-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Microbiology Research
p-ISSN: 2166-5885 e-ISSN: 2166-5931
2013; 3(3): 107-110
doi:10.5923/j.microbiology.20130303.01
Prevalence and Seasonal Variations of HIV 1 and 2 Infection among Children in Abeokuta, South West Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMotayo BO1, Usen U2, Folarin BO2, Okerentugba PO3, Innocent-Adiele HC3, Okonko IO3
1Department of Microbiology and Parasitology, Federal Medical Centre, Abeokuta, Ogun State, Nigeria
2Heamatology and Blood transfusion Unit, Federal Medical Centre, Abeokuta, Ogun State, Nigeria
3Department of Microbiology, University of Port Harcourt, P.M.B. 5323 Uniport post office, Choba, East-West Road, Port Harcourt, Rivers State, Nigeria
Correspondence to: Okonko IO, Department of Microbiology, University of Port Harcourt, P.M.B. 5323 Uniport post office, Choba, East-West Road, Port Harcourt, Rivers State, Nigeria.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
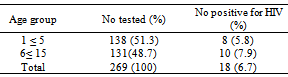
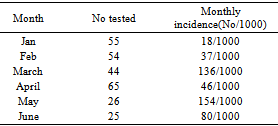
Recent studies have shown a high prevalence of HIV infection among children in Nigeria. Abeokuta still remains un-investigated for the exact prevalence of paediatric HIV infection. We have there tried to bridge this gap in Knowledge by determining the prevalence of paediatric HIV infection in Abeokuta. A six month retrospective study was carried out between January and June 2010 to determine HIV sero-prevalence and seasonal incidence of HIV. About 269 children were screened using double parallel rapid HIV antibody test kits: Chembio HIV-1/2 Stat-Pak® and Determine HIV-1/2® test kit following manufacturer’s instructions. An overall sero-prevalence rate of 14.9% (n=18) was recorded with no statistically significant association in relation to gender p < 0.05, age range 6 to 15 recorded a higher prevalence with 7.9% (10/131) while age 1 ≤ 5 recorded 5.8% (8/138). The highest incidence of infection was seen in the month of May with 154/1000 children tested and the lowest incidence was recorded in the month of January with 18/1000 children tested. This study has shown a relatively high prevalence rate of HIV infection among children in Abeokuta. It is therefore advocated that PMTCT and support services be scaled up in children with HIV in Abeokuta.
Keywords: Prevalence, HIV 1&2, Paediatric infection, PMTCT, Abeokuta
Cite this paper: Motayo BO, Usen U, Folarin BO, Okerentugba PO, Innocent-Adiele HC, Okonko IO, Prevalence and Seasonal Variations of HIV 1 and 2 Infection among Children in Abeokuta, South West Nigeria, Journal of Microbiology Research, Vol. 3 No. 3, 2013, pp. 107-110. doi: 10.5923/j.microbiology.20130303.01.
Article Outline
1. Introduction
- The Human immunodeficiency virus (HIV) pandemic is by far the most persistence medical challenge of man science the turn of the century. Since its discovery in America[1], the virus which is responsible for the development of AIDS has eluded medical solution. Thankfully, treatment of the infection is now possible with HAART[2,3], this does not completely clear the virus because of its unique properties of sequestration and cellular integration in diverse cell types[4,5]. The HIV pandemic is most severe in developing world with Sub-Saharan Africa being the most affected with about 1.9 million new infections in 2008 and about 22 million people living with AIDS in the sub-region[6]. One the most severely affected sub-population groups are children with various medical and social implications[7,8]. In 2008 alone, about 2.1 million children were reported to be living with HIV[6]. This figure has brought to bear the extent of burden exerted by paediatric HIV infection globally. In Nigeria, there is lack of sufficient data to demonstrate the actual burden of paediatric HIV in Nigeria[3], although there are several reports of institution based studies showing various prevalence rates across the country[8-10]. Studies done retrospectively have however indicated that likely seroprevalence rate may range from 5.7% to 20%[3]. However, current projections show an increase in the number of new AIDS cases in Nigeria, the alarming thing is UNAIDS estimated that 1 million Nigerian children were orphaned by AIDS by the end of 2001[6]. In developing countries such as Nigeria, new infections of paediatric HIV are mostly acquired through mother to child transmission [3,11]. Clinical presentations of paediatric HIV infections include respiratory tract infections, otitis media, diarrhoea disease, malnutrition and septicaemia[3, 9]. This puts infected children at great risk of mortality as severe immunosuppression commences early in children[12]. Serological testing which is the universally acceptable format of screening for HIV infections is of limited use in younger children particularly neonates born to HIV positive mothers, thus testing of children of 6 months and below born to HIV positive mothers is by diagnostic PCR methods[5]. There is a general lack of data on paediatric HIV in Abeokuta, a cosmopolitan city with a rising number of new HIV infections[13]. Although with the introduction of HAART to the paediatric age group, HIV related child mortality has been greatly reduced. There is a need to have a clear picture of the current prevalence rate of HIV infections in Abeokuta for the purpose of health systems planning and HIV care and prevention programmes. Our objective therefore, was to investigate the current prevalence of HIV and trend of infection in children at Abeokuta, Ogun state, Nigeria.
2. Materials and Methods
2.1. Study Area and Population
- Abeokuta city is the capital of Ogun state in Southwestern Nigeria. It is located at latitiude 709’N 3021’and longitiude with a population estimate for about 593,140 by 2005 estimates. The study site was Federal Medical Center, Idi-Aba HIV laboratory, which severs the Antiretroviral Clinic (ARV) and PMTCT (Prevention of mother to child transmission) programme. The Federal Medical centre is a 300 bedded tertiary Hospital serving Patients from all over Ogun state and neighbouring States like Lagos and Oyo States. The study was done between January 2010 and June 2010, children of age range 18 months to 15 years were recruited for the study. Information regarding demographic of the study participants were retrospectively retrieved from the Laboratory register after receiving oral permission from the Hospital Laboratory focal person for IHVN supported ARV programme. The highest degree of confidentiality was given to all information regarding study participants in accordance to the Belmont Report[14].
2.2. Sample Collection
- Whole blood was drawn from each child into EDTA bottles through venepunture. About 3mls of blood was collected aseptically and the plasma separated by centrifugation before testing was done almost immediately.
2.3. HIV 1 and 2 Antibody Testing
- All laboratory test was done at the IHVN supported HIV laboratory at F.M.C Abeokuta. Testing was done according to the Federal Ministry of Health (FMoH) testing Algoritim, using 2 rapid kits. The screening test was done using double parallel rapid HIV antibody test; Chembio HIV-1/2 Stat-Pak® (Chembio Diagnostics Systems, Inc. Medford New York 11763 USA) and Determine HIV-1/2® test kit (Abbott Japan Co., Ltd. Minto-Ku, Tokyo, Japan) according to the manufacturers’ instructions. The principle of action of the 2 test kits is based on qualitative, chromatographic, lateral flow immunoassay for the detection of HIV antibodies. A seropositive test was interpreted as an observable reaction in both test kits. Discordant results and seroreactivity to a single kit were recorded as seronegative. Discordant results were recommended for retesting after a period of 3 months. Subjects with double rapid HIV antibody non-reactive test results were reported as HIV-uninfected.
2.4. Data Analysis
- All data generated from the study were presented using descriptive statistics. The data was analysed using chi square test and ANOVA to determine any statistical relationship between the various variable analysed. Confidence interval was set at p< 0.05.
3. Results
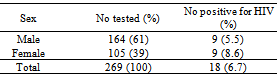
- During the study period, a total of 269 children ages 18 months to 15years, median age 5yrs comprising 164 male and 105 female children. Distribution of HIV 1&2 seropositivity in relation to demographic variables is shown in Table 1 and 2, while Table 3 shows the monthly HIV incidence rate for the half year period. An overall sero-prevalence rate of 14.9% (n=18) was recorded with no statistically significant association in relation to gender, (p < 0.05).Table 1 shows the distribution of HIV seropositivity in relation to gender, the proportion of male children tested was higher with 164 (61.0%) and females 105 (39.0%). Females recorded a higher HIV prevalence than males with 6.7% (9/105), while males recorded 5.5% (9/164) in the sub-population, while both genders recorded the same value in the total[population tested 3.35% (9/269). There was no statistically significant difference of HIV prevalence in relation to Gender (p < 0.05; x2 chi square).
|
|
|
4. Discussion
- The overall prevalence rate recorded in our current study was 6.7%. This is lower than most of the recent reports conducted in nearby centers in Nigeria such as a study done recently at Ibadan by Ogunbosi et al.[3] which reported a prevalence of 10.0% and another study done at Anyingba Kogi State that also reported 10.0% prevalence[8]. Studies from the South –south region of Nigeria have reported rates as high as 25.8% in children[9]. Our study rate of 6.7% is however, higher than some other studies carried out earlier such as that carried out in Kano by Sarai and Oyeyi[15], which reported a sero-prevalence rate of 4.0%, our report is also lower than that of the national sentinel seroprevalence rate of 5% reported for children in the year 2003[16]. The prevalence rate observed in our current study can be said to be expected because the overall prevalence rate observed in a general study done recently at the same site reported a rate of 11.7% in the general population[13]. This relatively high rate can be attributed to increase case detection and the fact that our center is the main referral center in Abeokuta and by extension, Ogun state receiving patients with all kinds of medical conditions. The gender distribution of HIV sero-positivity in our study reveals that females had a higher prevalence rate with 8.6% as compared to males 5.5%, there was no statistically significant difference in this variable p < 0.05 (Chi square). This kind of trend has been reported in similar studies such as, Sule et al.[8] and Sarai and Oyeyi[15]. This peculiar observation has however, not been linked to any particular risk factor such as Mother to child transmission (MTCT)[3]. It has also been previously reported that there is no association between gender and HIV exposure in infected pregnant mother[17,18]. There was also no association between age range and HIV infection in our current study, although we were not able to investigate MCTC transmission rates in our current study, previous studies have in sub-Saharan Africa has shown that MCTC remains one of the most efficient and prominent ways of paediatric HIV transmission[12, 19]. In Nigeria for instance, a recent study by Ogunbosi et al.[3] reported a 93.3% MCTC transmission rate. Although, our study revealed a slightly higher prevalence rate in the age group >5-15 years.We also investigated the monthly incidence rate of Peadiatiric HIV infection within a six month period in Abeokuta to determine the relationship between HIV risk exposure and seasonal variation. Our data revealed a steady increase in HIV infection rate from 18 per thousand in January to 154 per thousand children in May with a sharp decrease in April with 46 per thousand. Our data did not show any consistent pattern in HIV infection rate in relation to seasonality, but our data showed that there was a significant increase in infection rates during the early rainy season than the dry season. Our result is not in agreement to that of Thrustans et al.[20], which reported a higher prevalence of HIV infection among malnourished Malawian children during the rainy season, than the dry season, although their findings indicated that HIV incidence/prevalence is relatively constant throughout the year. There is no available scientific explanation to this pattern observed in our current study. Other studies have demonstrated that factors such as drought and scarcity of food can contribute to increased incidence and case detection of HIV in children owing to malnutrition[20]. A further prospective longitudinal study into the social and medical aspects of HIV infection and seasonality is suggested in this study environment.A major limitation to this study was our inability to investigate the possible transmission routes of the infected cases. In similar studies done, elsewhere in Nigeria, for example in a study by Ogunbosi et al.[3], they reported a distribution of 93.3% sreopositvity in MCTC cases; they were also able to investigate possible sexual and blood transmissible cases. This limitation faced in our study was partly due to logistic problems faced with our early infant diagnosis (EID) testing program which is still done at another referral center for HIV diagnosis as well as well as the original design of the study which was cross-sectional and retrospective. This however, serves as a window of opportunity for future researchers to investigate possible transmission routes as well as risk factors and probably the level of efficacy of current intervention measures of paediatric and infant HIV infection in Abeokuta.
5. Conclusions
- This study has shown a relatively high prevalence rate of HIV infection among children in Abeokuta. There was however, no relationship between demographic variables like gender and age range with HIV seropositivty. There was also no consistent pattern observed between HIV sero-incidence over a six month period, although it was observed that the incidence of infection was higher during the early rainy season compared to the dry months. Though, no explanation could be given to this observation, we recommend further prospective evaluation of a possible relationship between HIV infection rates and seasonal changes in Nigeria. It is also recommended that assess to PMTCT services be scaled up to arrest any chances of mother-to-child-transmission. Paediatric HIV treatment services and support should also be scaled to the local levels so as to ensure the achievement of a HIV free generation in the nearest future.
ACKNOWLEDEMENTS
- We would like to thank all the participants in this study, the efforts of the staff of the IHVN/HIV laboratory is also appreciated. The authors will also like to appreciate the effort of Miss Agunlejika Tomilola in the success of this work. The Management of Federal Medical centre Abeokuta is also appreciated for their support in the HIV/ACTION project.