-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2023; 12(1): 13-25
doi:10.5923/j.medicine.20231201.02
Received: May 20, 2023; Accepted: Jun. 12, 2023; Published: Jun. 14, 2023

Can Examination Reforms in Human Anatomy Improve Clinical Practice?
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh
Department of Anatomy, UP University of Medical Sciences Saifai Etawah, UP, India
Correspondence to: Rajani Singh, Department of Anatomy, UP University of Medical Sciences Saifai Etawah, UP, India.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Anatomy is foundation of medical education, end use of which is clinical practice to keep disease free society. Thus, Anatomical knowledge directly affects the clinical practice in diagnosis and treatment. There is concern a among anatomists and clinicians that medical trainees possess inadequate knowledge of anatomy to comprehend medical subjects and clinical practice. Umpteen number of reasons have been assigned to inadequate knowledge of anatomy. One of main cause of this inadequacy is attributed to existing examination system. The purpose of the study is to explore loop holes in present traditional examination system and to suggest reforms in it, thereby, improving clinical practice by removing inadequacy of anatomical knowledge. Literature search and authors own skill brought out the deficiency of prevailing examination system producing inadequate knowledge of anatomy and reforms to eradicate deficiencies have been proposed. Existing examination system is not only formal, routine and unfocussed on need of clinical practice but also the absence of teaching and examination during clinical phase of medical education. Therefore, the vast syllabus of Anatomy has been distributed in preclinical phase and by horizontal and vertical integration of Anatomy in clinical phase. Apart from this, reforms in scheduling of syllabus, paper setting and pattern of theory and practical examinations of Anatomy during preclinical and guide lines to syllabus and examination in clinical phases have been proposed. The Suggestions in examination reforms in Anatomy will definitely will improve knowledge of anatomy improving the safe and successful clinical practice.
Keywords: Human Anatomy, Medical Education, Clinical Practice, Examination system, Integration
Cite this paper: Rajani Singh, Can Examination Reforms in Human Anatomy Improve Clinical Practice?, Basic Sciences of Medicine , Vol. 12 No. 1, 2023, pp. 13-25. doi: 10.5923/j.medicine.20231201.02.
Article Outline
1. Introduction
- Clinical practice is the end product of medical education and the objective of clinical practice is to make disease free society. The medical education is chiefly, evolved from caring of human body against diseases thereby from Human Anatomy (HA). The causative of disease are invasion of pathogens, injury or trauma, misuse of limbs, sudden exposure to varying environmental conditions, side-effects / reactions and iatrogenic injuries creating anatomical distortions in form of break, cut, degeneration, extra growth/stones, narrowing, dilatation, thickening, thinning, blockage, dislocation, compression, variation, hematoma formation and variant attachments of tendon/ligaments and muscle fibers [1-2] in structures/organs/systems (SOS) of human body. These distortions, transform shapes, sizes, locations, orientations, branching patterns, pathways and configurations of macro/microstructures such as Vessels, Nerves, Fascicles, Bones, Muscles, Glands, Organs, Limbs and Systems constituting the organs and systems together with cascading effects on processes like altering the kinematics of organs, systems and associated activities and functions of the processes like haemo/fluid dynamics of flow through vessels/organs, two-way communication through nervous system, skeletal system of bones supporting chassis of body, muscular system providing strength supporting the activities and functions and Immune system supporting self-protection of the human body for survival. These distortions and their cascading effects impair the functions and activities of SOS creating signs and symptoms which helps in identifying the diseases through physical examination in preliminary diagnosis to estimate hidden location, identify structure in organs and systems, mapping the distortions through Surface Anatomy associated with surface markings. Further, the distortions are also correlated with impairment of functions and activities of SOS, disturbances in processes, signs and symptoms and diseases through altered morphology/morphometry keeping in mind the gross Anatomy of SOS and their variations/anomalies to confirm the disease. Later, by radiological/laboratory tests and interpretation also needs the knowledge of very precise normal/variant morphology of anatomical structures to identify distortion and to differentiate distortion from variations, anomalies and artifacts for right interpretation in final diagnosis [2]. Having finalized the diagnosis by identifying the disease the treatment analysis is carried out. During the training of medicinal treatment analysis, the action mechanism of medicines/drugs in relation to altering the functions and activities of anatomical SOS/interacting with metabolic and other processes including secretion / absorption from various glands/systems of body, is needed to teach/examine to avoid side-effects. The configuration of pathways of anatomical structures and organization of structures surrounding the distorted structure to be accessed for surgical intervention should be either revised or explained afresh and can also be demonstrated on cadaver to build more confidence in students studying Surgery. The relevant anatomical knowledge should be taught/examined. Then, the image examination and laboratory reports are to be analyzed by the clinician to keep check and balance of lapses of radiological/laboratory interpretation and confirmation of diseases. This loudly speak that the trainee students must know the above-mentioned Anatomy to take right decision in clinical analysis or he will be deemed to possess inadequate knowledge of Anatomy. But there is consensus among most of clinicians and anatomists that the clinical trainees possess inadequate knowledge of Human Anatomy to grasp other medical subjects and analysis of clinical practice [3-11]. The reasons for delivery/acquisition of inadequate knowledge of HA are absence of standardized syllabus due to arbitrary pruning, reduction of time schedule, closing of Department of Anatomy and dissection halls, filtering of experienced faculties of Anatomy, growing reduction/removal of cadaveric dissection including deteriorating examination system of preclinical phase and the absence of teaching / examination of HA schedule during clinical training of medical education. However, Much more has been said and done about all other factors to improve inadequate knowledge of Anatomy by learned authors [3-11] but little has been said about the impact, of prevailing formal unsystematic and haphazard examination system, on acquisition of Anatomy and absence of examination / teaching during clinical training of UGs, Specialties and super specialties causing acquisition of inadequate knowledge of Anatomy. “Education in general and medical education in particular, is not only learning of facts, but the training of mind to think” as aptly said by Albert Einstein. Evaluation is inextricable from an ideal curriculum which can stream line the learning process. However, it is well known fact that the examination is backbone of evaluation of ‘surface’, ‘strategic’ and ‘deep’ learning [12]. The knowledge may be inadequate, adequate and sound due to unsuitable examination system. The examination system is responsible for proper monitoring/ evaluating the ability of accumulated knowledge of HA of medical trainees. Thus, absence of a rational good examination system is one of the greatest reasons to acquire inadequate knowledge of HA. Therefore, better is the examination system and its evaluation, better will be acquisition of knowledge. But good examination system can be developed only by improving it through reforms in prevailing examination system. So, these reforms can make the examination system so better that, not to speak of, acquisition of adequate knowledge rather acquisition of sound knowledge is possible. As the degree of knowledge cultivated among the trainee medical students is monitored by examination system so, linking examination/evaluation to the learning process is a new route that ensures, not to speak of, acquiring quality and quantity of adequate Anatomy rather, standard of medical education can be raised [13] through boosting the performance of students in clinical practice. The educational environment and assessment of examination system are the only factors which influence students to adopt surface, deep or strategic learning [14]. In contrast, the students, driven by fear of failure, use ‘surface’ learning. They learn by rote with a simple aim of reproducing the material in examination. On the other hand, the students driven by recognition and encouragement through honest assessment use ‘deep’ learning to understand the meaning of contents of HA and its application in future. Students with ‘strategic’ learning are motivated on achieving higher grades and might switch between surface to deep learning methods [15-16]. This transformation in learning attitude will definitely give boost to improve the inadequate acquisition of anatomical knowledge. Thus, it is important to note here that, if the progressive and continuous monitoring of the acquisition of anatomical knowledge, by a refined rational examination system is adopted, the problem of inadequate knowledge of Anatomy can largely be taken care beforehand. Therefore, this study has been planned to suggest reforms in the examination system to compensate deficient accumulation of knowledge of Anatomy to satisfy the need of medical/clinical comprehension. The medical profession/education is aimed at providing safe and successful clinical practice which is expected to be achieved by reforming examination system as the end-use of medical education is safe and successful clinical practice.
2. Material and Methods
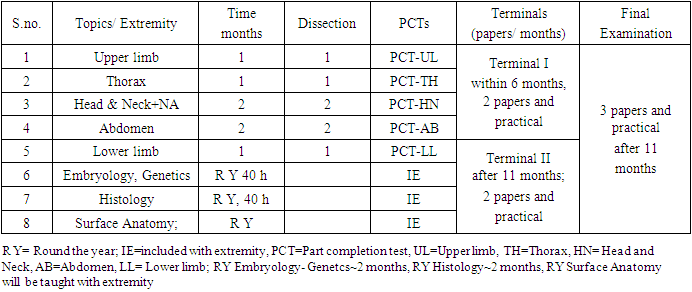
- The prevailing examination system has become traditional, formal, unsystematic and haphazard so, this is not suitable to monitor and evaluate knowledge of HA not only in preclinical phase but also there is absolutely, no schedule of teaching/examining for delivering/accumulating knowledge of HA, during clinical training of UG/ Specialty (PG)/Super-specialty (PPG) courses of medical education. However, ‘absence of a good evaluation /examination system dramatically reduces teacher’s efficiency, student’s intelligence and adequacy of resources’ [17] so, the students acquire inadequate Anatomy as the students pass the examination but do not know Anatomy. ‘Students work to pass, not to know...They do pass and they don’t know.’ as uttered by Thomas Huxley, a legendary figure [12]. So, the examination system should be fully overhauled to focus it on the accurate evaluation and monitoring of the HA in context with the need of its uses in learning the other medical subjects including safe and successful clinical analysis. The deficiencies in the examination system during preclinical phase have contributed heavily to inadequate knowledge of Anatomy to comprehend clinical practice. However, a good examination system, on the whole, depends on 1. Evaluation of comprehension of standardized syllabus of HA which should be well focused and in context with need of learning other medical subjects along with analyzing the diagnosis and treatment in clinical practice, 2. Competent faculties, who can design and develop the suitable new reformed examination system consisting of i. Scheduling of examination/tests, ii. Setting of good question papers, iii. True evaluation, iv. The honest promotion policy, in accordance with syllabus and 3. The practical/theoretical examinations consisting of examination papers focused on need based clinical applications and experiments on cadaver to be carried out by the examinee. Besides these properties to evolve a good examination system, let us analyze and compare the deficiencies of prevailing examination system to design reformations. The absence of standardized, syllabus due to pruning, experienced faculties, reduction/elimination of cadaver dissection, nonteaching/examining of variation/ anomalies and interrelationship among HA, Physiology, Pathology, Radiology, Medicine and Surgery are the main deficiencies in prevailing examination pattern. In the same continuation, the nonteaching/examining of anatomical distortions creating cascading effect on metabolic and other processes, functions and activities (Physiology) of SOS during eruption of diseases (Pathology) and mapping, identification and correlation of normal/ distorted SOS firstly, by physical examination involving Surface Anatomy and marking of gross Anatomy on surface of human body in HA then by Radiological interpretation in diagnosis and restoration of anatomical distortions in morphology of SOS through Medicines/Surgery, are another group of deficiencies in prevailing examination system. Besides, these deficiencies, there is no anatomical backup through experienced anatomical faculties during clinical training of UG / Specialty/Super-specialty courses of medical education when the application of HA in diagnosis and treatment is needed. This is another very serious deficiency in examination system. Ideally, the vast syllabus of HA should have been distributed as basic part during preclinical phase and its revision/addition for clinical applications during clinical training phase. In clinical training phase, Anatomy is referred by the words of mouth from consultants/faculties of that particular specialty or studied by the trainee himself, as such neither teaching of standard syllabus nor examination of HA is conducted during clinical phase. This is the greatest reason to acquire inadequate HA to comprehend clinical analyses. The need of scheduled teaching and examining is evidenced by BSMS model of integrated HA [18]. So, it is recommended that the clinically significant syllabus of HA should be integrated and taught/examined during clinical training. This is severest deficiency in prevailing system of education.However, in the BSMS model [18] based on horizontally and vertically integrated systemic module, a need-based HA has very nicely been planned but with some scars of weaknesses such as reduced teaching and dissection hours, piecemeal syllabus and teaching by fellow colleagues / demonstrators/tutors/ bureaucrats making irreparable damage to knowledge of HA. There is a trend of multiple-choice questions in examinations which is a hurdle to grasp the thoroughness of the subject. All these deficiencies have been analyzed in this section and reformations have been suggested.Reformed examination system of HA in preclinical phase: The objective of examination is to monitor/evaluate the accurate level of comprehension of subject and its application. Thus, analyzing the deficiencies of prevailing examination system and keeping in mind the characteristics of a good examination system as described above, the reformations are designed as under:- The syllabus of HA should be designed, developed and standardized for teaching/examination to remove the arbitrariness, variation and haphazardness of syllabus in preclinical phase crept into its examination through pruning of syllabus in various medical schools. So, the vast syllabus of HA should be redistributed partly into preclinical phase and partly into the clinical phase by integrating Anatomy, horizontally and vertically. Thus, the syllabus of HA for new examination system in preclinical phase should concentrate on basic knowledge of morphology & morphometry covering shapes, sizes, locations, orientations, branching patterns, pathways and configurations of multitude of anatomical macro/microstructures in organs or systems. The syllabus should also envelop surface Anatomy/surface markings and its morphometry with respect to landmarks, development of embryo to well-developed human being, standard histological slides, variations/ anomalies and a flying view of distortions pertaining to diseases. The examination should concentrate not merely on learning of facts rather train the mind of the students to think. So, examination should test not merely description of structures among the students rather their mind should be trained to apply this anatomical knowledge in grasping other medical subjects and clinical analysis by learning interwoven interrelation among anatomical SOS, their functions and activities, the normal/distorted SOS, their impact not only on functions and activities and eruptions of signs and symptoms of diseases, imagery analysis but also on changes in metabolic and other processes to be detected through lab. tests for diagnosis and advising treatment. As regards the faculties, no model can sustain in the absence of experienced faculties as these are the stalwarts who can appropriately give final shape and implement these examinations reformations by designing and developing the scheduling of teaching and examination/tests, setting of good question papers, guidance for evaluation and guidelines for promotion effectively. Therefore, the glimpses of salient features of planning for theory and practical examination along with the guidelines for promotion will be given here under. Broadly, this model has been adored with following features pertaining to 1. scheduling of examination/tests, 2. setting of question paper, 3. their evaluation and framing promotion strategy to evolve rational examination system. Scheduling of examination/tests: The examination schedule completely, depends on teaching schedule of syllabus covering systems/extremities/regions/topics of HA. As described above, there is no standardized syllabus, so, the examinations/tests’ schedule is also formal, depending on syllabus taught. However, removing all these constraints, the schedule of the examinations/tests has been evolved as under. There will be 5 parts completion tests (PCTs) on every taught and completed topics. The topics have been segregated into 5 extremities mixing embryology, histology, surface Anatomy and Radiology in all the extremities because the later topics are taught throughout the year corresponding to extremities. There will be two terminals on all taught topics at the interval of 6 months and Final examination after completion of full syllabus at the end of 12 months allocated after reduced schedule of HA (Table 1). The examinations of HA are conducted in two parts, 1. Theory and 2. Practical for doubly enhancing the expertise and skill.
|
3. Results
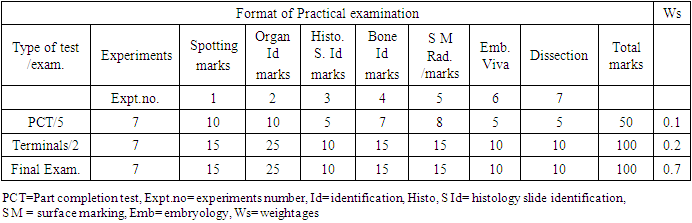
- The outcomes of standardization and scheduling of anatomical syllabus: The standardization of syllabus of preclinical anatomy has not been done so far. The syllabus of HA has been arbitrarily pruned due to reduction of schedule of preclinical Anatomy and cadaver dissection. So, different syllabi are taught in different medical institutions which indicate that the syllabi have been adopted by pick and choose methods at the free will of the institutes. This has further aggravated the situation of standardization of syllabus. That is why the arbitrary syllabus has been adopted in different medical institutions. However, the guidelines for standardization and scheduling of syllabi of HA for new reformed examinations in preclinical and clinical phases have been given in Material and methods section. The preclinical examinations have been designed as 5 PCTs (part completion tests), 2 Terminals and Final examination. The entire basic Anatomy has been divided into 7 topics, segregating into 5 extremities. This will be planned to be conducted progressively, by 5 PCTs. The PCTs will be conducted after completion of extremity. There will be 2 terminals every six months and a final examination within 12 months as currently schedule of HA has been reduced to 12 months. The schedule has presented in Table 1. The planning of examination with weightage has been done as shown in Table 2, 3. The PCTs will be having a theory paper of 50 marks followed by a practical for 50 marks. The terminals will be taken. through 2 theory papers each carrying 100 marks and a practical for 100 marks totaling to 300 marks. Final examination will consist of 3 papers in theory and a practical carrying 100 marks each totaling to 400 marks. There will be a weightage of 10% for PCT aggregates, 20% for terminal marks obtained by the students and a weightage of 70% may be given to marks obtained in Final Examination (Table 2, 3).
|

|
4. Discussion
- As already described, the upcoming medical professionals possess inadequate knowledge of needful Anatomy, so, it deteriorates safe and successful clinical practice lowering the standard of medical education. As the Anatomy is taught and examined in two episodes 1. teaching/examining Anatomy during preclinical stage and 2. teaching/examining Anatomy during clinical stage. As traditional trend of teaching/examining Anatomy during preclinical phase is delivering arbitrary syllabus of basic Anatomy with pinch of clinical applications due to reduced time schedule of Anatomy from 18 months to 12 months so, it affected the delivery of Anatomy. Apart from this, the examination system too has become formal. This has also tremendously reduced the delivery of Anatomy as it has induced the students to pass the examination rather than to grasp the subject. This has almost the paralyzed the delivery/acquisition of knowledge of Anatomy. The plight of delivery of Anatomy in clinical phase is still miserable which might have tremendously contributed to inadequate Anatomy among the clinical students ready to learn clinical analyses as there is no teaching/examination syllabus / schedule of Anatomy in this phase. This is another a big reason of inadequate Anatomy among the clinical students.However, the chief reason, for inadequate knowledge of Anatomy, is the present examination system which is a mere formality with deficiencies such as arbitrary syllabus, formal tests/ examinations’ schedule, conservative question papers, subjective evaluation and hollow promotion policy during preclinical phase of medical education and nonexistence of any standard syllabus and schedule for teaching / examination in HA during clinical phase consisting of UG, (PG) specialty together with (P PG) super-specialty courses in all the clinical streams. Although, some Applied Anatomy on the name of Clinical Anatomy is referred by word of mouth traditionally, by clinical faculties who possess remnant knowledge of Anatomy learnt during preclinical phase, of course, adored with rich experience of clinical practice which provide piecemeal anatomical knowledge. But sound anatomical knowledge along with systematic syllabus is lacking as elaborated by Cornwall, 2013 and Leveritt at al., 2016 [4,6]. ‘One of the greatest factors, for inadequate HA among the medical trainee students’, is absence of standardized syllabus and formal anatomical examination system in preclinical phase and no schedule of teaching or examination in HA during clinical training phase pertaining to UG, PG, P PG courses. Let us illustrate how this inadequacy influence the clinical practice.The clinical constraints of inadequate Anatomy: The arbitrarily, pruned syllabus of Anatomy and improper monitoring due to unsuitable examination of acquired knowledge of UG/PG/P PG students create incapability of analyzing diseases as Pathology deals with analysis of morbid structures of human body [24]. The morbidity is distortions/injury in macro/microstructures of SOS causing disturbance in metabolic and other processes, thereby, impairing of functions/activities of SOS. These impairment and imbalance of processes produce signs and symptoms of discomforts to patients as obtained via patient’s input. But the distortion in concealed organs and systems underneath skin is estimated by physical examination with the help of knowledge of surface Anatomy and surface markings, on patient input, thereon, during preliminary diagnosis. Then, the distortions are tested through imagery interpretation by comparing with normal and distorted structures and laboratory tests for disturbed processes. These analyses can be carried out only when the trainee student have clear concept of morphology/morphometry, configuration of structures with respect to functions of organs and systems of gross Anatomy including variations/anomalies, the developmental processes of SOS, the standard signature of axons and fascicles (microstructures) through histological slides, the interrelations among anatomical distortions and processes, impairment of functions/activities of SOS, signs and symptoms coupled with diseases for the specific specialties. So, if these anatomical factors are not known, the morbid structures and its impact on impairment and signs and symptoms cannot be correlated. Now, till the normal functioning of SOS are not known, the effect of morbid structure on the functions and activities of SOS including the degree of impairment of functions and activities of those SOS, cannot be estimated. This is a severe constraint in learning clinical analyses as the signs and symptoms of disease are produced by impairment of SOS and changes/disturbances in processes by distortions through action of Immune system against the threat. As, no sooner than, the structure is distorted by causative of diseases, this message is communicated by the sensory nerve network to brain, then the brain sends command to various anatomical elements (SOS and Processes) to take counter action against the threat. These create impairment, changes in processes producing signs and symptoms of discomforts in the body. This suggests that the trainee students must know the complete Anatomy along with Neuroanatomy in relation to functioning of Immune system involved with diseases of specialty. Apart from this, cascading effect on SOS and processes after medication, the functioning of the Immune system should also be taken care to avoid adverse side-effects and detailed configuration and morphology of SOS along with variations/anomalies may constraint the radiological interpretation and surgical procedure. Thus, this involved anatomical knowledge is a constraint for safe and successful clinical analyses. In the same continuation, these specialists (PGs) examine more advanced diseases so, they need disease and specialty specific advanced Anatomy, to investigate more critical cases. Such as, these trainees require the knowledge of more variations/anomalies/distortions, the specific development of SOS of the specialty, more precise comparison of normal / distorted structures (by more accurate knowledge of morphology/morphometry of SOS) in images, normal / variant/distorted microstructures in histological slides their correlation to map the pathways of fascicles [25] for repairing less invasive fascicular surgery, specific and detailed interrelations of normal/distorted structures with functions/activities of systems, processes, organs and limbs, mechanism of generation of signs and symptoms and identification of diseases, of course, for a single specialty. Though the touching knowledge of Anatomy and physiology of Immune system might have been delivered broadly, in preclinical and clinical phase of UG course, yet more detailed working of Immune system corresponding to that specific specialty is essential to analyze meticulously, the diagnosis and treatment in that specialty. If the trainee students of the specific specialty do not command above mentioned anatomical know-how, they cannot make a safe and successful clinical practice. These are again constraints of clinical practice. Further, the super-specialty medical trainees are trained for clinical analyses of more complicated and critically serious cases along with new diseases in that specialty so these trainees need more precise and deterministic diagnosis and treatment for safe and successful clinical practice. This advanced skill demands better command of involved and interwoven Anatomy together with very clear concept of functioning of Immune system for analyses of diseases during diagnosis. More Neuro/Micro-neuroanatomy is required to these trainees undergoing super-specialization in particular clinical stream. As after injury, there are two events, 1. the impact of distortion on processes, run in/by the organs, glands and systems, which are associated with working and functions of Immune system controlled by brain of the body to counter the threat, 2. The signs and symptoms of disease might be generated by neural disorders. In first case, normal but advanced diagnosis will be carried out whereas in second case, neural diagnosis should be carried out. These are the constraints faced by the super-specialist trainees. The treatment analysis also needs detailed Anatomy of organs/systems/limbs associated processes and interrelated Immune and nervous systems to estimate the adverse effect of medicine/drug and chalk out the pathway to target distorted structure for its manipulation. So, if the trainees do not possess this anatomical knowledge, their clinical analyses will be subjective, unsafe and unsuccessful clinical practice. It is pertinent to mention here that the constraints described above are in addition to basic constraints in para1 above. Elimination of inadequate Anatomy thereby clinical constraints through new examination system: As already pointed out that one of the crucial reasons for inadequate learning is obsolete examination system so, the reformed examination system has been designed to meet the challenges of inadequate knowledge of Anatomy hampering the comprehension of clinical analysis. All the constraints of inadequate Anatomy mentioned above can be compensated by well organized examination system as described in material and methods and results sections.In the new examination system, the syllabus of Anatomy has been distributed between the preclinical phase and in clinical phases consisting of UG, (PG) specialty and (P PG) super-specialty courses focusing on application of Anatomy taught, therein, under the condition of reduced time schedule of preclinical phase. However, the standardization of syllabus is to be done according to the guidelines given in this model. However, it is pertinent to mention here that the a very strong recommendation has been made to introduce necessary and sufficient teaching monitored by reformed examination system of HA by experienced faculties of Anatomy and clinical sciences in this phase of medical education. The reformations in paper setting of Anatomy and its encouraging evaluation pattern and strict promotion strategy as illustrated in material and methods section will definitely, bring sky change in comprehension of clinical practice. Let us examine, how? Such as during clinical phase in UG course, though the students might have learned the surface Anatomy, surface markings and Radiology in preclinical phase to some extent, yet the instant and timely revision and additional required Anatomy will be taught and examined through a continuous integration of Anatomy. So, while examining the patients, they will use this currently delivered knowledge of Anatomy. For example, a patient comes with a problem of sneezing and continuous flow of nasal secretion associated with headache and fever in OPD, the UGs in clinical phase diagnose as under. In such cases, patient might have been exposed to change of weather associated with sharp change in temperature by inhaling air through the nose-throat and bronchus to reach lungs for oxygenation. In this process, the surface, which came in contact with air, might have experienced cold and there would have been differential contraction (anatomical distortion) of tissues along with activation of nasal glands in this track. This might have been communicated by innervating nerves to brain as threat so it might have sent a command to take precautionary measures which might have activated various nasal glands for secretion (anatomical structures) causing flow of nasal discharge obstructing even breathing process, fever by activation of temperature center in the brain and clearing of track for any obstruction causing sneezing. The secretion and lower temperature may create obstruction in breathing and headache through other processes and system’s functioning. These appear to be caused by allergens/viral disease in throat effecting ear, nose too. Thus, such patients are prescribed specific antibiotic for throat and specific anti-inflammatory /pain killer/ antipyretic drugs which may have less or no side-effect for these anatomical structures/organs/systems in this anatomical region. The medicines are prescribed based on the severity of signs and symptoms in this viral disease.Similarly, during specialty course also, the upcoming specialists will be supplemented with disease/case specific Anatomy through vertically integrated delivery and the new examination system. Such as, during Analysis of disease, though the students already have preliminary idea of estimating distortions in corresponding SOS and their cascading effects on functions and activities of metabolic and other processes through Surface Anatomy, Surface Markings already studied in UG course yet through revising, refreshing and adding more knowledge through integrated delivery/examination of focused Anatomy, the knowledge is updated. Thereafter, the injured structure will be identified by radiological imaging/interpretation and the disturbances in processes by laboratory test results. It is worthwhile to add here that the trainee students should also learn radiological interpretation to keep check and balance over the radiological interpretation. But radiological interpretation completely depends on acquired knowledge of normal / distorted/variant morphology of SOS which will also be supplemented/examined by integrated Anatomy. As PGs specialties are deputed for patient’s investigation in OPD/wards/emergency services. If they encounter a patient with pain in right iliac fossa radiating to umbilicus, it is expected that there is inflammation in appendix. This may be due to some small seeds or any hard food particles accumulated or bacteria in appendix. This might have created anatomical distortion in the shape and size of appendix. appendix hardly affect the activities and functions of any SOS except inflammation while touching other structures. So, while diagnosing the pain by physical examination through palpating, percussing and auscultating, the diagnosis is carried out. The trainee student should be aware of surface location of this structure and its probable variations from surface landmarks to carryout physical examination further. It is pertinent to mention here that it is very difficult to image this distortion by imagery. The elicitation of signs is done by ‘Rovsing Test’. This test is completely dependent on the anatomical location, morphology and morphometry, configuration of structures in organs and systems surrounding the appendix. The left iliac fossa is pressed/palpated so, the coils of intestine come in contact with inflamed appendix which gives a feeling of pain to the patient. In normal case, Rovsing test is negative and the signs and symptoms are not elicited in case of retrocecal and pelvic appendicitis. Moreover, other causes of pain in right iliac fossa should also be kept in mind to differentiate the pain of appendicitis. The appendicitis is treated, in general, by surgery and very rarely by medicines. For surgical treatment, the surgeon needs the access path to appendix and meticulous configuration of surrounding structures to avoid any iatrogenic injury. Here in the new examination system, the questions in Anatomy to be asked from trainee students keeping in mind the testing of knowledge of HA required in their streams of clinical practice as illustrated above. Not only the knowledge of macro/microanatomy will be delivered to Super-specialists during this stage but also it will be asked in the new examination model to enhance the cognitive ability for future use. The clinical students must have the knowledge of working and functioning of body’s Immune system to master the diagnosis besides revising the involved Anatomy in diagnosis discussed in UG/Specialty courses. Furthermore, the medical students also analyze the treatment for restoration of distortions and corresponding disturbances in processes in the light of mechanism of actions of medicines/drugs and their side-effects along with side-effects created by the functions of Immune system involving Anatomical SOS. The distortions create signs and symptoms of diseases through impairment of functions / activities of SOS and disturbances in processes. This is how the disease is identified/confirmed in diagnosis. The analysis of treatment needs the Anatomy likely to be adversely affected by medicines/drugs and iatrogenic injury. This involved Anatomy may be asked in the theory /practical examinations to eliminate inadequacy of Anatomy.More advanced and critical patients approach to a super-specialist so; more meticulous HA is required for the disease to be analyzed and the treatment be prescribed. For example, typical cardiac pain is felt in the left side of chest radiating to left arm. There may be many reasons but if it is focused on cardiac disease, it may be blockage of coronary artery, valve malfunction, myocardial disorder or something else. This needs specific imagery interpretation and cascading effect on disturbed processes to be analyzed. This requires normal and variant morphology and morphometry (shapes, sizes, orientation) of heart and configured structures, branching pattern and pathways of neurovascular structures, their normal/obstructed diameters and other knowledge associated with such clinical cases in the stream of their clinical practice. If surgery is required to be carried out, the detailed access path and distorted structure and configuration of surrounding structures is to be meticulously located, mapped, identified precisely to plan surgery. If the accumulation of necessary and sufficient syllabus of HA is monitored by new examination system and found satisfactory through the questions prepared on the basis of theme of 5 types of questions as elaborated above in reformed examination system, the trainees are ready to take a challenge of grasping related medical subjects and apply HA in clinical practice. There are a few institutes in the world where a day before surgery, the surgeons and trainees are given complete demonstration of mapped access path to target distorted structure and detailed and meticulous configuration of surrounding structures involved in this surgical intervention to plan surgery This process of integration of anatomy to surgery has already been started in the University of South Florida. Regional anatomy has been taught before and during surgical procedures in the operating room [26,27]. Moreso, the procedure has been suggested to be carried out on cadavers to contain the iatrogenic injuries [2]. The questions in the examinations should be so designed that these cases should be covered in question paper with special attention to failure cases due to anatomical lapses.However, there is a very beautiful reformative decision by ‘The Brighton and Sussex Medical school (BSMS) in Great Britain’ to implement horizontal and vertical integration of Anatomy in their medical graduation course [18]. But not only the hours of dissection and teaching have been drastically reduced, but also, the teaching by demonstrators / tutors/bureaucrats/fellow colleagues and arbitrary syllabus of HA are deficiencies in this system. Whatever advanced, secured and focused on mass destruction, the weaponry be, till the soldiers do not have intuition, encouragement and zeal to fight against their enemy with the objective to defeat, it will be rather impossible to win the fight. [Dr Rajani Singh]. Similarly, the first and foremost necessity to cultivate and test the necessary and sufficient HA among medical trainees at various stages of medical education and clinical practice, is that both trainee students and both faculties should be motivated to contribute to their level best to achieve the goal of sufficient HA. If both or any of them will ignore the reformations, it will not bear fruits as sweet as needed.
5. Conclusions
- The chief advantage of reformed examination system is to remove the menace of inadequate knowledge of Anatomy to clearly understand the safe and successful clinical practice. The suggested reformed examination system coupled with strong recommendation to integrate Human Anatomy horizontally and vertically in UG/ specialty/super-specialty courses together with monitoring of adequate Anatomy through the above examination system have been proposed in this article. Thus, reformed new model of examination system will eradicate inadequate knowledge of Anatomy.
6. Recommendations
- As there is no conventional teaching and examination system of HA during clinical phase of UG, specialty and super-specialty courses prevailing in medical education so it is strongly recommended to integrate standardized syllabus of HA and an examination system as brought above.