-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Microbiology Research
p-ISSN: 2166-5885 e-ISSN: 2166-5931
2015; 5(3): 118-121
doi:10.5923/j.microbiology.20150503.06
Sero Prevalence of Salmonella typhi among Pregnant Women in Niger State
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdogo Liilian, Samuel Graba, Abalaka Moses
Department of Microbiology, Federal University of Technology, Minna, Nigeria
Correspondence to: Adogo Liilian, Department of Microbiology, Federal University of Technology, Minna, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This study reports the prevalence of typhoid fever among pregnant women in Niger state. The study was carried out among pregnant women at the antenatal care unit of nine General Hospitals, in Niger State. Questionnaires were issued to obtain demographic information. Two milliliters of blood sample was collected from each pregnant woman and centrifuged at 1,500 rpm for 5 minutes. Widal test was used to detect the antibody titers in sera were in a titre of 1:80 was considered significant and the result of each patient was recorded. Nine hundred pregnantwomen were examined from the three zones of the state, out of which 610 (67.8%) were infected. Prevalence of Salmonella typhiin relation to age group shows that women between the ages of 35–44 had the highest rate of infection (71.8%).Those within the age groups of 25-34, 15-24 also had a prevalence of 68.1% and 66.7% respectively. The relationship between typhoid fever infection and age group was statistically significant (P = < 0.05). Prevalence of Salmonella typhi in relation to gestation period shows that pregnant women in their third trimester had the highest infection rate (71.5%) while those in their first and second trimester had a prevalence of 66.1%, 65.5% respectively. The relationship between typhoid fever infection and gestation period was statistically insignificant (P = > 0.05). The highest percentage (69.9%) of significant titre of antibodies to Salmonella was detected among subjects who utilize borehole water while the least was detected among subjects who utilize tap water. Well water users recorded a prevalence of 68.5%.There was a significance difference between Salmonella typhiinfectionand water supply (P < 0.05). Four hundred and fifty one women (50.0%) were positive to the somatic (O) antigen indicating acute infection. Typhoid feveris a dangerous infection among pregnant women and is common in Nigeria. Pregnancy makes the host more vulnerable to typhoid fever. Public awareness, early and prompts diagnosis is of great importance in curbing the menace of the diseases.
Keywords: Salmonella typhi, Pregnant women, Typhoid fever, Widal test
Cite this paper: Adogo Liilian, Samuel Graba, Abalaka Moses, Sero Prevalence of Salmonella typhi among Pregnant Women in Niger State, Journal of Microbiology Research, Vol. 5 No. 3, 2015, pp. 118-121. doi: 10.5923/j.microbiology.20150503.06.
1. Introduction
- Typhoid fever is a global infection [1] and is responsible for acute life threatening febrile illness. Typhoid fever is one of the major bacterial infections worldwide. It has an estimated case of twenty two million with two hundred thousand interrelated deaths world-wide annually [2]. Although, typhoid fever is widespread in various regions of the world, the genuine burden of the infection is weakly defined within most endemic countries. The well-known occurrence of multidrug-resistant typhoid fever also complicates the problem [3] [4].The disease is a major challenge and an essential health setback in some continents such as Asia and Africa particularly in Nigeria owing to poor hygienic environment and the absence of or insufficient clean water supply [5]. Typhoid fever is amongst the major prevalent disease in Nigeria due to various interconnected factors such as scarce amenities for handling unwanted products and abuse of antibiotics; these amongst other factors are responsible for the widespread of typhoid fever affecting both little children and young adults [6]. Infection of pregnant women with Salmonella occurs as frequently as its infection in the general populace, with a prevalence of 0.2% positive rectal cultures at the point of delivery [7]. It has been projected that the incidence of foetal loss which occurs from untreated typhoid cases all through pregnancy might be as high as 80% [7].Special concern arises as soon as pregnancy is complicated by S. typhi [8]. Diverse severe outcomes and morbidity connected with typhoid fever in pregnancy include maternal mortality, premature labor, spontaneous abortion and infection of the fetus.Due to the hormonal changes that suppress immunity, pregnant women are at an increased risk for getting food-borne infections [9]. Hormonal changes which occur during pregnancy impair the cell mediated immune response and they increase the susceptibility of pregnant women to various infections. Pregnancy is considered as a high risk factor for acquisition of Salmonella infections [10]. This study examined the incidence of typhoid fever among pregnant women and the effect of gestation period, age and water supply in relation to the incidence of the infection.
2. Materials and Methods
- Study AreaNiger state is located in the Northern part of Nigeria. Niger state lies on latitude 80 to 11:30’ North and longitude 3 30’ to 7 40’ East. The State is bordered to the North by Zamfara State, West by Kebbi State, South by Kogi State, South West by Kwara State, North-East by Kaduna State and South East by FCT. Niger State also has an International Boundary with the Republic of Benin along Agwara and Borgu LGAs to the North West [11].Niger State experiences distinct dry and wet seasons with annual rain fall varying from 1,100mm in the northern parts to 1,600mm in the southern parts. The maximum temperature (usually not more than 94°C) is recorded between March and June, while the minimum is usually between December and January. The rainy seasons last for about 150 days in the northern parts to about 120 days in the southern parts of the State [11].Niger state has twenty-five local government area councils and the state is zoned into the senatorial districts (Zone A, Zone B and Zone C). Three local governments were picked from each zone. General hospital Bida, Lapai and Agaie were used to represent Zone A, General hospital Minna, Suleja and Tafa, were used to represent Zone B and General hospital Kontagora, Kagara, Wushishi were used to represent Zone C. General hospital Minna, Lapai, Agaie, Suleja, Tafa, Kontagora, Kagara, Wushishi and Bida was used for the study. General hospitals are amongst the largest hospitals in Niger state and so attract patients from neighboring villages. It therefore became imperative to use these hospitals as the collection centre for this study. Study Population The study was hospital-based. It was carried out among pregnant women who reported for the antenatal care units of the General hospitals. The purpose and procedures of the study was explained to the pregnant women and demographic information was obtained from each participant through a structured questionnaire. Permission to that effect was received from the hospital ethical committee. The study did not interfere with the normal management of these women. Samples were collected between the months of May and November, 2013 at the various hospitals.Sample collectionBlood samples were collected from 900 pregnant women in the nine hospitals mentioned earlier. For each participant, a tourniquet was tied around the upper arm to enable the veins to be seen and felt using the index finger. When a sufficiently large and straight vein was felt, the women were asked to tighten their fist which made the veins more prominent. The desired site was disinfected using 70% alcohol swab. A sterile needle attached to the needle holder was directed upwards in the line of the vein; two milliliters of blood was collected. The tourniquet was released and the women were instructed to open their fists. The needle was removed carefully and a piece of dry cotton wool was pressed on the punctured site. Two milliliters of the blood samples was centrifuged at 1,500 revolutions for five minutes to separate the serum from the blood cells.Widal testThe widal test commonly used in typhoid diagnosis was carried out in this work. The Widal agglutination technique was carried out according to manufacturer’s instructions (Micropath antigens/ febrile antigens kits) containing the somatic (O) and flagella (H) antigens. Positive and negative serum controls were included; antibody titres of 1:80 or more was considered clinically and diagnostically significant. Laboratory ProcedureThe reagents were stored at 2-8°C until ready for use. The reagents were removed and placed on a flat dry surface and allowed to equilibrate to room temperature before testing. The reagent bottles containing the antigens were shaken before dispensing. The clear serum was picked and dropped on the tile using a pipette into eight (8) different portions. A drop of the undiluted antigen suspension was added to each serum aliquot in the following order. Somatic (O) antigen A, B, C and D and the flagella (H) antigen a, b, c and d. The content of each circle was mixed uniformly over the entire circle with separate mixing sticks and the slide was gently rotated back and forth. The reactions were observed macroscopically after a minute. The agglutination observed in any circle was indicative of anti-salmonella antibodies in the patient’s serum while the absence of agglutination indicates the absence of the pathogen [12].Data analysisStatistical Package for Social Sciences (SPSS) 2014 was used to analyze the results obtained.
3. Results
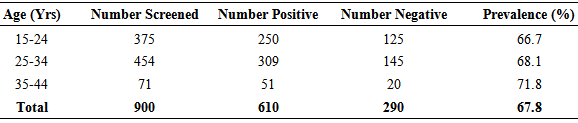
- A total of nine hundred pregnant women were screened in the three Zones. Prevalence of Salmonella typhi in relation to age group shows that women between the ages of 35–44 had the highest rate of infection 71.8% as shown on Table 1. Those within the age groups of 25-34, 15-24 also had a prevalence of 68.1% and 66.7% respectively. The relationship between typhoid fever infection and age group was statistically significant (P = < 0.05).
|
|

|

4. Discussion
- In this study, 610 (67.8%) of the 900 (100%) blood samples were positive for Widal reaction which reveals a high prevalence rate in the population studied. However, this is slightly lower than the results obtained from [13] [14].In relation to age group, Table 1 shows that women between the ages of 35–44 had the highest rate of infection (71.8%). This could also be because women within this age range are more likely to eat and/ or drink freely from public sources. The months of April, May and June in Niger state is usually characterized with extreme temperatures (hot weather). High patronage of packaged water, zobo juice and other tasty drinks are popular during this season. Some of the persons who dispense these items have little or poor knowledge of hygiene or infectious diseases thereby serving as carriers of the infection.Although all ages were affected in this study, the incidence was lower in the age group of 15-24 years. This result is similar to the findings of Pokharel and his colleagues who recorded a low prevalence of typhoid fever among young adults within the age group of 13 – 24 years [15].The results indicate that the infection was highest among pregnant women in their third trimester (Table 3). This could be due to environmental or physiological changes, or immune suppression. According to the findings of Pejcic-Karapetrovic and his colleagues, hormonal changes which occur during pregnancy impair the cell Mediated immune response and they increase the susceptibility of pregnant women to various infections [10].Infection rate in relation to water usage revealed that subjects who utilize borehole water recorded the highest percentage (69.9%) of significant titre of antibodies to Salmonella. This may also be due to contamination with sewage. This could also be because most boreholes are drilled to generate income; therefore most of the boreholes are shallow wells as most of them do not meet the required drilling specification and are thereby exposed to contamination by sewage. Water treatment standards may also be compromised. It could also be due to poor hygiene, improper handling of water and poor storage facilities. Tap water users recorded the highest infection rate in zone C as shown in Figure 4.11. This is similar to the findings made by Udeze and his colleagues [16]. This incidence rate could be because most of the pipes conveying water to various homes are metal pipes which may have been affected by corrosion, thus, the pipes have leakages along the way thereby permitting the entry of microorganisms (Salmonella inclusive) from the soil into the water occasioned by poor sewage disposal, open air defecation and overflow of water bodies during the rainy season. In Niger state, the major ecological problem is flooding, particularly when the Niger River overflows its banks [17].This present study indicates that the sero prevalence of Salmonella typhi among pregnant women in Niger state is quite high and this can be hazardous in pregnancy, as it interferes with the immune process.The infection caused by Salmonella typhi remains an imperative public health problem, especially in this part of the world, therefore, all Antenatal units of hospitals in Niger state and other parts of Nigeria should introduce routine testing of typhoid fever for pregnant women. Provision of potable water and healthcare facilities by authorities at various levels is required in order to put a break to the endemic nature of the infection. To limit the transmission of faecal-orally transmitted infections, enlightenment programs on basic rules of hygiene for such communities should be encouraged. Improvisation of safe drinking water either by boiling, chlorination, addition of sodium aluminate (alum), should be encouraged.