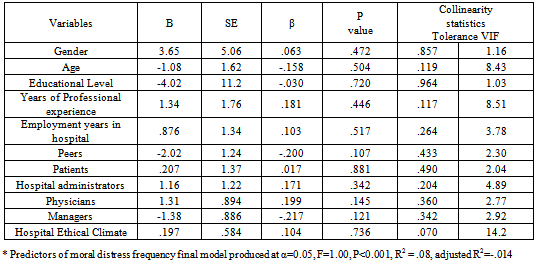
- Tables (2), (3), and (4) show multiple regression analysis of predictors of total moral distress, moral distress intensity, and moral distress frequency. The results in table (2) indicate that none of the variables has prediction performance of total moral distress among critical care nurses and the prediction performance was (F=.95, P<0.001, R2 = 0.07, adjusted R2=-.003). Similar results were shown in tables (3, and 4), poor prediction performance of moral distress intensity and moral distress frequency (F=.65, P<0.001, R2 = .05, adjusted R2=-.026, and F=1.00, P<0.001, R2=.08, adjusted R2=-.014).These results indicate that these variables including: demographic (age, gender, education, years of experience, & employment years in same hospital) and variables related to hospital ethical climate(peers, patients, physicians, managers, & hospital administrators) were having no statistically significant prediction performance in relation to moral distress, however, they may retain a clinically significant performance on nurses' perception of moral distress at critical care settings as proposed in the current study framework. And it is worthy to mention that there were no differences in the results between hospitals from all three sectors.
|
|
|
|
4. Discussion
- None of the demographic variables including (age, gender, years of professional experience, education, andemployment years in the same hospital) were able to predict moral distress, moral distress intensity, and frequency. While several studies reported that Moral distress was influenced by nurses’ educational levels, Meltzer and Huckabay reported that, in their study, nurses with a bachelor’s degree reflected significantly higher feelings of moral distress when witnessing futile care felt unable to provide adequate care[1].Similarly, lacks of knowledge of other treatment options or inexperience were found to be influential on nurses’ perception and response to otherwise unethical decisions or plans[15].In spite the fact that many studies indicated moderate ability of the hospital ethical climate to predict the presence of moral distress[4, 8, 16], the results of the current study indicated that the participants' perception of hospital ethical climate and its' five components s including: peers, patients, physicians, mangers, and hospital administrators were unable to predict the moral distress, intensity, and frequency at Jordanian critical care settings. Although the predictors including (demographics, total HECS, & variables related to HECS) were controlled in two stages: 1) the prediction performance within the moral distress in general and 2) the prediction performance when demographic variables are covariates; there was no prediction performance reported for all recorded variables and moral distress, moral intensity and frequency. Thus, there should be other factors beyond the researcher’s vision of the current study as represented and proposed through the framework, which may lay behind retaining the prediction performance of moral distress among critical care nurses. Despite the fact that the current study didn't show statistically significant prediction results, it has a clinical merit that may help in establishing implications and recommendations of further research venue.
5. Study Limitations
- Generalization should be cautionly considered. Despite the assurance of anonymity of all participants, potential socially desirable responses may have affected the results because of the nature of this study. A limitation of this study, as in previous research that has attempted to measure moral distress, is that the MDS draws on Jameton’s definition of moral distress with an emphasis on the inability of nurses to act due to institutional constraints rather than as a function of an inability to balance between individual and contextual constraints on moral action[17]. On the other hand, as the first study that investigated issues related to moral distress and hospital ethical climate in Jordan, the findings provide a foundation for the development of evidence-based interventions, designed to improve the nursing profession. Data in the current study point to the importance of moral distress and the ethical climate in ICUs as variables worthy of further investigation.The nature and extent to which organizational factors contribute to moral distress require further attention in research. Given that some researchers have shown that nurses leave their positions because of moral distress, there is a particular need to focus on the relationships among moral distress, intension to stay, recruitment, and retention. In addition, focusing on the role of hospital ethical climate as a mediating factor between moral distress and decisions to leave nursing is exceptionally needed by both quantitative and qualitative research for better understanding of these phenomena. Fruitful areas for future research include exploring also the situations giving rise to moral distress which pertained to the nurses' work environment are acknowledged.
6. Conclusions
- This study has revealed that moral distress is a common encounter among nurses, regardless of age, gender, work experience, years of experience, or own perception of hospital ethical environment, though they are not familiar with the term which implies that solutions to relieve their distress are unexplored. It is suggested, therefore, that ethics and ethical decision making be included as an integral part of all nursing curricula. A forum also needs to be founded to facilitate sharing of nurses' moral concerns and experiences of moral distress, as well as encouraging nurses to voice these concerns to physicians, patients, and families. This would serve to augment nurses' coping abilities and support them in their role as moral agent. Education may be included in this setting, if necessary, to allow for a common language for nurses to discuss moral issues with clarity and understanding.Based on the results and conclusions of the present study, it is recommended that: Further studies should be conducted addressing other variables than hospital ethical climate as a predictor of moral distress, different study designs, considering larger sample size, and other areas of specialization. Furthermore, Communication between professionals in health care organizations should be studied using both quantitative and qualitative approaches. Emphasis needs to be on partnership in ethical decision making that related to patients in critical care units. An analysis of moral agency in relation to organizational structures is required in order to enhance our understanding of moral distress in nursing practice and the possibilities for improving care. Examining the nature of moral distress in relation to the ethical climate has potential benefits for both nurses and patients. So the exploring the extent to which organizational factors contribute to moral distress requires further attention in research. Given the current and future shortages of registered nurses, attention to moral distress and the development of positive ethical climates is of paramount importance to the evolution of quality work environments and quality patient outcomes.
ACKNOWLEDGEMENTS
- The authors gratefully acknowledge funding from Deanship of Scientific research in the University of Jordan. Thanks also to Dr. Linda L. Olson & Dr. Mary Corley, for sharing their instruments. Also special thanks to Dr. Mohammad Nassar who provided assistance with statistical analysis of this study.