-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Nursing Science
p-ISSN: 2167-7441 e-ISSN: 2167-745X
2013; 3(1): 1-6
doi:10.5923/j.nursing.20130301.01
Assessments of Adherence to Hypertension Medications and Associated Factors among Patients Attending Tikur Anbessa Specialized Hospital Renal Unit, Addis Ababa, Ethiopia 2012
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHabtamu Abera Hareri1, Mesfin Abebe2
1Department of Nursing, College of Health sciences, Debre Markos University
2Department of Nursing, College of Health Sciences, Addis Ababa University
Correspondence to: Habtamu Abera Hareri, Department of Nursing, College of Health sciences, Debre Markos University.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Hypertension is one of the most important preventable causes of premature mortality worldwide and it is one of the primary risk factors for heart disease and stroke.In Ethiopia 10.6% and Addis Ababa, 30% of the population has been estimated to have hypertension. Adherence to medication therapy is an aspect of patients’ care that is often overlooked and should be evaluated as a crucial part of cardiovascular management. Institutional based cross-sectional study was conducted. Systematic sampling technique was used to select 286 study subjects. A structured standard interviewer administered questionnaire was used after some modifications and analysis was done using SPSS 16. P-value <0.05 was considered significant association. Scoring method was used to classify patients’ level of adherence. Of 286 subjects included in the study 165(57.7%) were female and mean age was 52±13 year. The adherence level of respondents to medication was 69.2%. The medication adherence was found to be better in patients who had been informed about their medicine. There was significant association between marital status, work status, Health care facilities, duration of Hypertension and its treatment and medication adherence. The rate of adherence to medication was generally found to be low in these study participants.
Keywords: Hypertension, Adherence Status, Medication, Perception
Cite this paper: Habtamu Abera Hareri, Mesfin Abebe, Assessments of Adherence to Hypertension Medications and Associated Factors among Patients Attending Tikur Anbessa Specialized Hospital Renal Unit, Addis Ababa, Ethiopia 2012, International Journal of Nursing Science, Vol. 3 No. 1, 2013, pp. 1-6. doi: 10.5923/j.nursing.20130301.01.
Article Outline
1. Introduction
- Hypertension is an overwhelming global challenge with high morbidity and mortality rate. Analysis of the global burden of hypertension revealed that over 25% of the world's adult population had hypertension in 2000, and the proportion is expected to increase to 29% by 2025. The prevention and control of high blood pressure has not received due attention in many developing countries. Adherence to therapies is a primary determinant of treatment success. Poor adherence attenuates optimum clinical benefits and therefore reduces the overall effectiveness of health systems 1, 2, 4Despite its importance, adherence to medication therapy is an aspect of patients’ care that is often overlooked and should be reevaluated as a crucial part of cardiovascular management. Although reliable, large-scale,population-based data on high blood pressure in SSA are limited, recent studies provide important and worrisome findings in both epidemiology and clinical outcomes. Although overall hypertension prevalence is between 10%-15%, prevalence rates as high as 30%-32% have been reported in middle-income countries. Importantly, hypertension awareness, treatment, and control rates as low as 20%, 10%, and 1%, respectively have also been found. Rapid urbanization and transition from agrarian life to the wage-earning economy of city life continue to fuel increases in average blood pressure levels and prevalence of HTN 2, 3.The epidemiology of high blood pressure among adults in Addis Ababa was studied. About 20% of males and 38% of females were overweight, with 10.8 % of the females being obese. Similarly, 17% of the males and 31% of the females were classified as having low level of total physical activity. Reported use of anti-hypertensive medication, was 31.5% among males and 28.9% among females. High blood pressure is widely prevalent in AA and may represent a silent epidemic in this population. In Africa, 15% of the population has hypertension. Although there is shortage of extensive data, 6% of the Ethiopian population has been estimated to have HTN. Approximately 30% of adults in Addis Ababa have hypertension above 140/90mmHg or reported use of anti-hypertensive medication This indicates an urgent need for strategies and programmes to prevent and control high blood pressure, and promote healthy lifestyle behaviors primarily among the urban populations of Ethiopia1,4.A WHO report estimates that adherence to antihypertensive medications ranges from 52% to 74% when adherence is defined as possession of a medication at least 80% of the time. It also identified non adherence to medical treatment as a major public health concern, especially in patients with chronic conditions, e.g. hypertension. It is now evident from WHO data that coronary heart disease and cerebrovascular disease are increasing so rapidly that they will rank Number one and five respectively as causes of global burden by the year 2020. In Africa only 5-10% have a blood pressure control of hypertension of<140/90 mm Hg5, 6. The number of adults with hypertension in 2025 was predicted to increase by about 60% to a total of 1.56 billion. According to the WHO, more than 80% of deaths from hypertension and associated cardiovascular diseases now occur in low and middle-income countries and this is particularly common among people of low socio-economic status7,8. In spite of many advances made in adherence research, non-adherence rates have remained nearly unchanged in the last decades. Poor adherence is associated with bad outcome of the disease and wastage of healthcare resources 1, 9
2. Objective
- The objective of this study was to assess adherence and associated factors of adherence to medication among hypertensive patients attending Tikur Anbessa Specialized Hospital renal unit, Addis Ababa, Ethiopia 2012.
3. Methods
- The study was conducted in Tikur Anbessa specialized Hospital renal unit in Addis Ababa, Ethiopia. Based on the 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), Addis Ababa city has a total population of 3,384,569. It lies at an altitude of 7,546 feet (2,300 meters). The area was selected because it is central referral hospital that provides organized hypertension follows up care. The study period was from September 2011 to May 2012. A cross-sectional study design was conducted in Tikur Anbessa specialized Hospital renal unit. Source population was all hypertensive patients during the study period. Study subjects were all HTN patients who fulfilled the inclusion criteria
3.1. Sampling and Sample Size
- Study was carried on total of 1700 patients attending Tikur Anbessa Specialized hospital. Out of this 286 were selected by systematic random technique down the list. The first study subject was selected by simple random technique using lottery method. Every other two patients were interviewed when they came for follow up at renal unit from the registration list of patients
3.2. Data Collection and Processing
- A structured standard interviewer administered questionnaire was used after some modifications. The questionnaire was initially prepared in English and then translated in to Amharic version. The Amharic version was again translated back to English to check for consistency of meaning. During data collection supervision was carried out and daily checking of the collected data was made by principal investigator. To assure data quality, data collectors were recruited; training and orientation were given to data collectors and supervisor. About 5% of the data were verified by the principal investigator during the initial stage of data collection and appropriate instruction was given to the data collectors and supervisor. Supervisor and principal investigator were closely followed the data collection process at the spot. Data were entered to Epi-info version 3.5.1 and analyzed by using SPSS 16.0 software.
3.3. Operational Definitions
- Rudd (2000) suggests adherence is the willingness and ability of the individual to follow the clinical prescription. Medicine related adherence: to receive all the prescribed medications regularly in the last month. Diet-related adherence: to consume a low-fat and low-sodium diet and increase vegetables and fruits; exercise-related adherence: to exercise 30 minutes/days at least three times a week; Substance-related adherence: not to smoke (either never smoked or stopped smoking), decrease coffee taking and stop alcohol. The adherence score for each item was obtained by calculating the mean(10). A cut-off point was set at 3 and the respondents were categorized in to adherence and non adherence groups, the respondents with a score of 3 and above were considered as adherent and a score of below 3 were considered as non-adherent.
4. Results
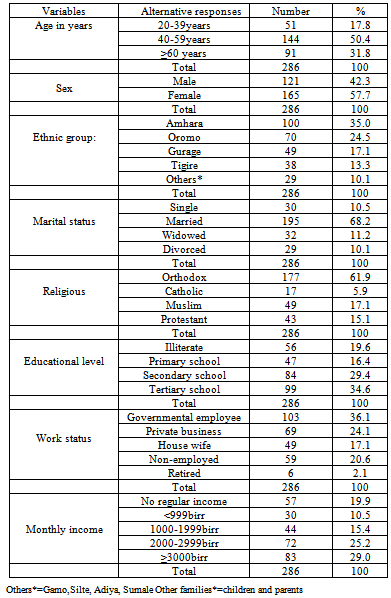
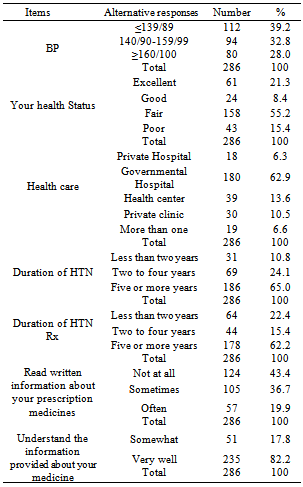
- The total study sample was 286 hypertensive patients, with the response rate of 100%. Socio demographic Characteristics of the study sample are presented in Table 1. The study consisted of 165(57.7%) females. The mean age of the respondents was 52±13.03years. Majority of the respondents 177(61.9%) were orthodox by religion and 195(68.2%) were married. Out of the respondents 99(34.6%) attended tertiary school educational level and 103(36.0%) respondents were governmental employed. Eighty three (29%) of respondents have income ≥3000 Ethiopian Birr (ETB) and 57(19.9%) did not have regular income and live with support from others.As regard information on Hypertension and Patients’ Condition Table 2. Of the respondents 80(28%) had blood pressure ≥160/100mmHg .Concerning health status, more than half of the respondents 158(55.2%) considered their health status as fair. Majority of the respondents 180(62.9%) gone to governmental hospital to receive health care service most of the time and 186(65%) were hypertensive for five or more years and 178(62.2%) were on hypertensive treatment for the same period. Near to two third of respondents 196(68.5%) were on one to two antihypertensive medications. Of the respondents 124(43.4%) never read written information about their medications and 235(82.2%) study subjects were understood very well the information provided by health care givers about their medication.
|
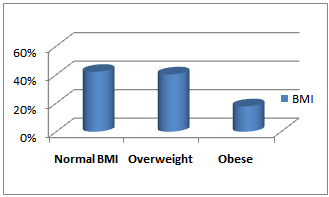 | Figure 1. BMI of respondents (N=286) |
|
| |||||||||||||||||
|
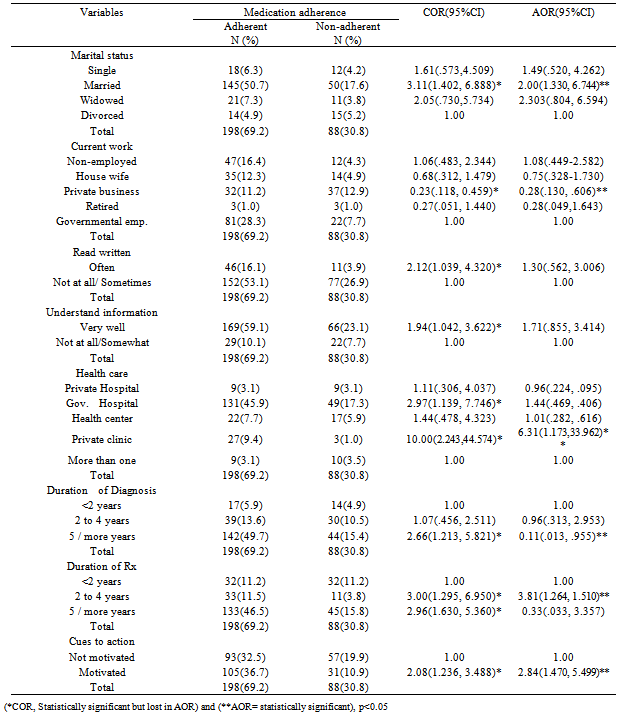
- Adherence From the total study participants 198(69.2%) were adherent to medication regimen where as the rest were not. Married respondents were 2 times more likely to adhere to anti-hypertensive medication compared to divorced AOR=2.00, 95%CI: 1.330-6.744, P=0.008. Respondents who had private business were 72% less likely to adhere to medication compared to governmental employed AOR=0.28, 95% CI: 0.130-0.606, P=0.001. Respondents who attended most of the time private clinic to receive health care were 6 times more likely to adhere to medication than who attended more than one health care facilities AOR=6.34,95%CI: 1.173-33.962, p=0.032. Respondents with the duration of diagnosis of five or more years were 89% less likely to adhere to treatment when compared to with diagnosis of hypertension less than two years AOR=0.11, 95% CI: 0.013-0.955, P=0.045. Those with treatment duration between two to four years were 4 times more likely to adhere to treatment compared to<2years AOR=3.81, 95% CI: 1.264-11.510, P=0.018. Motivated respondents were 3 times more likely to adhere to the medication compared to those not motivatedAOR=2.84, 95% CI 1.470-5.435, P=0.002 (Table 5)
5. Discussion
- Hypertension is one of the mostly prevalent chronic diseases in the world 5, 11, 12. In study conducted in Brazil showed that Adherence to treatment is the most important factor to an effective blood pressure control. Non-adherence to medication is a major factor to non- control of blood pressure in more than two-thirds of hypertensive individuals13. It was identified 69.2% of respondents in this study was adherent to medication which is significantly lower compared to expected index of 80% medication adherence 5, 10, 13, 14. It is also lower than previous studies done in Kuwait 88.6%, Nigeria 75%, India 73%, and Turkey 72% were adherent15, 16, 17, 18.. This might be due to better access and care to patients in these countries. This could also be related to low level of education and low level of awareness related to risk of hypertension complications. Failure to adhere by hypertensive patients to medications can lead them to poor blood pressure control and increased risk of complications. The relation between age and medication adherence was found in studies conducted in New Orleans USA and Iran 19, 20. In this study there was no association between age of respondents and medication adherence. In this study even though there was no significant association between sex and adherence level, females were more adherent than males (40.9% Vs 28.3%). This finding is in line with a study done in Gonder University Hospital (65% Vs35%) 1.This can be explained by the fact that; men are burdened by the outdoor activities which make them busy and make them forget their medications. Alcohol consumption, a commonly practice by males, could also be a barrier for their treatment adherence.In this study awareness of the negative consequence of non- adherence to antihypertensive drug therapy(17.8% Vs 48%), patients attending private hospital(3.1% Vs34.1%) had low level of adherence and adherence to medication in motivated patient(36.7% Vs 65.7%) were low compared to study conducted in southwestern Nigeria 16. This can be explained by the findings of the respondents related to perception of risk was very low (17.8%) in this study groups. Low Perception of negative consequence and lack of reminders could lead to non- adherence. Patients with hypertension for five or more years were 88% less likely to adherent to treatment which is lower than studies conducted in India showed 1.71 times more adherent compare to these who were not adherent 17.This could be related to symptom free nature of the disease, lack of knowledge and continuous reminders. It is important to provide continuous awareness and reinforcement to those groups of patients in this study groups to improve their adherence status. The health care team, especially nurses should emphasis on the awareness creation related to hypertensive complications. There by increase adherence behavior of their patients. In general, lack of organized continuous health education concerning hypertension management might be the cause for non-adherence among these patients.
6. Conclusions and Recommendations
- The adherence to medication was generally low in these hypertensive patients. It was indicated in this study that patients had low perception of risk of complication of hypertension which was reflected by low level of adherence. Factors such as marital status, work status, Health care facilities, duration of HTN and its treatment were associated with medication adherence. The medication adherence was found to be better in patients who had been informed about their medicine. The present study will provide base line information that will enable to explore the problem at wide range by conducting further more research in different segment of populations. Health professionals must educate hypertensive patients about their disease with specific emphasis on its causes, the severity of the disease, their medications and the consequences of non-adherence with treatment. They need to stress the importance of adherence with their hypertension treatment despite the absence of symptoms. It is necessary to stress the benefits of their treatment and their risks of developing complications. The present study will provide base line information that will enable to explore the problem at wide range by conducting further more research in different segment of populations, to investigate the problem in better way and design interventional activities accordingly.
ACKNOWLEDGEMENTS
- This research was funded by Addis Ababa University. Moreover, we would like to thank the study participants and data collectors for their fully participation and responsible data collection.
References
| [1] | Copyright © 2013 Scientific & Academic Publishing. All Rights Reserved Abere D, Getahun A, Solomon M, Zelalem B. (2012): Adherence to antihypertensive treatment and associated factors among patients on follow up at University of Gondar Hospital, Northwest Ethiopia. BMC Public Health; 12:282. |
| [2] | Ronan O’Carroll, Martin D, Marie J, Cathie S. (2010): Improving adherence to medication in stroke survivors (IAMSS): a randomized controlled trial: study protocol. BMC Neurology; 10(15). |
| [3] | Cooper RS, Amoah AG, Mensah GA. (2003): High blood pressure: the foundation for epidemic cardiovascular disease in African populations. Ethn Dis.; 13(2); S48-52. |
| [4] | Fikru T, Peter B, Stig W. (2009): Population based prevalence of high blood pressure among adults in Addis Ababa: uncovering a silent epidemic. BMC Cardiovascular Disorders; 9(39). |
| [5] | Sabate E. (2003): Adherence to long term therapies: Evidence for action. Geneva, Switzerland: WHO; 35(3); 207 |
| [6] | Seedat YK. (2000): Hypertension in developing nations in sub-Saharan Africa. J Hum Hypertens; 14(10-11); 739-47. |
| [7] | Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. (2005): Global burden of hypertension: analysis of worldwide data. Lancet; 365(9455); 217-23. |
| [8] | World Health Organization (2003). Adherence to long-term therapies: evidence for action. Geneva: World Health Organization. Accessed on12/2/2012. |
| [9] | Hashmi SK, Afridi MB, Abbas K, Sajwani RA, Saleheen D, Frossard PM, Ishaq M, Ambreen A, Ahmad U. (2007): Factors Associated with Adherence to Anti-Hypertensive Treatment in Pakistan. PLoS ONE; 2(3); e280. |
| [10] | Carpenter R. (2005): Perceived threat in compliance and adherence research. Nursing Inquiry; 12(3); 192-199. |
| [11] | Aram V Chobanian, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S. (2003): The National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension; 42: 1206-1252. |
| [12] | Chockalingam A, Campbell NR, Fodor JG. (2006) : Worldwide epidemic of hypertension. Can J Cardiol.; 22(7); 553-5. |
| [13] | Rachel G, Bastos B, Nereida Kilza da Costa L. (2006): Adherence rates of hypertension treatment in Brazil and around the world. Rev Bras Hiperten; 13 (1); 35-38. |
| [14] | Jae-Hyun P, Youngsoo S, Sang-Yi L, Sang III L. (2008): Antihypertensive drug medication adherence and its affecting factors in South Korea. Int J Cardiol;128( 3) ; 392-398 |
| [15] | Amal M Al-Mehza, Fatma A Al-Muhailije, Maryam M Khalfan, Ali A Al-Yahya. (2009): Drug compliance among hypertensive patients: an area based study. Eur J Gen Med.; 6(1); 6-10. |
| [16] | Kazeem B Yusuff, Abdrahman A.( 2007): Assessing patient adherence to anti-hypertensive drug therapy: can a structured pharmacist-conducted interview separate the wheat from the chaff? The Inter J of Pharmacy Practice; 15: 295–300. |
| [17] | Subhasis B, P. Sankara Sarma(2011): Adherence to antihypertensive treatment and its determinants among urban slum dwellers in Kolkata, India. Asia-Pacific J of PH. http://aph.sagepub.com/content/early/.abstract? |
| [18] | Ana do lu Kar di yol Derg: The assessment of adherence of hypertensive individuals to treatment and lifestyle change recommendations. Hypertensive individuals and lifestyle 2009; 9: 102-9. |
| [19] | Krousel-Wood MA, Islam T, Muntner P. (2008): Medication adherence in older clinic patients with hypertension after Hurricane Katrina: implications for clinical practice and disaster management. Am J Med Sci.; 336(2); 99-104. |
| [20] | Negin H, Narges R (2004): Determinant factors of medication compliance in hypertensive patients of Shiraz, Iran: archives of Iranian medicine; 7(4); 292 - 296. |
| [21] | Helvi K.(1999): Compliance of patients with hypertension and associated factors in Finland population. JAN; 29(4): 832-839. |
| [22] | Lawrence J, Michael W. Brands, Stephen R. Daniels, Njeri K, Patricia J. (2006): Dietary approaches to prevent and treat hypertension: a scientific statement from the American Heart Association; 47: 296-308. |