Rajani Singh1, Fabrice Duparc2, David Gareth Jones3, Kavita Gupta4, Rahul Kumar1
1Department of Anatomy, UP University of Medical Sciences Saifai Etawah, India
2Department of Anatomy, Rouen University, 22 Boulevard Gambetta, Rouen, France
3Department of Anatomy University of Otago, Otago, New Zealand
4Department of Physiology Sri Guru Ram Rai Institute of Medical Sciences Dehradun, India
Correspondence to: Rajani Singh, Department of Anatomy, UP University of Medical Sciences Saifai Etawah, India.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The development of science and technology and population explosion with changing life style has thrown the threats and challenges to the medical education/profession, besides, the existing complexity of human body and diseases. This clearly, alarms the existing clinical practice to equip it with consistence and intensive integrated research in medical subjects in general and anatomical research in particular to combat these threats and challenges. Therefore, this study has been aimed at analyzing the involvement of grey areas in clinical practice due to lack of known/unknown Human Anatomy and research in it to improve safe and successful clinical practice. This has been done by feedback survey and literature review. The statistical mean analysis of feedback survey reveals that anatomical standalone/collaborative research is most essential. However, percentage analysis of individual subjects reveals that total population in the range of 67%-100% advocate anatomical research to be most essential, 0%-33% plead for essential and none of the subjects expressed their viewpoints for research to be not essential. In the same continuation, the literature review too brings out the knowledge gaps/handicaps of clinical practice due to known/unknown Anatomy. Thereafter, it is elaborated as to how anatomical research can minimize the handicaps by improving safe and successful clinical practice. The inference of study by both methods, namely, statistical analysis of feedback and review of literature hold the intensive integrated standalone/synergistic anatomical research high. So that, it can generate wings to clinical practice to fly high in the sky of safety and success.
Keywords:
Anatomy and clinical practice,Anatomical variations and diseases, Diseases and anatomical distortions, AnatomicalHandicaps of clinical practice, Standalone/collaborative anatomical research
Cite this paper: Rajani Singh, Fabrice Duparc, David Gareth Jones, Kavita Gupta, Rahul Kumar, Will Standalone/Collaborative Anatomical Research Revolutionize Clinical Practice?, Basic Sciences of Medicine , Vol. 12 No. 1, 2023, pp. 1-12. doi: 10.5923/j.medicine.20231201.01.
1. Introduction
There are three aspects of this study in this article, one is Human Anatomy (HA); the other is human anatomical handicaps in clinical practice and third is anatomical research to root out the anatomical handicaps in clinical practice. These aspects will be studied in the light of involvement of HA in medical education after which a clinical expert is produced. This tells the role of HA in medical education. But, clinical practice hovers around the diagnosis by examination, investigation and medication through locating and analyzing distorted structures, their impact on the functions and activities of organs and systems producing signs and symptoms of discomforts with the help of patient’s input, physical examination and imagery/lab. tests and manipulation of treatment by restoration of distortion. Thus, thorough knowledge of HA is imperative not only to diagnose the disease and manage the treatment, but also to comprehend other medical subjects. However, the clinical practice requires knowledge of all the medical subjects in general and variant gross/developmental HA including microanatomy by histological analysis of slides in particular. This speaks of our studies would be concentrating on deficiency in the knowledge of HA constituting the handicaps of clinical practice and need of anatomical research to remove these handicaps.
1.1. Human Anatomy
These handicaps of clinical practice are unknown/new variations/distortions in morphology, morphometry, configuration of structures, developmental process at gross and microanatomical level of human being and are found in 1. structures (Vessels, Nerves, Bones, Muscles……), 2. organs (Brain, Heart, lungs, livers, Abdomen, intestines, Kidney ….) and 3. systems (Nervous, circulatory, respiratory, digestive …….. systems; 11) have been addressed as Anatomical Parameters, (APs). These anatomical parameters are also distorted in shapes, sizes, locations, orientations, pathways, branching patterns and configurations which are addressed as Elements of APs, (EAPs). The variations (Vs), anomalies, (As) and distortions (Ds) are produced by invasion through antigens, injury or trauma, misuse of limbs, iatrogenic injuries and sudden exposure to varying environmental conditions creating diseases due to malfunctions of anatomical parameters [1]. The distortions (break, cut, degeneration, extra growth, stones, narrowing, dilatation, thickening, thinning, blockage, dislocation, compression, variation, hematoma formation and variant attachments of tendon/ligaments and muscle fibers variant attachments of tendon/ligaments and muscle fibers) generate not only signs and symptoms through impairment of functions and activities [2,3], but also transform or alter kinematics of organs and systems associated with activities and functions including haemo /fluid dynamics of flow of fluids through vessels/organs, two-way communication through nerves, skeletal system of bones supporting chassis of body, muscular system providing strength to support the activities and functions and many metabolic/other processes of secretion/excretion going on in human body for survival. Here, it is pertinent to mention that the nature, kind and pattern of these deformations are not fully known. These can be explored by perpetual standalone/collaborative anatomical research. The distortion is communicated by nerve network of human body so essentially the knowledge of location of deformations and corresponding innervation patterns are inevitable not only to diagnose the diseases accurately but also to know the origin of signs and symptoms. This reveals that whether the impairment has been caused by structural deformations or through neural disorders, it should be differentiated for proper diagnosis. Not only these neural elements carry the information of deformations to make the patient feel the signs and symptoms but also this neural network activates corresponding metabolic processes to repair by internal safety network of body. These metabolic processes due to distortions of APs and EAPs are either slowing down/accelerating the secretion/ absorption from glands/organs/structures or changing the contents of fluid/fluid dynamics besides the distortions may cause the spread and intensification of infection, changes in blood, urine and fecal constituents. Apart from this, the accurate locations of APs and processes from landmarks, morphology, morphometry of EAPs and APs together with variant configuration of macro /microstructures are also very important anatomical parameters to know. Thus, not only, the knowledge of naturally occurring new variations but also correlation among APs, EAPs, Ds/Vs/As of involved structures, impairments of functions/activities, signs and symptoms and diseases are very essential to accurately define the disease. Thus, besides the variations, the interrelations are also not fully known but more often form handicaps and/or knowledge gaps in clinical practice. These knowledge gaps can be bridged up by standalone or collaborative anatomical research.
1.2. The Anatomical Constraints/Handicaps in Clinical Practice
As elaborated above, the knowledge of new/ unknown developmental variations and anomalies in structures, branching patterns and configuration and corresponding neural injury or irritation caused by these anomalies modifying the functions and activities creating signs and symptoms of discomforts of diseases and are major constraints/handicaps of diagnosis and treatment during safe and successful clinical practice.It is well established fact that diagnosis depends on the interwoven interrelation among distortion in EAPs and thereby APs due to diseases in HA, the impact of distortions on impairment of APs, signs and symptoms and diseases so, the knowledge of these interrelations is imperative. Furthermore, the imagery interpretation and assessment of other transformational metabolic processes in diagnosis is another challenging area perceived as big handicaps besides, imagery being almost incapable of imaging of fascicles/axons and microanatomical distortion in these elements. The clear comprehension of distortions due to accidental trauma/injury and corresponding changes in metabolic processes are also very complicated besides, the location and types of new /unknown distortions created by new pathogens or diseases. This forms a sizable number of handicaps in clinical practice due to numerous anatomical distortions for each AP. Each distortion is likely to impair the functions in many ways terminating to multidimensional array of matrices’ relationship almost impossible to comprehend. However, it is tried to be understood case wise differential diagnosis having many ifs and buts. The analysis of the relationships of diagnosis and surgical and medicinal treatment with APs, EAPs and distortions of HA, their one to one and many-one highly complex relationship with impairment, signs and symptoms, diseases, radiological images, surgical procedures including the anesthesia and medicine prescription (Fig. 1) become, 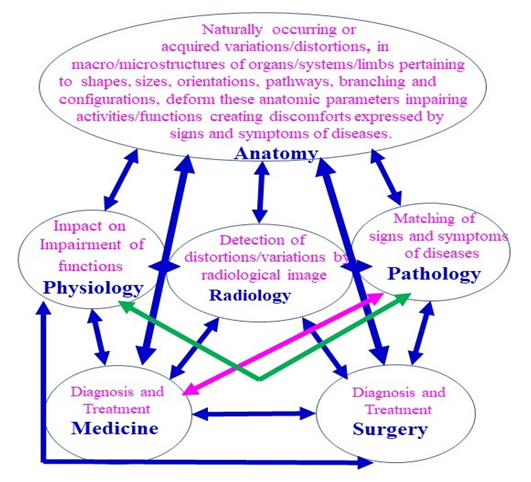 | Figure 1. Interrelation of Anatomy with Physiology, Pathology, Radiology, Surgery and Medicine |
still, complicated as it assumes highly complicated multidimensional tensor or matrix solutions as there is ever increasing chain of relation such as there are 3 APs. Each AP is having 7 EAPs. Each EAP has a fleet of Ds/Vs/As (Fig. 2). 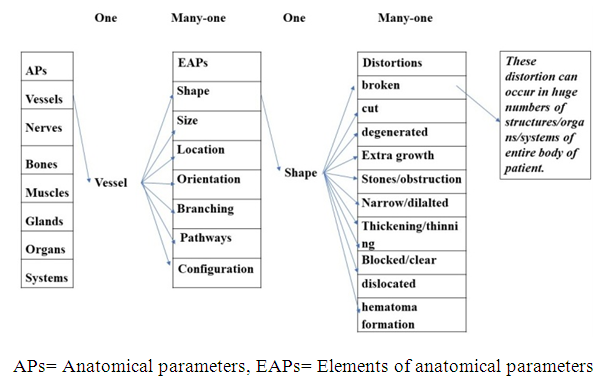 | Figure 2. Displaying Many-one relationship in APs, EAPs and Distortions |
Impairment of each distortion create different multitude of signs and symptoms and each group of signs and symptoms belong to many diseases (Fig. 3). 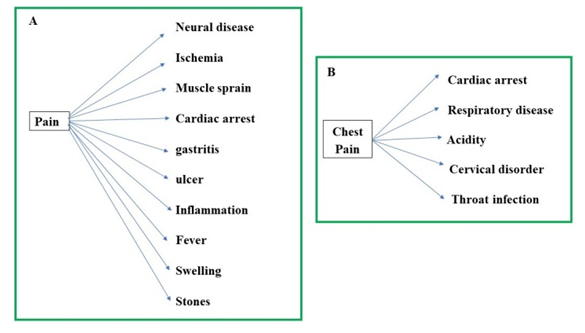 | Figure 3. A, B -Correlation of sign and symptom and diseases |
In these circumstances, the clinicians keep on doing experiments on patients’ body which many times proved to be dangerous to them. However, this can be solved only by collaborative anatomical research with relevant medical professionals including other experts if required. Apart from this, the advancement in science and technology, to facilitate clinical practice in general and diagnosis and treatment in particular, is another very important area which is also outcome of research in general and anatomical research in particular giving wings to clinical practice. Here not only very accurate and precise knowledge of Anatomy is required to design and develop these instruments but also to apply these tools by the clinicians on patients.
1.3. Research in Anatomy to Enhance the Diagnosis and Treatment Skill in Clinical Practice
In this modern world of advancing science and technology, research in Human Anatomy plays very vital and crucial role in medical profession in general and clinical practice along with HA in particular. At present, the medical education/clinical practice are not being fully updated with clinical solutions compared with the speed of emerging new variations, diseases and pathogens or otherwise in relation to distortions in anatomical structures and their interrelationship so this can be done by perpetual standalone and collaborative research in Anatomy to combat these present/future challenges by bridging up the knowledge gaps in clinical care through anatomical standalone /collaborative research.Therefore, the objective of this study is to seek feedback of viewpoints of various faculties of medical education on degree of need of anatomical research and to review literature to combat above mentioned challenges of threat/ menaces together with future challenges of medical practice for updated health care solutions through accurate diagnosis and treatment to revolutionize clinical practice depending upon the intensification of standalone and collaborative research in Anatomy.
2. Materials and Methods
To plan and design this study, it has been decided to carry out this work in two phases, namely, 1. seeking of feedback of viewpoints pleading the degree of need of anatomical research to improve clinical practice from medical faculties and 2. review of literature qualified by authors own skill, knowledge and experience. The study has used the knowledge, experience and skill of experts in various fields of medical education through published research and feedback from 13 basic scientists, 9 paraclinical scientists and 29 clinical scientists consisting of 12 Professors, 25 Associate Professors and 14 Assistant Professors totaling to 51 faculties of UP University of Medical Sciences Saifai India. For seeking the feedback, a questionnaire consisting of 15 questions targeting the degree of need of anatomical research to improve clinical practice by seeking the opinion of medical faculties has been prepared. The feedback has been assessed on the basis of model prepared on three points scale relating the viewpoints of the subjects supporting the degree of the need of standalone/collaborative synergistic anatomical research. This three-point scale in the model has been defined as anatomical research to improve clinical practice to be, 1. Most Essential (ME), 2. Essential (E) and 3. Not Essential (NE). If the opinions of individual subjects, through answers of the questions in the questionnaire supporting the need of research, are in the range of 9 to 15 (equivalent to 60% to 100%), these viewpoints represents standalone/collaborative synergistic anatomical research to be ME. Whereas the supporting viewpoints in form of answers, if culminate into 7 and 8 questions, equivalent to 47% to 53% , these are categorized as essential, E. Lastly, if the supporting answers fall in the interval of 1 to 6 questions, equivalent to 7% to 40%, these fall in the category of not essential, NE. As it is self-explanatory that the viewpoints of degree of need of individual subjects totally depends on skill, knowledge and experience of subjects and their background of HA and clinical practice so, very divergent viewpoints have been received from various divergent populations / subjects that do not lead to any meaningful inference so, to centralize the viewpoints to compare with model, 3 point scale, to assess the degree of need of anatomical research, mean and standard deviation have been computed. For making better statistical analysis to draw more meaningful conclusion, the percentage analysis has also been carried out for giving more dimensions in assessing various degrees of need of research from viewpoints. Therefore, feedback data on viewpoints has been statistically analyzed by computing means and percentages. The means, then, compared and assessed on model scale and viewpoints have been graded as ME, E, NE to conclude the degree of need of anatomical research to improve clinical practice. The permission to seek viewpoints of faculties of our institute has been taken from Dean of the institute. All participants were informed that their viewpoints were used for research work.The anatomical variations/anomalies constituting handicaps of clinical practiceIn second phase of study, it is well established fact that there are umpteen numbers of known/unknown anatomical variations/anomalies which interfere with pattern of distortions causing diseases to be restored through clinical practice enveloping diagnosis and treatment. These variations are- 1. Naturally occurring variations and 2. Acquired ones. Naturally occurring variations are genetic/developmental variations or otherwise whereas the acquired variations are caused by trauma/injury, infections by pathogens, exposure to varying extreme environments misuse of limbs and iatrogenic injuries/side-effects at gross and microanatomical levels. Partly, these are known to clinician and mostly unknown. The knowledge gaps or constraints related to unknown Variations have been analyzed.Further, the handicaps of unknown relations of disease with anatomical Vs/As/Ds in EAPs of APs and their impact on functions/activities and metabolic and other processes of structures, organ and systems creating signs and symptoms during diagnosis have been analyzed. This, has been extended to grey areas in mapping concealed distortions and cascading changes in metabolic and other processes by imagery and lab tests to diagnose the disease. Thereafter, the suitability of treatment depending on above relations and implications of macro/microsurgical intervention due to unknown macro/microanatomy have also been examined. In this process, the handicaps/lapses in imagery interpretation due to lack of anatomical knowledge of EAPs of macro/microstructures has also been investigated. The handicaps of medicinal treatment have been analyzed in the light of location and degree of distortion in EAPs of APs. The effect of organ/location specific drugs/medicines in relation to side effects/reactions is also considered. For surgical treatment, the major need of demarcation of access path to reach target distorted structure together with highly precise configuration of surrounding structures is very essential to minimize invasion due to iatrogenic injury. Before surgical treatment, the anesthesia is given for painless surgery. The variations in the configuration of nerve network are to be explored to carry out surgery, smoothly. The constraints of precise imagery interpretation for surgery, imagery guided surgery, laparoscopic surgery, endoscopy, angiography and microsurgery including proper use of upcoming new instruments applied in diagnosis and treatment will be analyzed. Tomorrows’ microsurgery too has been analyzed in view of limitation of resolution and morphology, morphometry and configuration of fascicles and axons.
3. Results
Statistical Mean analysis: The standalone/collaborative synergistic anatomical research is highly advanced and incomprehensible to common medical professional and dependent on aptitude and sufficient skill, knowledge and experience so feedback obtained, in form of viewpoints supporting the degree of need of research, is varied and diversified. Therefore, viewpoints of individual subjects do not provide meaningful inference. To obtain centralized viewpoints the mean and standard deviations have been computed so that these computed viewpoints of 3 categories of disciplinary subjects in basic, paraclinical and clinical sciences having 3 classes of faculties namely, Professors, Associate Professors and Assistant Professors have been superimposed on model three-point scale to reach meaningful inference (Fig. 4). 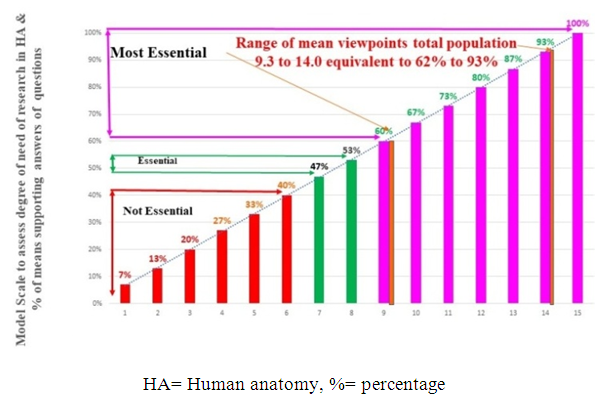 | Figure 4. Chart showing model scale for evaluation of opinions of participants |
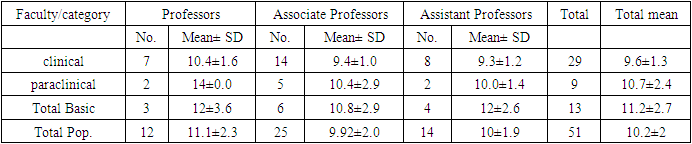
By superimposing, it is pertinent to mention here that no mean viewpoints from entire populations/subjects fall in the category of not essential (NE) and essential (E) degree of need of anatomical research. The mean viewpoints of all the above categories/subcategories of faculties, namely, ‘total population of faculties, total Clinical faculties, total Paraclinical and total Basic faculties, total Professor, total Associate Professors and total Assistant Professors, total Clinical Professors, total Paraclinical Professors, total Basic Professors, total Clinical Associate Professors, total Paraclinical Associate Professors and total Basic Associate Professors, Clinical Assistant Professors, Paraclinical Assistant Professors, Basic Assistant Professors fall in the range of 9.3-14.0 which on the model 3 point scale are in Most Essential category of supporting standalone / collaborative synergistic anatomical research to improve safe and successful clinical practice (Table 1). Besides, the viewpoints of all the individual populations separately, too present anatomical research Most essential as can be seen in table 1.Table 1. Mean viewpoints, supporting anatomical research, of all categories and sub categories of populations
 |
| |
|
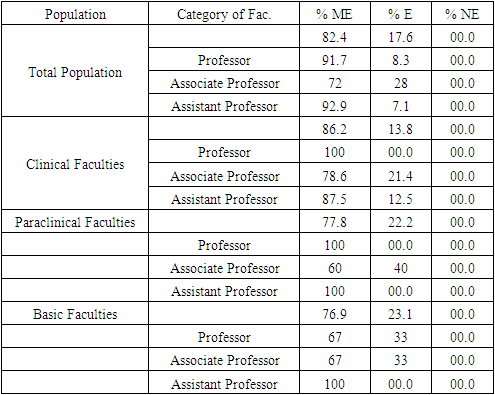
Statistical Percentage analysis: The percentages of responding populations of all the categories and sub categories of faculties, supporting various degree of need of anatomical research to be most essential, essential or not essential, has been presented in the Table 2. These data have been clearly illustrated through pie chart Figure 5 and 6. It is noteworthy here that no viewpoints of any population (0% population) advocates not essential, degree of need of research in Anatomy to improve clinical practice. However, majority of all categories /subcategories of populations as shown in table 2, plead for most essential degree of need of research in Anatomy ranging from 60%-100%. But some percentage of populations ranging from (0%-40%) put fourth their opinion for essential degree of need of research in Anatomy (Table 2). In the second part of this study, the literature survey has been carried out and following results were obtained. Table 2. Percentages of individual viewpoints supporting degree of need of anatomical research of various categories/sub-categories of participants
 |
| |
|
Handicaps of clinical Practice due to HA:The following handicaps/constraints in clinical practice due to 1A. new/unknown anatomical variations / anomalies / distortions at gross levels, 1B. The microanatomical handicaps due to variations in internal morphology of fascicles etc. 2A. Less understood interrelationship of Physiology and Pathology with HA and 2.B. knowledge gaps in interrelationship of Anatomy with Radiology and clinical sciences have been estimated in our analysis. These handicaps will be tried to be eliminated through anatomical standalone / collaborative research as illustrated below. 1A. Handicaps/constraints due to New/unknown anatomical variations/anomalies/distortions at gross and microlevels: There are enormous numbers of variations/anomalies, brought out through standalone research in Anatomy at gross level through cadaveric dissection published in Anatomical literature, some of which are not known to clinicians and the cadaveric research reveals that, still, there are umpteen numbers of variations to be discovered. The standalone research in HA on cadaver dissection continuously discover the new variations in APs and EAPs. These are naturally occurring or developmental variations/anomalies. The acquired variations/anomalies/distortions, causing diseases, are observed in EAPs and APs of patients’ body. These are tried to be detected through physical examination and imagery coupled with lab. tests. The distortions produce cascading effects on processes going on in human body for survival. These unknown variations, anomalies and/or distortions are constraints in diagnosis as well as analysis of treatment as explained above. 1B. Microanatomical handicaps in clinical practice due to internal morphology of structures: The distortions, which are found at gross level, are also present in injured internal microstructures either, or the distortions are only at gross level. The distortions, at microanatomical level, are difficult to be detected as the dimensions of fascicles or axons are beyond the resolution limit of imaging instruments. These present future challenges and threats. These distortions, in neurovascular and/or skeletomuscular structures, are either due to naturally occurring variations in EAPs of APs of human body or by acquiring through injury/infection. These are cause of concern in clinical practice. This is again very big handicap in clinical care. These handicaps described here may be reduced/ eradicated by standalone/collaborative anatomical research.2A. Handicaps/constraints due to interrelationship of Physiology and Pathology: The APs and EAPs are used in all functions and/or activities of body parts/systems to keep the human body alive and working. When APs and EAPs are modified either by distortion/injury or sometimes developmental variations/anomalies which cause impairment of functions and activities producing signs and symptoms of diseases, the unknown interrelations play very vital role constituting an important handicap throwing greater challenges in diagnosis and treatment.2B. Interrelationship of Anatomy with Radiology and clinical sciences: The identification of APs through EAPs, location of APs, location and degree of distortions/injury in EAPs and thereby in APs suffer from a big handicap in imaging and its right interpretation in presence of new and unknown Ds/Vs/As. Even this misinterpretation of imagery due to absence of thorough and accurate morphology and morphometry, the interpretation of degree of arbitrary deformation in EAPs and APs and instrument’s limitation including image defects and artifacts etc. may mislead the radiologists thereby clinician in diagnosis of disease. It is pertinent to mention here that, in normal practice, the clinicians blindly, believes the radiological interpretation report without checking the distortion and its degree. So, if any lapse from radiologist side is executed in diagnosis, this misdiagnosis may create serious clinical complications. But misdiagnosis always ends in mistreatment so, these are very critical clinical constraints. The other signs and symptoms on account of disturbance in fluid dynamics of fluid flow, in the body constituting metabolic processes or otherwise, is not fully known. So, it confuses the clinicians. These are the constraints of imagery interpretation which may also mislead the mode of treatment depending on severity of disease. However, the collaborative research in HA and imagery can improve these handicaps effectively and efficiently.If the disease has been decided to be treated by medicinal treatment to manipulate the anatomical distortions detected during diagnosis, like breaks, cuts, extra growths, stones, degenerations, narrowing, dilatations, thickening, thinning, blockages, dislocation, variations/anomalies, compression, hematoma formation, variant attachments of tendon / ligaments and muscle fibers variant attachments of tendon / ligaments and muscle fibers in EAPs of APs. After the accurate diagnosis through comprehension of relation between anatomical distortion and its cascading effect on the processes and working of APS, the physician should analyze the effect and mechanism of medicine/drug on the basis of location of APs and their functions for manipulation of distortion reducing the discomfort and disappearance of signs and symptoms keeping in mind the metabolic processes, absorption and secretion of biochemicals and other functions and activities of APs. For this, the clinicians should have thorough knowledge of APs so that these be monitored time and again during treatment. If the surgical treatment is decided to manipulate the distortion in question, it requires greater precision of interpreting images pertaining EAPs of APs and access route and accurate identification of structural configuration of APs in the vicinity of distorted structure which, in turn, can only be successfully, done with the help of comparing normal image from cadavers coupled with dissected real structure with the distorted image of live patient as explained in preceding sections. Before surgical intervention, anesthesia is given by nerve blocking for painless surgery. For this, the entire local nerve network and innervation pattern should be known to anesthetist or it has to be interacted with an anatomist in general or neuroanatomist in particular or it can be achieved by collaborative anatomical research synergizing with anesthetist, surgeon and anatomist. The entire process of surgery will be done more confidently if the imagery interpretation and surgical intervention are carried out on cadaver prior to real surgery. This again is part of synergistic collaborative anatomical research. The above elaborated handicaps/knowledge gaps/grey areas, about unknown anatomical variations/distortions and their interrelationship, can be solved either by standalone or collaborative research in Anatomy with Physiology, Pathology, Radiology, Surgery and Medicine for drastic improvement in clinical practice.
4. Discussion
The advancement and growth of any science depends on research and its applicability to make it applicable in new areas of human facility so, is the case with medical science to be used for health care in general and clinical care in particular. It is pertinent to mention here that clinical care for diseases is always associated with examination of human body whose structures are used in processes to keep human alive. Therefore, human anatomy is the chief subject to be mastered for successful clinical practice. As regards research in anatomy, in this world of changing environment, advancing science and technology influencing food habits and life style, the clinical complications increased multifold so to combat with this menace, research, in all the medical subject in general and HA in association with clinical practice in particular, has become indispensable. Thus, degree of need of research, to improve clinical practice, has been studied by two methods, namely, A. Obtaining feedback from skillful, knowledgeable and experienced medical faculties grouped in Professors, Associate Professors and Assistant Professors in three fields, 1. Clinical, Paraclinical and Basic sciences and B. By literature review/analysis with authors own skill, expertise, knowledge and experience.As described above, the feedback data has been collected from the clinical/non-clinical faculties based on the answers of 15 questions in questionnaire regarding degree of need of anatomical research to improve clinical practice. The study has been carried out under two heads namely, mean analysis and percentage analysis. The degree of need of anatomical research has been graded on a 3-point scale depicting degrees as ME, E and NE.Mean analysis: 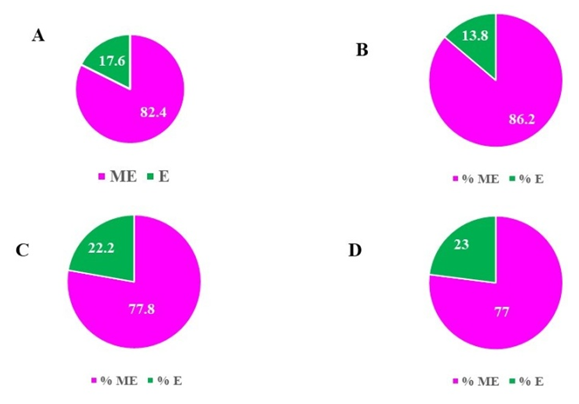 | Figure 5 |
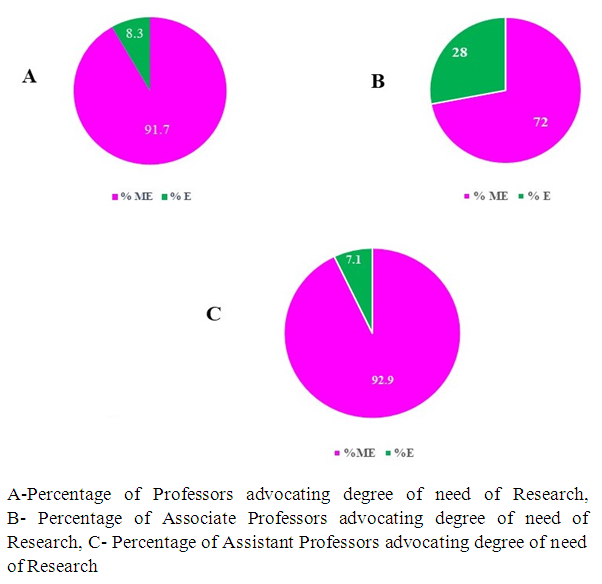 | Figure 6. Pie diagram showing percentage analysis for degree of need of Anatomical research advocated by professors, associate and assistant professors |
The mean viewpoints have directly been superimposed for comparison on the model scale and inference has been tabulated in Table 1. The mean viewpoints of all the categories/sub-categories of populations, such as, ‘total population of faculties, total Clinical faculties, total Paraclinical and Basic faculties, total Professor, total Associate Professors and total Assistant Professors, total Clinical, Paraclinical and Basic, Professors, Associate and Assistant Professors, separately, fall in zone of ‘ME’ ranging from ‘9.3±1.2 to 14±0.0 (Table 1) on the model scale (Fig. 5). The responses of broad groups of Total faculties, clinical, paraclinical and basic faculties have been found in the range of 9.6±1.3 and 11.2±2.7 which again advocate for ‘ME’ degree of anatomical research. Whereas the mean viewpoints of ‘Total Professors, Associate Professors and Assistant Professors’ fall in the range of 9.92±2.0-11.1±2.3 revealing research to be ‘ME’ to improve clinical practice. However, the mean viewpoints of Total population have been found to be 10.2±2 which clearly, establishes the ‘ME’ degree of need of anatomical research. Detailed mean viewpoints of all sub-categories also present ‘ME’ degree of need of research can be seen in Table 1.To add value to statistical analysis, percentage analysis (Table 2) reveals that 82% of total faculties individually, express their viewpoints on research to be ME, 18% essential (E) and none as not essential (NE) for improving clinical practice. 92% Professors, 72% Associate Professors and 93% Assistant Professors advocate anatomical research to be ‘ME’ whereas 8% Professors, 28% Associate Professors and 7% Assistant Professors plead anatomical research to be essential but none says NE. 86% of clinical, 78% of paraclinical and 77% of basic faculties express their views for research in HA to be ‘ME’ whereas 14% clinical, 22% paraclinical and 23% of basic faculties plead for the research to be essential without any score for NE. In clinical field, 100% of Professors, 79% of Associate and 88% of Assistant Professors; in paraclinical streams, 100% Professors, 60% Associate and 100% Assistant Professors and in basic sciences, 67% of Professors and Associate Professors including 100% Assistant Professors pleaded for research in HA to be ME. Thus, 33% of basic Professors and Associate Professors supported research in HA to be essential. This data as described above has been presented by pie charts in Figure 5 and 6. However, none of the faculty have viewpoint for research to be not essential. More so none of clinical, paraclinical Professors and none of paraclinical along with basic Assistant Professors advocated research in HA even essential li.e. all these advocate research in HA to be most essential (Table 2). Constraints/handicaps of anatomic variations in clinical practice:As every human being is anatomically different from one another, so, the EAPs, thereby, the configurations of APs, have large numbers of variations. These variations sometimes create discomforts expressing signs and symptoms and many times these are asymptomatic. The symptomatic variations create diseases. As the APs are used in carrying out the functions and daily activities of human being so, when these APs are distorted by variations, these restrict or constrain the functions/activities of APs of body. Thus, the distortions of both, EAPs and APs, produce impairment of the functions and daily activities with expression of discomforts through signs and symptoms. The distortions, as a threat, are communicated by nerve network to brain which, in turn, activates the inbuilt self-protection system of body creating more signs like altering the secretion or absorption pattern of glands and/or organs, digestion, urinary activities, neural communications and the hemodynamics/fluid dynamics of fluids present in the body deregulating metabolic processes as cascading effects (personal communication). The distortions are examined by physical examination first, based on patient’s feedback thereafter the structure/ organ is identified and accordingly the imagery is advised. But as all the variations, causing problem, is unknown so, the imagery expert may interpret it normal. Based on imagery interpretation, the clinician also, in the absence of knowledge of variations, does not, usually, cross examine the radiological report and the patient is prescribed medicine on the basis of signs and symptoms suppressing the discomfort. The medicine/drug, many times, does not provide relief due to misunderstood original problem of patient rather, it introduces side-effects. Because the structure/organ was considered normal so the cascading effects of the variations are not investigated which could have elicited the signs and lab. test for the same would have been advised. Later on, the complication becomes unmanipulable together with side-effects. This is a great problem. This sends clear message to clinical analyst that detailed clinical significance of every discovered new variation, should be brought out for the future reference of clinicians. This conveys that not only intensive and integrated standalone anatomical research can bring out such hidden unknown variations but also the variations discovered by anatomists should be passed on to clinicians either, or a skilled anatomist should be attached with clinician while performing diagnosis. If these variations are not known to clinicians, they may confuse and misdiagnose the disease. So, these unknown variations are real handicaps of diagnosis and greatest challenge to clinical practice. These handicaps can be removed by standalone/collaborative cadaveric research in HA. This will make the clinical practice smoother. Constraints of complex interrelationship among Anatomy / Physiology / Pathology: “Where there is a disease in human body, it is due to an anatomical distortion so Anatomy is associated to it” [3]. Therefore, basic approach to diagnose and treat the diseases should be to restore the distortions. The traumas, injuries, pathogens, environmental hazards, congenital anomalies and iatrogenic injuries/side-effects are main causatives of diseases creating distortions/injuries in corresponding APs, which produce signs and symptoms of discomforts in patients. So produced distortions not only generate impairment in the functions and activities of distorted APs but also disturb the equilibrium effecting the working of corresponding APs like regulatory mechanism of secretion processes by organs and glands, the oxygenation of blood, metabolic processes of food intake, regulated blood circulation process etc. running in the body to keep it alive and working. Let us elaborate, how? As soon as the APs are distorted, the communication system of human body instantly convey the threat message to brain which, in response, simultaneously, make the body feel the discomforts and so activate the protection mechanism through self-protection system by issuing a command to APs meant to take safety measures to combat the threat. This command not only generate signs and symptoms of discomforts due to impairing corresponding APs but also create signs by altering kinematics of metabolic or other large numbers of processes of APs. These actions happen through very complex interrelationship between various stages of disease process, distortion and impairment of functions. Therefore, the clear comprehension of these relationships is essential. Whatever be the claim, but these are less understood and interwoven with Anatomy, Physiology and Pathology. This can be understood by the fact that 1. the signs and symptoms and disease have matrix many one relation, means same signs and symptoms are observed in many diseases (Fig. 2) so the assessment of disease is subjective based on purely signs and symptoms, 2. There are large numbers of structures and organs and systems (APs) along with multitude of EAPs associated with enormous numbers of naturally occurring and acquired Ds/Vs/As and 3. So, there are huge numbers of impairments (Fig. 3). Therefore, the interrelation among these subjects is incomprehensible and can be thoroughly understood either by synergizing the clinical practice or at least associating the standalone and collaborative anatomical research. Thus, the real causes, of diseases thereby signs and symptoms, are anatomical Ds so it is essential to correlate the anatomical Ds with its impact on impairment of functions and activities including signs and symptoms and diseases. Anatomical Ds/Vs/As are only partly known that too, physicians are not updated with these known factors so this is very serious handicap of clinical practice. Collaborative research is the solution.Anatomical handicaps of clinical practice consisting of diagnosis and treatment: Diagnosis: The clinical practice starts from the patient’s feedback of his discomforts in terms of symptoms of disease in his body. As explained above, the diseases are nothing but invasion of causatives which distorts/modifies the specific APs through EAPs. These distortions, in turn, modify the functions and activities of these APs together with disturbing the equilibrium of metabolic or other processes generating signs and symptoms of inconvenience. Thus, the root cause of the disease are the distortions of anatomical structures, therefore, the basic approach to diagnose the diseases and prescribe treatment remain to restore these distortions and to remove the cascading effect on the processes. So, as already explained, the entire process of medication rests on investigation and restoration of anatomical distortions in shapes, sizes, locations, orientations, branching patterns, pathways and configurations of structures, organs and systems. The anatomical knowledge pertaining to morphometry of morphology of EAPs and APs to investigate the distortion and analysis of treatment to restore the distortion as far as possible without side-effects should be applied. Therefore, as illustrated above, the diagnosis and treatment, the chief constituents of clinical practice, cannot be precisely analyzed without sound and advanced knowledge of HA either, or anatomical standalone and/or collaborative research for unknown anatomical variations/constraints of clinical practice. This is illustrated below.The feedback obtained from patient consisting of family history to comprehend genetic/developmental disease/ variation, causative of discomforts to estimate nature and type of distortion whether it is due to infection etc. and chronology of disease to assess the gravity of disease. As explained above, the discomforts are the outcome of anatomical distortions so, the clinician enquires the patient the location of discomforts to locate probable distorted specific APs. For this, the examination of patient’s body is carried out through observation, palpation, percussion and auscultation [4] based on the knowledge of normal human body from cadaver consisting of ‘Organization and development of EAPs of APs in normal human body, functions and activities of APs and EAPs and metabolic and other processes running in body’ and impairment of functions and activities of EAPs in APs. Thus, firstly, these distortions are to be identified in modified structures, detected, located and mapped. So, the clinician locates the spot and estimate the presence of concealed distorted structure and degree of injury by physical examination of patient’s body and analyze the transformations of metabolic processes through location of distortion in structure and analyzing the interrelationship of kinematics of the structures with activities and functions and dynamics of fluid flowing in related structures to comprehend and relate signs and symptoms with disease. This information helps in eliciting the signs while analyzing the disease. This estimation of anatomical distortions and their cascading effect in other processes in the body of patient will enable the clinician to advise the imagery and lab. tests to confirm the disease. If this information is unknown to clinician, this is a clinical handicap. Either it is to be interacted with skilled anatomist or anatomical research in collaboration with clinician, radiologist, physiologist, and pathologist will uncover the solution. Constraints of Imagery: As the cure of disease is related to restoration of distortion so, it is not merely, the accurate identification of distorted APs at the right location and signature of distortion/injury to be imaged and mapped, rather, it is, configuration of the distorted structure among the surrounding structures in organs/systems and access path, to be clearly brought out. However, there is sky difference between images and real APs and that too, this information depends on radiological mapping and interpretation where lot many processes involved in imaging and interpretation of images with defects introduced by instruments including resolution, edging effect and artifacts together with subjectivity in interpretation. So, completely and exclusively, depending on imagery may be disastrous. Routinely, from imagery interpretation, the APs and distortion/injury therein are identified by comparing the images of EAPs of APs of live patient with knowledge of real EAPs and APs from cadaver on the basis of precise knowledge of their morphology and morphometry. The presence of unknown variations in EAPs and configuration of APs, many times, confuse the radiologist in identifying image of real APs and distortions therein. Thus, the interpretation of these images, due to unknown variations and under machine limitations, are serious constraints of image formation and interpretation. This invites a big uncertainty which may even distort the diagnosis so treatment jeopardizing the health of patient. So, this again is a big constraint /handicap. The uncertainty, as described above, will not only lead to misinterpretation of images but also may alter the thinking process of clinician regarding the diagnosis of disease. Besides, many times, it has been heard that the imagery is normal but, in that case, in place of leaving the patient suffering from existing problem, the injury to nerve network related to particular AP should be analyzed as the feelings of signs and symptoms are generated by communication through nerves. Thus, the nerve network and innervation pattern either should be known or should be discovered by synergistic anatomical research.These are very crucial constraints in diagnosis through imagery. But these can be improved by extracting EAPs of APs from cadaveric dissection and the images of normal APs of cadaver may also be taken thereafter the images of the same structure of AP from cadaver and the images of real distorted structures of AP of patients should be compared for more precise interpretation and evaluation of distortion. Whatever it is, in all cases, HA is to be analyzed more precisely. However, many things in these distorted/normal anatomical parameters are known and many things unknown so, unknown can be discovered through collaborative research in HA. After imagery interpretation with accurate knowledge of distortion in AP, the clinician analyzes cascading effects of distortions on metabolic processes disturbing the functions and activities of APs like change in absorption/secretion, fluid dynamics, contents of fluid etc. for confirmation by lab. tests for eliciting the signs. This will require the knowledge of interlinked Anatomy. But partly it is known and partly unknown so research will bring out the clear picture. “The ever-expanding array of newer diagnostic methodologies, including the innovations, in the way, the body can be visualized (e.g., computed tomography, magnetic resonance imaging scans), require a specific level of anatomical knowledge” [5]. Besides this, the imagery interpretation becomes more complex during imagery guided surgery, microscopic surgery like endoscopic, laparoscopic and micro-neuro surgery needs more precise Anatomy for successful clinical practice [6]. These constraints can be taken care by synergistic research in Anatomy.Apart from this, the recording and interpreting microstructures like fascicles and axons are still a challenge as the diameter of fascicles (200-800) micron [7] and diameter of axons (0.1-10) micron [8] whereas injury on these structures is smaller than the diameters. The imaging of these structure along with injury thereon are beyond resolution limit of high-resolution MRI (2000 micron). However, these distortions/variations/anomalies can be detected by high resolution MRI scanning coupled by color coded frequency analysis as claimed by Baumer et al. 2012 [9], Chhabra et al. 2013 [10]. But these anomalies or variations can definitely be detected by high resolution MRI and histological slides and their correlations [11,12]. Therefore, such handicaps may be overcome by synergistic anatomical research. Having analyzed the severity of disease through degree of distortion, risk of life through manipulability of disease, by either treatment whether medicinal and/or surgical, is decided. The medicinal treatment and surgical treatment separately, will be examined for constraints and their viable solution. Let us examine both these treatments separately.Handicaps of Medicinal treatment: As root cause of the disease has been established to be the anatomical distortions, so, this treatment should be focused on manipulating the anatomical distortions, corresponding to the diseases, such as, ‘broken Shapes, Cuts in shapes, degeneration, extra growth, stones, narrowing, dilatation, thickening, thinning, blockage, dislocation, compression, variation and/or hematoma formation’ in EAPs of APs. These anatomical distortions are not only analyzed in Vessels, Nerves, Bones, Muscles, Glands Limbs and Systems depending on signs and symptoms, but also the cascading effects of distortions on metabolic processes disturbing the functions and activities of APs like changes in absorption / secretion, flow dynamics, fluid contents of fluid etc. such that organ wise, system wise and location wise sensitive newly discovered molecules of medicines/drugs may be prescribed with minimum side-effects.Handicaps of Surgical treatment: The handicaps of diagnosis discussed above are common to medicine and surgery both. Other handicaps, specifically, for surgery are 1. Explicit pathway to access safely, the targeted distorted structure for surgical manipulation together with precise EAPs of anatomical macro/micro surrounding structures encountering in the way to avoid iatrogenic injury, 2. The precise location and identification of EAPs of targeted distorted structure and organization of surrounding structures, 3. The morphometry of the structures from cadavers w.r.t. landmarks, 4. The perfect identification of nerve network including structure and organs for nerve block by anesthesia and 4. Healing medicines and drugs.Before going for surgery, anaesthetist is to analyse the situation to find which kind of anaesthesia, local or general is to be given by blocking the specific nerve to facilitate painless surgery. For this, the source is radiological images. This is very dangerous procedure because a small lapse can lead to very grave consequences. Therefore, it requires not only thorough knowledge of macro/microanatomy of nerve network, but also standalone/collaborative research in Anatomy synergising with anaesthetists and surgeons. The precise identification of distorted structure is highly essential together with its configuration wrt surrounding structures and morphometry of EAPs and APs and their location with respect to prominent landmarks. Additionally, the demarcation of access path is equally important to avoid any unwanted iatrogenic injury to access the target distorted structure. These data are derived from imagery interpretation which is to be cross checked by surgeons. As described above, for the precise imagery interpretation, it should be done synergistically with an expert anatomist. However, more safe and successful surgical manipulation can best be carried out more confidently by experimenting the entire exercise of surgery on cadaver first. The surgical treatment requires the access path through structures encountering while reaching to the distorted organs for repairing / grafting / manipulating so, in presence of variations in surrounding structures may end up in iatrogenic invasions. This is a big grey area. These gaps can be bridged up only by collaborative research in Anatomy and pathology / radiology / surgery/ medicine. As in many countries of the world, there is practice that before surgery day, the entire procedure is discussed and analysed before with anatomist as elaborated. Apart from this, the best practice would have been if the entire surgical procedure is exercised on the cadaver. Further, as regards manipulation of structures in imagery guided surgery, the calibration of radiological images is essential to avoid surgical errors due to limitations of image formation and interpretation. During imagery guided surgical intervention, the surgeon must calibrate the tip of surgical instrument w.r.t. in situ location of APs in imagery screen so there should be coherence and coincidence of imagery and real surgical intervention. Or there is a chance of iatrogenic injury [6].In laparoscopic procedures, very accurate morphology and morphometry of the anatomical structures and their configuration should be investigated to chalk out accurate access path to reach and manipulate the target distorted structure safely and without enhancing the invasion. With the advent of laparoscopic and micro-neurosurgery together with imagery guided surgery, “the augmented importance of endoscopic and laparoscopic procedures demands more meticulous macro/microstructural clinically orientated anatomy” [6] to be associated with collaborative research. There is a large grey area/knowledge gap to be patched up by research in these fields. Handicaps of surgery of microstructures: In case of human anatomical microstructure manipulation by microsurgery, the chief handicap of radiologic instrument is its resolution limitation. As the high-resolution MRI (with high intensity magnetic field) has minimum resolution of 2 mm (2000 micron) as the sections of Anatomical structure in MRI can faithfully be viewed minimum at 2mm interval. So, any structure, of size of 2mm, can only be viewed faithfully in high resolution MRI. Therefore, anatomical structures or injuries, of size less than 222 in any dimension, cannot be imaged faithfully not to speak of its interpretation. However, interpretation of images of microstructures can be improved by microscopic cadaver dissection and imaging of that microstructure and then comparing it with real images through High resolution MRI. Besides, to map such structures/injuries less than 222, the histological technique can be used with the help of high- resolution MRI from same cadaveric structure [11]. So, in case of microsurgery, not only the anatomy of the nerve but also its internal morphology “is vital to develop rational bases for repair and development of engineered constructs” [13] as “varying degree of fascicular injury allows possible replacement of individual fascicles as opposed to the entire injured nerve and more reasonably explains the formation of neuromas in situ” [13]. “Despite our best efforts in nerve repair, full functional recovery is seldom achieved. Motor nerves tend to be more refractory than sensory to full recovery” [14]. But, “clinical practice in neuropathy is very complex as Woodhall and Beebe (1956) [15] noted nerve repair rarely restored function greater than 50% for the median nerve. Other nerves demonstrated poorer functional recovery”. These things happen due to grey areas/knowledge gap of shapes, sizes, locations, orientations, pathways and configurations of fascicle/nerve fibers. As explained above, the imagery constraints introduce lot of uncertainty in images and their interpretation of fascicles so the surgery becomes not only dangerous but also recovery is reduced due to lack of end-to-end matching of number and size of fascicles. However, On the same lines, Singh et al. 2019 [11] have also carried out the mapping and correlation of fascicles of femoral nerve cropped from a cadaver and prepared histological slides to facilitate diagnosis and treatment by repair/grafting/regeneration at fascicular level. If this is blended with high resolution MRI, it will solve this problem of microscopic end to end matching effectively.The detection of these parameters, for diagnosing and treating the injuries in general and neurological treatment by medicines and micro-neurosurgery for repairing / grafting / regeneration of injured fascicles/nerve fibers in particular, are essential for non-invasive procedures and better recovery. As regards microanatomical research to unearth the variations like orientations, locations, pathways, branching patterns and configuration at fascicular level in neurovascular, muscular and bony structures, these can be explored by tissue collection from cadaver and preparing histological slides and correlating these slides to know complete picture in relation to location, EAPs and APs [16]. As Anatomy could not be developed as an essential subject of medical education [17,18] so, it pits Anatomy against the excitement of the rapidly moving disciplines, such as virology, genetics and molecular biology. They are rapidly moving but to place all the stress on them to improve clinical disciplines is hazardous as these subjects can provide better results if these are taught and developed by medically qualified anatomists. Apart from this, as wide spectrum of diversification in variations, anomalies or distortions in anatomical EAPs of APs and corresponding impairment of functions and activities, new discoveries in pathogens/antigens and their mode of invasions in APs producing diseases and, the innovations in imagery equipment, the discovery of new and advanced specific molecules based on structures, organs, systems and locations and with development of science and technology, more focused and based on specific injury and/or injured micro-structures to be repaired / grafted / replaced / removed by the surgical interventions, are major threats and challenges of tomorrows’ medical profession. To combat with these threats, intensive, integrated and synergistic standalone and collaborative anatomical research for safe, successful and smoother clinical practice is most essential.
5. Conclusions
The mean analysis of feedback data establishes that the total population expressed their opinion on need of degree of standalone/collaborative anatomical research is most essential to improve safe and successful clinical practice. The categories and subcategories separately, also support the above inference.The percentage analysis reveals that none of the faculty expressed viewpoints for not essential degree of need of anatomical standalone/ collaborative research. More so none of clinical, paraclinical Professors and none of paraclinical along with basic Assistant Professors advocated research in HA even essential not to speak of not essential in percentage analysis. However, separately, in various populations, majority more than 67% advocates most essential whereas some (maximum 33% in one category) support the research to be essential. The disease is caused by anatomical distortions impair structures/organs/systems of body producing signs and symptoms which in turn, create imbalances in the cascading effects on metabolic processes disturbing the functions and activities of APs like changes in absorption/secretion, flow dynamics, fluid contents of fluid etc. All this put together help in diagnosis and treatment. All these things are related to known/unknown Anatomy so, the anatomical standalone/collaborative research is indispensable for improving safe and successful clinical practice. Thus, the inference is that yes, research in Anatomy will not only improve the clinical practice rather this will combat the future challenges and threats of clinical practice.
ACKNOWLEDGEMENTS
No funding has been received from any agency.Conflict of interest: None
References
| [1] | Singh R, Shane Tubbs R, Gupta K. et al. (2015) Is the decline of human anatomy hazardous to medical education / profession? A review. Surg Radiol Anat 37 (10): 1257-65. |
| [2] | London DA, Andelman SM, Christiano AV, Kim JH, Hausman MR, Kim JM (2019) Is Wikipedia a complete and accurate source for musculoskeletal anatomy? Surg Radiol Anat 41(10): 1187-1192. doi: 10.1007/s00276-019-02280- Epub 2019 Jul 1. |
| [3] | Singh R, Yadav Nisha, Pandey Manisha, Jones DG (2022) Is inadequate anatomical knowledge on the part of physicians hazardous for successful clinical practice? Surg Radiol Anat https//doi.org/10.1007/s00276-021-02875-7. |
| [4] | Standring S (2012) Evidence-based surface anatomy. Clinical Anatomy 25:813–5. |
| [5] | Priyadharshini NA, Dinesh Kumar V, Rajprasath R, Rema Devi (2019) Relevance of Learning Anatomy to Clinical Practice: Perceptive of Medical Students, Interns, and Clinicians. Natl J Clin Anat 8: 32–37 DOI https://doi.org/10.1055/s-0039-1688893 3. |
| [6] | Barlow, DH (1981) On the relation of clinical research to clinical practice: Current issues, new directions. Journal of Consulting and Clinical Psychology 49(2): 147–155. https://doi.org/10.1037/0022-006X.49.2.147. |
| [7] | Choi AQ, Cavanaugh JK, Durand DM (2001) Selectivity of multiple-contact nerve cuff electrode: A simulation analysis IEEE Trans. Biomed. Eng 48(2): 165-172. |
| [8] | Perge JA, Niven JE, Mugnaini E, Balasubramanian V, Sterling P (2012) Why do axon differ in caliber? J Neurosci 32: 626-638. |
| [9] | Bäumer P, Heiland S, Bendszus M, Pham M (2012) MR neurography – Diagnostic criteria to determine lesions of peripheral nerves. Magnetom Flash (Suppl. 2):10-4. 2012. |
| [10] | Chhabra A, Zhao L, Carrino J A et al (2013) MR Neurography: Advances Radiol. Res. Pract 2013: 809-568. |
| [11] | Singh Rajani, Raj Kumar, Naresh Chandra, Kavita Gupta, MS Ansari (2019) Microanatomy of nerve to iliacus and its clinical significance. Int J Morphol 37 (3): 1150- 1163. |
| [12] | Singh Rajani (2020) Microanatomy and clinical significance of cutaneous nerves of thigh. Basic Sciences of Medicine 9(2): 15-23. |
| [13] | Evans Gregory RD (2001) Peripheral nerve injury: A review and approach to tissue engineered constructs. Anatomical Record 263: 396-404. |
| [14] | Mitchell SW, Morehouse GR, Keen WW (1864) In gunshot wounds and other injuries of nerves. Philadelphia: JB Lippincott. |
| [15] | Woodall B, Beebe WG (1956) In peripheral nerve regeneration: A follow-up study of 3,656 World War II injuries. VA Medical Monograph. Washington, DC: US Government Printing Office. |
| [16] | Chandra Naresh, Rajani Singh (2019) Tracking of Fascicles of Sartorius and Pectineus Nerves-A key to Neurosurgery. Journal of Clinical and Diagnostic Research 13(1): AC01-AC08. |
| [17] | Singh Rajani, DG Jones, Raj Kumar, Naresh Chandra. (2021) Will Development of Human Anatomy Revolutionize Medical Education? Basic Sciences of Medicine 10(1): 10-18. |
| [18] | Turney BW (2007) Anatomy in a Modern Medical Curriculum. Ann R Coll Surg Engl 89(2): 104-107. doi:10.1308/003588407X168244 PMCID: PMC196455 PMID: 17346399. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML