-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Microbiology Research
p-ISSN: 2166-5885 e-ISSN: 2166-5931
2013; 3(6): 213-223
doi:10.5923/j.microbiology.20130306.04
Bacterial Biofilm: A Major Challenge of Catheterization
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJibrinNdejiko Mohammed1, Bashir Mohammed Abubakar2, Hindatu Yusuf3, Mohammed Sulaiman4, Haruna Saidu4, Abdulrahman Idris5, HamzatIbiyeye Tijani6
1Department of Microbiology, Ibrahim Badamasi Babangida University, P.M.B 11, Lapai, Nigeria
2Department of Biological Science, Bauchi State University, P.M.B 65, Gadau, Nigeria
3Department of Biochemistry, Bauchi State University, P.M.B 65, Gadau, Nigeria
4Department of Biological Sciences, Gombe State University, PMB 127, Gombe, Nigeria
5Department of Microbiology, Kaduna State University, P.M.B. 2339, Kaduna, Nigeria
6Faculty of Bioscience & Medical Engineering, Universiti Teknologi Malaysia, johorebahru, 81310, Malaysia
Correspondence to: JibrinNdejiko Mohammed, Department of Microbiology, Ibrahim Badamasi Babangida University, P.M.B 11, Lapai, Nigeria.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Biofilm is a community of microorganisms of same or different species encased in a self-produced extracellular polymeric substance on both living and non-living surfaces. Catheters are generally critical indwelling medical devices commonly used in clinical applications to enhanced flow of fluids out of the patient’s body as well as influx of medications into human biological systems. Like many other indwelling medical devices, catheters are prone to enhanced risk of nosocomial infections which becomes a critical challenge as a result of microbial attachment to the surfaces of the catheters. Attachment and subsequent biofilm development on catheter surfaces cause a number of persistent infections. The biofilm development increases resistance to antibiotics. However, this sometimes led to high pathogenesis, patient morbidity and mortality. This condition usually calls for a premature catheter removal which will increase the cost of treatment and improvidence of resources. This review focuses on how catheters get infected, microbial diversity among catheter biofilms, factors mediating biofilm formation on catheters and current strategies used in controlling biofilm formation on indwelling catheters.
Keywords: Biofilm, Catheter, Antimicrobial, Encrustation, Intra-luminal, Extra-luminal
Cite this paper: JibrinNdejiko Mohammed, Bashir Mohammed Abubakar, Hindatu Yusuf, Mohammed Sulaiman, Haruna Saidu, Abdulrahman Idris, HamzatIbiyeye Tijani, Bacterial Biofilm: A Major Challenge of Catheterization, Journal of Microbiology Research, Vol. 3 No. 6, 2013, pp. 213-223. doi: 10.5923/j.microbiology.20130306.04.
Article Outline
1. Introduction
- Microorganisms are the most abundant form of life on earth; they are numerically more and phylogenetically diverse than every other living forms[1]. Our basic knowledge of microorganisms is based on historical reasons that originate from empirical researches on microorganisms that live in suspension in liquid growth media. However, Microbiologist and biotechnologist have generally found out that most of microbial cells live in spatially distinct communities, otherwise known as biofilms. These organisms mostly grow together and embed themselves in multi-polymer matrix known as Extracellular Polymeric Substances (EPS) to form the sessile microbial communities [2]. EPS is a complex secretion of polymers which include absorbed nutrients, metabolites, products of cell lysis and particles from the surrounding environment. The EPS serves to Protects and provide stability for the surface-bound microbes. It prevents the access of antimicrobials and disinfectants and provides the microorganisms with inherent ability to withstand harsh environmental factors such as UV lights, pH fluctuations, osmotic shock, host immune systems and desiccations[3, 4].In comparison to the free living microorganisms, the functions and pathological properties of biofilms becomes altered. Living as a biofilm confers advantages on the microorganisms such as resistance to adverse conditions (low nutrient, antimicrobials and detergents), and the ability to acquire transferable genetic materials within short period of time[5]. The existence of microorganism in biofilms exert direct or indirect influence on the human biological system in terms of diseases, pipe water contamination, contamination of food contact surfaces and natural environment. It is also worth mentioning that Biofilms offers remarkable advantages in degradation of hazardous organic substances and hence their wide application in the treatment of waste water[6]. On their adherence to a particular surface, the microorganisms increase their adaptation to the environment of the biofilm through mass secretion of the exopolysaccharide[4]. Although it is widely agreed that microbial biofilms can grow on every surface, their significance in health care services such as their critical role in medical-indwelling devices is sometimes underestimated. Majority of nosocomial infections have been linked to the growth of biofilm on biosurfaces and indwelling devices used in the treatment of processes. Biofilm growth and development on the indwelling medical devices resulted from adhesion and subsequent capsule formation by the adherent organisms [7].Catheters are plastic tubes used to enhanced flow of medications and waste substances into and out of the human system. Intravascular catheters are mainly used to pass medical substances or medications directly to the patient’s blood circulatory system; urinary catheters on the other hand are used to remove waste fluids from the patient’s urinary compartments[8]. The major challenge of catheterization in health care services has direct relationship with development of biofilms on the catheters[9]. Biofilms can formed on indwelling medical devices including prosthetic heart valve, pacemakers, central venous catheter, urinary catheter, contact lenses, intra-uterine devices etc. thereby causing persistent and deadly infections[10]. In another development, Infection of patients been treated with indwelling medical devices dated back to the fourteenth Century[11]. Meanwhile, the relationship between such infections and the Kosch’s postulate in many instances are still yet to be fully established thus implicating biofilm as the causes of the indwelling device-related infections[9].
2. General Overview of Biofilm Formation
- Biofilm is a community of microorganisms of same or different species encased in an extracellular polymeric matrix and are normally found on both living and non-living surfaces. Generally, biofilm formation is initiated with the adherence of individual cells to the preconditioned biotic and abiotic surface layers[12, 13].The presence of bulk solution or fluid on these surfaces serve as the basis or foundation for the biofilm formation[14, 15]. This is followed by a reversible attachment which is normally mediated by gravitational migration of individual cells, motility of the bacteria and the shear force of the surrounding mobile phase[16]. The irreversible attachment occurs as a result of concurrent production of the EPS and the strong interactive forces that exist between the microbial appendages and the surfaces[17]. This process occurs between 20 minutes to 4hours depending on the physiology of the species involved and the nature of the preconditioned surface layer[17, 18]. Meanwhile, as the microbial cell move closer to a surface (<1nm), the initial attachment is facilitated by the attractive or repulsive electrostatic and hydrophobic interactions, steric hindrance and van der Waals forces[10]. The hydrophobic interactions have been postulated to play important roles in the primary adhesion[19], while the irreversible attachments are mediated by the molecular interactions that exist between specific adhesions and the surfaces[10]. The entire adhesion has also been explained with the aid of different molecular cell contact theories such as Derjagun-Landau-Verwey-Overbeck (DLVO) theory and the extended DLVO theory and the thermodynamic approach[14, 15, 20]The maturation of biofilm is attained when the irreversibly attached cells develop to form a more organised and complex structure whose shape depend on source of the nutrients, however mushroom structure is common among bacteria biofilms[21]. This is followed by microbial dispersion which is the final stage of biofilm development and occurs when there is alteration in the mature biofilm structure as a result of increased shear force, depolymerisation of the EPS, use of antimicrobials and nutrient depletion[20, 22]. This final dispersion of biofilm is a complex process that plays a crucial role in initiating and transmitting infectious diseases. The major steps of the biofilm formation are illustrated in the Figure 1 below as adopted from Otto, 2004.
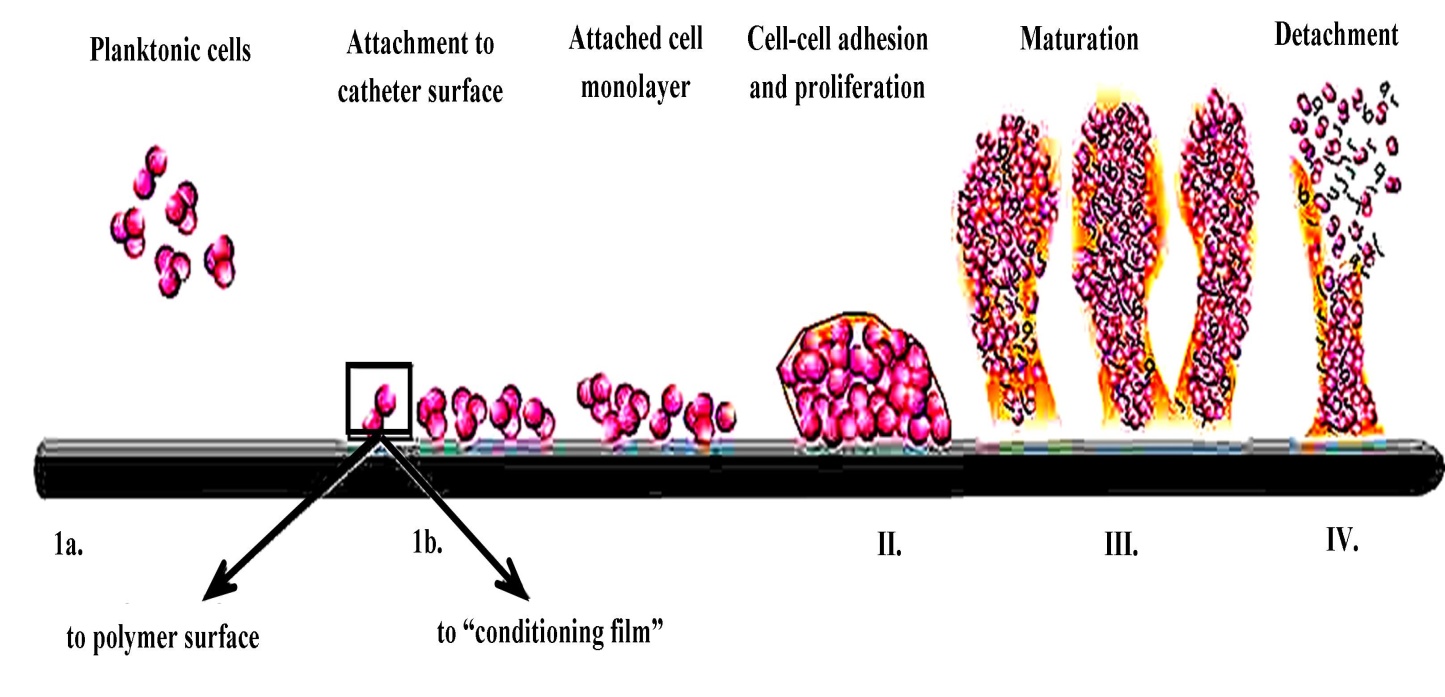 | Figure 1. Themajor steps in Biofilm formation[23] |
3. Contamination of the Catheters
- Over 80,000 infections associated with catheters are been reported per annum by the intensive treatment units (ITU) of the United State of American (USA) alone and approximately 250,000 to 500,000 clinical cases per annum in the entire hospitals in USA[24]. These catheter-linked infections originate from microorganisms that attached to the implanted device in the process of insertion, cross-infection via body contacts and/or during surgery with contaminated surgical tools. (See Figure 2)It has been observed that the principal waysby which microorganisms reach and subsequently contaminate these catheters is usually through themovement of the skin’s microbial flora from the point of insertion to the catheter tract and along the tip of the catheter[25], Contamination of the catheter hub as a result of its direct contact with hands or contaminated liquids and other medical instruments, spreading of the contamination from another point of infection via blood flow and rarely contamination as a result of an infusate. There have been well recognized evidences that associate catheters with infection and subsequent involvement of biofilms in such infections in various literatures. This is due to the fact that catheter itself is a potential substratum for microbial adherence and subsequent biofilm development. Apart from being infected by the haematogenous route catheters can also serves as the channel for the passage of skin microbial flora into the patient’s body[8]. The Intravenous catheters and urinary catheters mostly used in many hospitals have also been found to be the frequent cause of nosocomial acquired bloodstream infections by the coagulase-negative staphylococci which account for about one third of episodes of catheter-related bloodstream infection[26, 27]. Infection of the Central venous catheter (CVC) has been reported to cause an in-hospital mortality rate of up to 35%, long time hospitalizations, and many complications that are associated with the treatment of such infections[8]. Catheter-associated urinary tract infections (CAUTIs) are also common type of hospital acquire infections that are of significant interest due to their complexity and frequent reoccurrence. These infections have been linked with Escherichia coli and Proteus mirabilis whose virulence factors have been reported to include adhesion, motility, biofilm formation, resistance to immunity and acquisition of nutrient[28].
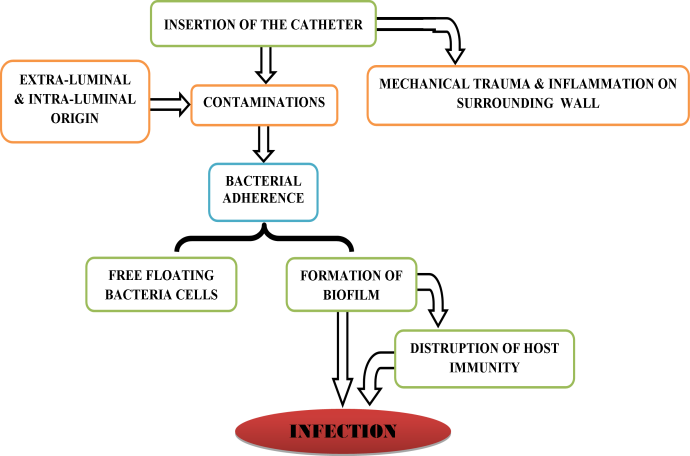 | Figure 2. Schematic flow of catheter contamination and other events that lead to infection |
4. Role of Biofilms in Producing Catheter Related Infections
- The role of biofilms in initiating catheter related infections cannot be overemphasized. Their roles include detachment of the cells from the biofilm to initiate blood stream infections and infections of urinary tract, production of endotoxins by the biofilm encased gram negative bacteria [29], prevention of the damaging effect of the host immune system, transfer of plasmid through the process of conjugation which leads to generation of antibiotic resistance strains[10], encrustation or obstruction of catheters with crystallised substances produced by the bacteria. Development of gravels and pyelonephritis has also been associated with bacterial colonization of the catheters and subsequent biofilm formation[30]. Rodríguez et al.[31] investigated Biofilm formation in Acinetobacterbaumannii with respect to its associated features and clinical implications using microtiter assay and reported biofilm formation by Fifty-six (63%) of isolated 92 strains. Thomson et al,[8] also reported that urinary or bloodstream infections associated with catheter and cerebral shunt-related meningitis are caused by bacterial strains that have potential to form biofilm easily. In another development Dolan (2001) stated in his review that biofilm formation on CVCs is universal, He however emphasized that the extension and location of such biofilm is dependent on the length of catheterization. Short-term catheterization (<10 days) tends to favour greater biofilm development on the external surface while long-term catheterizations (30 days or more) tend to favour greater biofilm growth on the inner lumen of the catheter[32]. It is also important to note that the accidental breakdown of catheterization can result in early bacteria colonization of the catheters. Evaluation and analytical comparison of intra - luminal and extra-luminal source of urinary catheter-related infections revealed that unexpected breakdown of catheters and subsequent introduction of contaminants causes bacteriuria within first two days. However, bacteriuria delayed to after 3-7 days when closed and sterile catheterization was maintained[33]. The type of the fluid passing through the catheters can also influence biofilm formation in the sense that Gram-positive organisms such as Staphylococcus epidermidis and Staphylococcus aureusgrow poorly in intravenous fluids, whereas Gram-negative bacteria such as P. aeruginosa, Pantoeaspp, Klebsiellaspp., Enterobacterspp. and Serratiasppcansustained their growth in intravenous fluids [32]. Upon insertion, both the inner and outer surfaces of the urinary catheters serve as targets for microbial attachment and subsequent biofilm development. Endogenous microorganisms that originate from the gastrointestinal tract have been found to colonized the region of the body between the anus and the scrotrum/ vulva and ascend the catheter via extra-luminal route during catheter insertion. The exogenous microorganisms which can originate from cross contamination from the hands of medical personnel on the other hand, move upward the catheter via intra-luminal route (access of the organisms to the inner lumen of the catheter)[34]. Investigation of a number catheters shows that the thickness of catheter biofilms ranges from small patchy layers of attached cells to extensive biofilms that often covers the entire length of the inner lumen of the catheter and comprising of a very high bacterial population[7]
5. Microbial Diversity in Biofilms of the Catheter
- Over the last decade, catheters, most especially the urinary catheters has become the second commonly used indwelling material inserted to the body of patients. This has subsequently resulted in increased infections of urinary catheters (IUC) with over 40% of the nosocomial infections occurring in catheterized patients during the first 10-14 days of catheterization[30]. Microrganisms most often isolated from catheter biofilms include Candida albicans, P. aeruginosa, K. pneumoniae, Enterococcus faecalis, S. epidermidis[32], Acinetobacterbaumannii[8] and Escherichia coli, while the strongest biofilm producers are Proteus mirabilis, E. faecalis, Candida tropicalis, andStaphylococcus aureus which are also responsible for the mixed species biofilms[30]. Bonkatet al[35] studied microbial biofilms in suprapubic catheterisation that are nowadays used as an alternative to urethral catheterization using conventional culture techniques and isolated a total of 428 microorganisms of which Enterobacteria, Enterococcus and P. aeruginosa were the most frequently isolated spp. They also compared the frequency of catheter associated with bacteriuria in suprapubic catheterisation with those of published findings of urethral catheters[36-38] and reported no significance difference between the two. They were however speculative on the reduction of catheter associated urinary tract infection with the suprapubic catheterization [35] .In another development, Choeet al[39] analyzes bacteria distribution of biofilms that grows on urinary catherters using 4 different 16S rRNA approaches namely capillary electrophoresis, terminal restriction fragment length polymorphism (T-RFLP), denaturing gradient gel electrophoresis (DGGE), and pyrosequencing. They isolated 329 spp of which Edwardsiella, Enterobacter, Escherichia, and Pseudomonas were the predominant isolates for each of the four techniques. Other represented organisms they isolated include Moraxella, Proteus, Serratia, Yersinia, Burkholderia, Corynebacterium, Achromobacter, Alcaligenes, Citrobacter, Stenotrophomonas, and Streptococcus[39]. Meanwhile, systematic antimicrobial treatments during catheterization have been reported to reduce microbial diversity on the urinary catheters. Frank et al.[40] used molecular techniques involving PCR and cloning to investigate diversity of microorganisms on the urinary catheters and reported that both outer and inner surfaces of 8 catheters removed from patients undergoing no systemic antimicrobial treatment were colonized by 20 different microbial species. However a wide variation existed between the internal and outer surfaces whereas only one catheter out of six was colonized by a single microbial species in patients undergoing systematic antimicrobial treatment[40, 41].
6. Factors Mediating Biofilm Formation on Catheters
- Development of biofilms on catheters is determined by several variables. The microorganisms must be able to adhere to the exposed surface of the catheter and become irreversibly attached. Attachment of the microbial cells is dependent on the physiological and chemical properties of the surface, hydrophobicity of the microorganisms and the substratum; catheters that are both hydrophobic and hydrophilic in nature favours attachment of wide species of microorganisms. Divalent cations such as calcium and magnesium increases the urinary pH and ionic strength and has been reported to facilitate bacterial attachment[42]. Other factors include production of platelets, tissue proteins and sera (host preconditioning films), number and type of the microbial cells, the rate at which the liquid flows through the surface of the catheter and the composition of the liquid itself[15, 43, 44]. As a result, the irreversible attachment and production of EPS promote the formation of biofilm as the biofilm growth rate continue to be affected by the flow rate, nutrient and antimicrobial composition of the liquid passing through the catheter and the ambient temperature[32].In another development, the surface coating of the central venous catheters with heparin has been reported to exhibit the potential to reduce in vitro and in vivo microbial attachments. Appelgrenet al. (1996) found that in vitro adherence of coagulase-negative Staphylococci to heparin coated catheters was drastically reduced as compared to non heparinized catheters (p < .05). In the in vivo study of 32 central venous catheters, he observed bacteria and fungi colonization in only four of the thirteen heparinized catheters while fourteen out of nineteen were colonized in the no heparinised catheters with the coagulase-negative Staphylococci been the most frequently isolated bacteria in both cases[45]. It has however been observed that low citrate concentration and sodium heparin that is widely used as catheter lock solution can serve as a strong stimulant for S. aureus biofilm formation[46].
7. Encrustation and Obstruction of the Catheters by Biofilms
- Encrustation of catheters results from the deposition of mineral salts such as magnesium phosphate, ammonium phosphate and calcium phosphate on both the inner and outer layer of the catheters. These mineral salts accumulate as a result of microbial activities that exert functional roles to increase the acidity of normal urine and turn it alkaline in urinary catheters[47]. In addition to occluding the lumen of the catheter and subsequent urine leakage or retention which inflicts pains and distress on the patients[48], these deposits also causes trauma to the urethra and bladder mucosa. Encrustation and unidentified blockage can also lead to disease conditions such as pyelonephritis, septicaemia and shock[47]. About half of catheterized patients most especially, the elderly people suffer from encrustation and obstruction (catheter blockage). This is common of long time catheterization and gives rise to more community nursing caseload[49]. A wide number of studies have demonstrated that the steps involved in encrustation to include bacteria contamination of the urinary tract predominantly by P. mirabilis and other urease producers, multiplication and their attachment to the catheter, subsequent biofilm formation and accumulation of the extracellular polymers which elevate the urine pH and triggers the stabilization of the crystallized magnesium and calcium phosphates on catheter inner surface[48, 50-52]Electron microscopy of catheter encrustation reveals the presence of large numbers of bacilli known to easily form biofilm conforming to the view that encrustations originate from mineralized biofilms. Bacteriological studies of the encrusted catheter biofilms also show the urease producing P. mirabilis to be the dominant isolate[7, 47]. Although many studies reported biofilm mineralisation to be involve in encrustation, other studies reported involvement of bacterial capsule polysaccharide which enhance more stabilization of the crystals[51, 53]. Thus the general methods for preventing encrustation involves incorporating antimicrobials to the polymers and designing catheters whose surface property will not allow initial bacterial attachment[54]. A photograph of catheter tip with encrustation (adapted from Hoet al.) is shown in Figure 2.
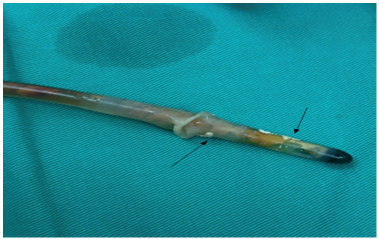 | Figure 3. Residual encrustations at the catheter tip after it removal[55] |
8. Mechanism of Antimicrobial Resistance in Catheter Biofilms
- Generally, antimicrobial agents known to be effective against microorganisms that grow in suspension frequently fail to exert their effects when used on the microorganisms that grow in biofilms. This has been attributed to a variety of mechanisms which includes the accumulation of the extracellular polymeric substance that tends to allows partial or zero penetration of the antimicrobial agents in to the microorganisms (see Figure 4) for instance,aminoglycosides with positive charge can bind to negatively charged polymeric substances in the biofilm matrix and retard their penetration. EPS can also dilute the antimicrobial concentration before they get to the individual cells in the biofilm, thus reducing the potency of the antibiotics against microorganisms[4, 56]. Microorganisms grow slowly when they are in biofilm and therefore become resistance to antimicrobial agents that requires vigorous microbial growth, the slow growth also promote poor expression of antimicrobial binding proteins among organisms growing in biofilms. Other mechanisms of resistance in biofilms include activation of multiple genetic materials that allow microorganisms to alter their cell envelop, the molecular targets, and the susceptibility to specific antimicrobials. This mechanism of resistance is otherwise refers to intrinsic resistance[57, 58].
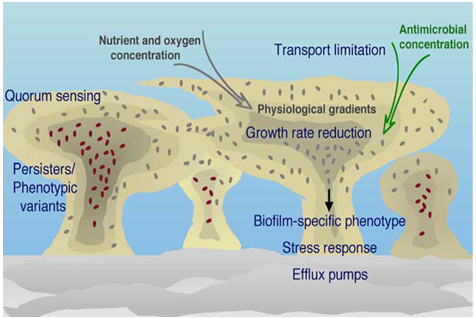 | Figure 4. Mechanisms of biofilm antimicrobial resistance[64] |
9. Current Strategies in Controlling Biofilm Development on Catheters
- One of the best ways to prevent biofilm development on any surface is to prevent the initial attachment of microbial cells by avoiding contamination of the exposed surface. The preventive measures in catheter related blood stream infection include prevention of extra-luminal contamination through adoption of aseptic measures such as the use of sterile gloves, gown, cap, and mask during the insertion of the catheters. The use of skin antisepsis such as 2% aqueous chlorohexidine-containing antiseptics which has been reported to be very effective is also another pre-infection measure[65]. The number of skin micro flora at the insertion site is an important factor that should be considered to prevent catheter related blood stream infection. It is recommended that central venous catheters be inserted at sub-clavian sites as the catheters inserted into jugular have been reported to possesses higher risk of microbial colonization in comparison to those inserted into a subclavian[25, 66]. Furthermore, to prevent endoluminal contamination, the hub should be handled with high degree of asepsis. This can be achieved by protecting the hub using an iodine-impregnated foam or povidone, external protection of the hub, ensuring spacing in changing the infusion set and reduced number of lumens in the catheter. Povidone iodine is also the commonly applied antiseptic in USA for cleansing arterial catheter and insertion site of the central venous catheters (CVC)[67]. Other preventive measures include avoiding unnecessary manipulation of catheters, use of antiseptic connectors and involvement of well-trained proffessionals[66]. Some of the commonly used strategies of preventing contamination of the urinary catheters such as systematic or direct introduction of antimicrobial agents in to the bladder and catheter irrigation has all been reported to be ineffective measures of preventing microbial colonization of the urinary catheters[36]. Modification of materials used for catheter design is another economic and effective preventive measure that is recently used in the medical industry. In this approach, the catheter surfaces are modified to avoid microbial adhesion[68, 69]. The proposal is to construct a device without any fouling properties in order to minimize adsorption of protein and subsequent microbial adhesion and at the same time preserving the favourable characteristics of the device in terms of its strength and inertness[70]. An in vitro study has shown that use of heparin, sodium citrate and sodium EDTA, can hindered biofilm development by S. aureus indicating that they can be applied to reduce the biofilm-associated infections in indwelling catheters[46].Furthermore, the used of antimicrobial agents to control biofilm formation on medical indwelling devices has been investigated by many researchers. Dolan[32] reviewed that augmentation of dextrose-heparinized left atrial catheter with sodium metabisulfite prevented the microbial colonization of the catheters and also reported that minocycline and rifampin impregnated catheters experiences less microbial colonization as compared to chlorohexidine and silver sulfadiazine impregnated catheters. Similarly, the impregnation of central venous catheter with minocycline- rifampin (M/R CVCs) has been found to be efficient in combating catheter-related blood stream infections and subsequent biofilm formation by both Gram-positive and Gram-negative organisms[71, 72]. It was however not effective on P. aeruginosa and Candida spp.In order to increase the antimicrobial performance of this approach, Raadet al.[71] developed a novel minocycline/ rifampin catheter that included chlorhexidine (CHX-M/R catheter) which they found to have prolonged activity and effective in complete inhibition of all the resistance strains including the Pseudomonas aeruginosa and Candida spp. In a related research, Kamal et al.[73] in their study of reduced intravascular catheter infection by antibiotic bonding found that cationic surfactant coated catheters bonded with cephalosporine has less microbial contamination and biofilm development than the untreated catheters. Application of ointment containing multiple antibiotics prior to insertion of attachable subcutaneous cuff that contains silver ions, coating the inner lumen of the catheter with an antibiotic, using topical antibiotics and removing the contaminated catheters can also reduce contamination of catheters and biofilm development that accompany such contaminations [32].Dolan[74] reviewed that novel techniques such as the use of chelating agents, biofilm dispersants, quorum sensing inhibitors and bacteriophages can eradicate biofilms on intravascular catheters. The Chelating agents such as ethylene diaminetetraacetic acid tetrasodium EDTA or disodium EDTA and minocycline-EDTA are capable of destabilizing the biofilm structure[75]. To support this, Percival et al.[76] and Kite et al.[77] reported that 40 mg/mL of tetrasodium EDTA was able to eliminate biofilms in an in vitro model and on hemodialysis catheters respectively. Other forms of preventive techniques include: i. mixture of tigecycline and disodium EDTA with gentamicin and disodium EDTA which has been reported to drastically reduced biofilms of Staphylococcus species and P. aeruginosa growing on Hickman catheter[74]. ii. Dispersal of microbial cells from biofilms by shedding of daughter cells during active growth can be achieved by changing the nutrient levels or quorum sensing or by the use of flow shear force.iii. Oxidizing biocides, such as chlorine, surfactants, or enzymes can also cause disruption and subsequent dispersal in biofilms[74]. iv. Unsaturated fatty acids such as cis-2-decanoic acid produced by P. aeruginosa can disperse several clinically relevant biofilms in vitro. This type of dispersion is taught to be as a result of degradation of the EPS by neighbouring cells in response to the cis-2-decanoic acid (signalling molecule). However this approach requires additional treatment with antibacterial agents to prevent reattachment of the dispersed cells[78].v. Some strains of bacteriophage produce polysaccharide depolymerases that are capable of degrading the biofilm EPS. Curtin and Dolan[79] and Fu et al[80] both studied the use of bacteriophage to prevent biofilm prevention and reported the prevention ofS. epidermidisand P. aeruginosabiofilm growth on phage treated catheters.
10. Techniques of Studying Catheter Biofilms
- Generally, a wide number of techniques and models have been used to study microbial biofilms on different surfaces. Some of the common techniques include direct microscopic techniques such as confocal laser scanning microscopy, atomic force microscopy and scanning electron microscopy, micromanipulation,[1, 14, 81-83]. These models involves theuse of flow cells, 96 well micro titer plate also refered to as the Calgary Biofilm Device, colony biofilms, biofilm ring test, micro fermentors and modified robbins devices[84, 85]. However, some of these models yielded positive results in in vitroinvestigation, they do not really represent the ideal conditions in the studies of biofilm related infection such as catheter biofilms.In order to establish a comprehensive technique for studying and controlling biofilms on medical instruments such as catheters, there is need for simulation and development of direct and no destructive techniques and models that represent the actual clinical conditions[86].In order to quantify biofilms on central venous catheters, an internationally referenced method otherwise known as Maki's semi-quantitative method or roll plating technique can be employed. In this method, the tip of the catheter is removed and moved randomly over a general purpose agar medium to count the number of the microorganisms after a specified period of incubation[32]. This method suffers the disadvantage of not able to discover more than 1× 103 colonies and it inability to detect biofilms growing on the inner lumen of the catheter[87]. An improved semi quantitative roll plating that uses sonication and vortex to quantify biofilms can detect up to 1 × 104 colonies per tip however there is need for further determination of its recovery efficiency[86]. The use of acridine orange to directly stains the catheter biofilms is a rapid method that do not modify the clinical conditions of the catheters and simply record positive and negative results instead of quantifying the cells[32, 88]. Another culture independent technique used for studying catheter biofilms is the molecular technique which involves 16s rRNA, polymerase chain reaction PCR, denaturing gradient gel electrophoresis DGGE and Fluorescence in situ hybridization FISH[39, 89, 90]. These techniques is based on application of PCR to amplify the segment of 16s rRNA isolated from the biofilm sample, this will produced a combined PCR products from the various microorganisms that constitute the biofilm. The PCR products are subsequently subjected to screening and separation by DGGE to produce an order of bands which correspond to various microbial species in the biofilm sample[89]. This technique is faster and overcomes the problem of misrepresentation in the rolled plate culture technique and has been used to study microbial diversity of biofilm samples [39, 89].In another development, Hassan et al[91] compared Tissue Culture Plate (TCP) method, Tube method (TM) and Congo Red Agar method (CRA) for their ability to detect biofilm formation in about 110 clinical isolates and reported the superiority of the TCP over TM and CRA, for the details about these methods the reader is refer to the work of Hassan et al[91]. In a related study, clement et al.[92] used crystal violet staining, biofilm ring test, and resazurin assay to study biofilm formation in 34 clinical E. coli strains. Comparing the analysis of the 3 methods, they state that “there was significant correlation between CV and RZ assay (Spearman r = 0.68; P < 0.0001) and between CV and BRT (Spearman r = 0.54; P = 0.0007). RZ and BRT were not significantly correlated (Spearman r = 0.18; P = 0.28)”.
11. Conclusions
- Microbial biofilms pose a major challenge to the entire catheterization process and account for most nosocomial infections in catheterized patients or patients under treatment with other indwelling medical devices. Apart from resistance to host immune system, the developments of biofilms by the microorganisms drastically reduce their sensitivity to the antimicrobial agents and make them almost impossible to eradicate using the conventional methods. In addition to obstruction and encrustation of the catheter by these biofilms which inflict serious pains and distress on the patients, detachment of microbial cells from the catheters results in serious infections. Although medical indwelling devices has different design features, important factors such as duration of catheterization, composition of the surrounding fluids or nature of fluid flowing through the catheter, the flow rate, the type of the contaminating microorganism and preconditioned film determines the type and extent of biofilm development on indwelling catheters. Combating the challenge posed by biofilm development on indwelling catheters is based on conducting researches that evaluate the existing control strategies and their effectiveness while developing both in vivo and in vitro catheter related models of biofilms that considers the specific conditions found in catheters in order to come up with reliable and novel techniques. Development of novel aseptic measures that prevents the initial colonization and microbial attachment to the devices will also help in combating the challenges of biofilms in medical care. There is also need to improve the in situ imaging of biofilms, probes for real time analysis and characterization of biofilm specific gene regulators.