-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2022; 11(1): 5-15
doi:10.5923/j.medicine.20221101.02
Received: Sep. 4, 2022; Accepted: Sep. 16, 2022; Published: Sep. 23, 2022

Why Should Anatomy not be a Clinical Subject? -An Analysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh1, David Gareth Jones2, Fabrice Duparc3, Kavita Gupta4
1Department of Anatomy, Uttar Pradesh University of Medical Sciences, Saifai, Etawah, UP, India
2Department of Anatomy, University of Otago, Otago New Zealand
3Department of Medicine, Rouen University, 22 Boulevard Gambetta, Rouen, France
4Department of Physiology, Subharti Medical College Dehradun, UK, India
Correspondence to: Rajani Singh, Department of Anatomy, Uttar Pradesh University of Medical Sciences, Saifai, Etawah, UP, India.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Human Anatomy is the science of all the macro/microstructures of human body. These structures are invaded by trauma/infection causing partial/full impairment of functions/activities of these structures producing signs and symptoms of diseases. The recovery from these diseases is done in clinical practice after studying the basics in medical education. Thus, neither medical education can be mastered nor clinical analysis carried out without sound knowledge of Anatomy. Consequently, Anatomy, medical education and clinical practice have an interwoven interdependent interrelationship among them. Hence, where there is clinical practice, Anatomy is associated with it. Therefore, this study has been designed to argue for Human Anatomy to be recognized as a clinical subject. The need, utility and applications of Human Anatomy/clinical Anatomy in medical education and clinical practice has been explored through literature search and argued as to why Anatomy should be a clinical subject. As there is intimate relationship among medical subjects and clinical practice, the teaching of human anatomy should be continued throughout all stages of medical education and clinical practice. Disease is caused by anatomical distortions/variations, and these, in turn, impair the functions and activities of affected structures. Impairment produces signs and symptoms of discomfort causing disease. As a result, it is argued that this makes Human Anatomy essential not only in medical education but also in clinical practice. In other words, there is a case for treating Human Anatomy as a clinical subject.
Keywords: Applied Anatomy, Distortions, Impairment, Diseases
Cite this paper: Rajani Singh, David Gareth Jones, Fabrice Duparc, Kavita Gupta, Why Should Anatomy not be a Clinical Subject? -An Analysis, Basic Sciences of Medicine , Vol. 11 No. 1, 2022, pp. 5-15. doi: 10.5923/j.medicine.20221101.02.
1. Introduction
- Clinical subjects are those subjects which are perpetually and essentially used in the diagnosis of disease and management of treatment during clinical practice as the chief objective of clinical practice is to keep human body free of discomforts and diseases. But the diagnosis of disease and management of treatment during clinical practice not only completely involve knowledge of Anatomy but also comprehension of medical subjects and human body, the abode of disease, are indispensably necessitate Anatomy as the clinical practice is evolved from developing techniques / methodologies to eradicate discomforts and diseases by understanding disease then formulating its detection and deletion from human body with the help of developing medical subjects in medical education. So, comprehension, investigation and diagnosis of disease are essential and it is the first step of clinical practice to meet the its objective, the end use of medical education. Let us elaborate it. The disease is generated by causatives (invasion of antigens, injury or trauma, misuse of limbs, iatrogenic injuries, sudden exposure to varying environmental conditions and developmental symptomatic variations) creating anatomical disturbances in human body. These disturbances create distortions in shapes, sizes, locations, orientations, branching patterns, pathways and configuration of macro/microstructures forming organs, systems and limbs through setting / organization / configuration of these structures. The structures, invaded by above causatives, may be infected / distorted / degenerated / broken or produce distortions (break, cut, degeneration, extra growth, stones, narrowing, dilatation, thickening, thinning, blockage, dislocation, compression, variation, hematoma formation and variant attachments of tendon / ligaments and muscle fibers). These distortions alter the constituents of fluids and fluid dynamics in the vessels, deregulate the secretion/ excretion of chemicals from organs and glands including metabolic other processes. These distortions along with their cascading effects impair the normal functions and activities of anatomical structures, organs and systems (SOS) creating signs and symptoms of discomforts of disease. Therefore, the disease can be diagnosed only with thorough knowledge of normal/distorted anatomy, as explained above. The mapping the distortions, in morphology and morphometry of effected SOS followed by cascading disturbances in normally regulated processes in relation to functions and activities of anatomical SOS, is correlated with its impact on impairment of the activities and functions of SOS and these processes together produce signs and symptoms of discomforts of disease. To manage the disease, it has to be diagnosed. The diagnosis of disease is carried out by physical examination based on the patient’s input (chronology of disease, its genetic relation with the family history, causative to estimate pathogen and signs and symptoms of disease). Thereafter, the confirmation of preliminary diagnosis by physical examination is done by imagery interpretation and lab. tests. This clearly establishes that, for diagnosis of disease, the comprehension of Anatomy is essential for estimating, genetic relation, distortions and physical examination in relation to SOS. To evaluate malfunctioning of SOS thereby signs and symptoms, Physiology is required to be understood. But Physiology is the science of functions of Anatomical SOS so, it can only be learned with the help of Anatomy. Pathology (disease) is to be understood to correlate it with distortions in anatomical SOS and impairment of functions. This clearly says that the understanding of Pathology completely depends on Anatomy. Similarly, learning of all other subjects also need knowledge of Anatomy as all these subjects deal with management of the disease in human body (HA). So, all the medical subjects must be clearly understood to apply this knowledge in diagnosis and analysis of treatment. Diagnosis consists of Physical examination of human body (HA), radiological interpretation (Radiology), laboratory tests by Pathology [1], and Microbiology. Treatment analysis for location, organ and system (HA) specific molecules, for mechanism of action of drug/medicine/molecule (Pharmacology), for restoring distortions, discomforts and impairment of SOS without side-effects of Medicine and mapping and delineation of access path and target structure for planning Surgery [1]. All these things are related to either human body thereby HA or disease (Pathology and Physiology) and its eradication. As explained above, primary diagnosis is carried out first by physical examination on the basis of signs and symptoms and impairment of functions of SOS. This requires not only sound knowledge of surface HA with respect to relevant landmarks but also the detailed knowledge of concealed internal SOS their morphology, morphometry and configuration of SOS on the basis of surface anatomy. In addition to this, interwoven interrelationship of SOS with functions and activities, signs and symptoms and diseases should also be known to correlate these parameters and to advise right imagery and lab. tests in final diagnosis. Beyond this, imagery interpretation does need in depth knowledge of HA for comparing normal and distorted structures.The medicinal treatment analysis requires above-mentioned skill in HA to be highly essential not only for radiological interpretation but also for confirming diagnosis by crosschecking radiological interpretation report leading to accurate disease. However, in the routine practice, the clinicians believe the accuracy of report without crosschecking and analyze the treatment. After diagnosis, the treatment is analyzed on the basis of new molecules discovered in relation to location, organ or system specific medicine drugs to avoid side-effect and reaction of medicines. As regards surgical treatment, it requires safe access path, identification of target structure target structure and configuration of surrounding structures to avoid iatrogenic injury. Therefore, due to perpetual need of HA at all stages of medical education including clinical training/practice, a study has been designed to assess the need and applicability of HA in medical education and clinical practice from literature review and our own critical analysis to declared HA, a clinical subject so that the delivery of necessary and sufficient HA could be insured at preclinical phase coupled with required HA could also be supplemented continuously at all stages of medical education by horizontal and vertical integration of HA, be it, Medical Graduation, Post-Graduation (specialty) and Post PG (super-specialty) levels. Therefore, the objective of this study is to analyze as to why HA should not be a clinical subject as it is part and partial of not only clinical practice but also medical education.
2. Material and Methods
- HA constitutes the basic foundation of medical education, providing the fundamental concepts of the development of morphology (shapes, sizes, locations, orientations, pathways, branching and configurations, parameters of SOS) and morphometry of SOS. The microanatomy of microstructures and touching reference of genetics also lies in the syllabus of HA. HA is acquired/delivered at two stages, 1. HA at preclinical stage and 2. Applied/Clinical HA during clinical training/practice stages. As HA is needed continuously and constantly at all stages of medical education, so, the literature survey has been carried out to assess the degree of demand, necessity, importance, usefulness and applicability of HA in clinical practice on 3 bases; the need of HA independently to learn human body, to comprehend other medical subjects and then its application in clinical practice which is end use of medical education. This reveals that HA is delivered/acquired in preclinical phase to master it so that it can be applied in learning other medical subjects which are used in diagnosis and treatment during clinical training and practice.The literature has been reviewed to explore the interwoven interrelation of HA with other medical subjects namely Physiology, Pathology, Radiology, Microbiology, Community medicine, Forensic, Pharmacology, Medicine, Anesthesia, Surgery and the application of HA in diagnosis and treatment of diseases during clinical practice. In addition to this, the usefulness of variations/anomalies in SOS is very important not only to understand human body, to grasp other medical subjects and their implication on clinical practice. The degree of need of HA to comprehend other medical subjects will be estimated. Thereafter, the need of HA will also be assessed for carrying out safe and successful clinical practice.
3. Results
- The need of HA to understand human Body: The cultivation of basic theoretical knowledge of HA in association with cadaveric dissection delivers the knowledge of growing shapes, sizes, locations, orientations, branching patterns, pathways and configuration/organization of structures (morphology) of embryo to complete human body including variant DNA configuration carrying characters for genetic diseases etc. The configuration/organization of structures constitute organs, systems and limbs. This study will enable to learn normal/variant morphology of the structures, organs and systems. Thus, besides Gross Anatomy and morphology at microstructure level, the most important and crucial factor to understand human body is the multitude of variations/ anomalies in Gross and Microanatomy which are sometimes symptomatic and many times asymptomatic occasionally generating disease in structures (Vessels, Nerves, Bones, Muscles, tendon, ligaments etc.), Organs/Glands (Brain, Heart, lungs, livers, Abdomen, intestines, Kidney, Pancreas etc.) and systems (Digestive system, Circulatory system, Skeletal system, Muscular system, Respiratory system, Endocrinal system, Nervous system, reproductive system, integumentary system, excretory system, lymphatic system, immune system, urinary system), either due to these variations or distortions by infection or trauma and creating hurdles in diagnosis and treatment. The sound knowledge of HA will make the medical trainees’ skillful and expert to have command on HA. The need of HA to understand other medical subjects: Now, let us elaborate how HA supports learning of other medical subjects efficiently (Fig. 1).
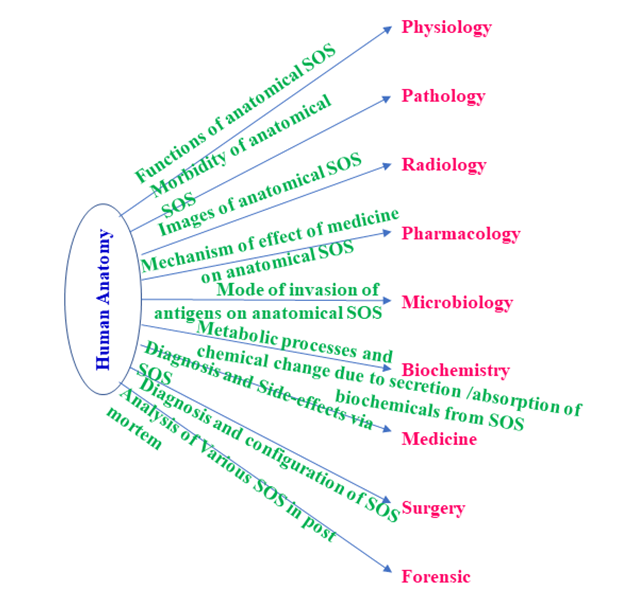 | Figure 1. Dependence of other subjects on Human Anatomy to comprehend medical education |
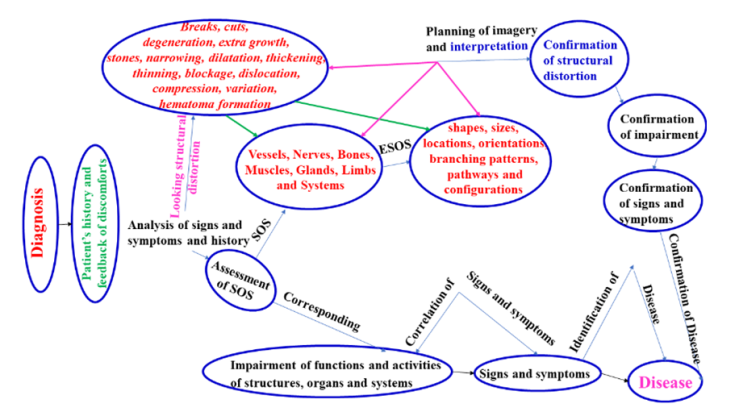 | Figure 2. Application of Human Anatomy in diagnosis |
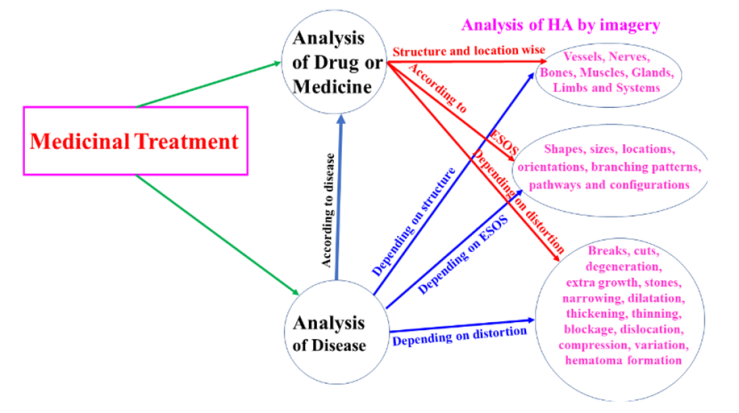 | Figure 3. Application of Human Anatomy in medicinal treatment |
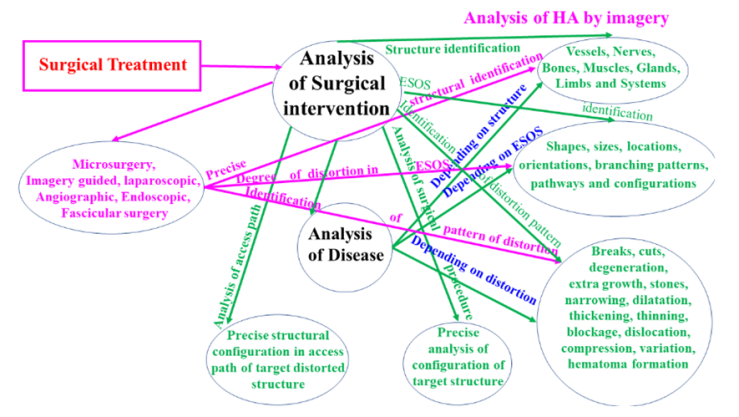 | Figure 4. Application of Human Anatomy in surgical treatment |
4. Discussion
- The discussion will be focused on the objective of article for considering HA as a clinical subject. So, if the use of HA is essential throughout medical education in general and most essential in clinical training/practice in particular, it must be recognized as a clinical subject. However, in the present system of medical education, the teaching of HA is either only during preclinical phase or it is integrated horizontally and vertically during entire medical education. After preclinical clinical stage, there is no standard pattern or syllabus of teaching HA during clinical training of UGs, PGs and P PGs. Conventionally, during teaching or guidance in clinical training, the students are guided extemporarily, case wise, by clinicians. HA is a rote subject and is forgotten rapidly so whatever remnant HA they know on the basis of that they guide the medical student either, or the students learn HA by themselves. But in the present scenario, the medical students were found to possess inadequate knowledge of HA by both these systems as expressed by clinicians and anatomists both [11,12]. So, if HA is recognized as a clinical subject and its schedule and syllabus is revised as per need and application of HA, it will improve the learning clinical training / practice as comprehension of anatomical structures, their configuration in to organs and systems of human body and all the medical subject so efficiently that there will be tremendous improvement in the quality of clinical practice as it is explicitly, elaborated in preceding sections. Therefore, the HA should be not only taught during the preclinical phase to create foundation of basic HA to grasp other medical subjects but also it should be cultivated during clinical training of UGs, PGs and P PGs in medical education through integrating HA with teaching and formulating proper syllabus of HA at all these stages as per need and application.HA to understand a normal human body: The end use of medical education is clinical practice. The clinical practice hovers around management of diseases in human body. But the disease is caused by to trauma/injury, infection and/or developmental variations/anomalies in the morphology of anatomical SOS of human body. These causatives generate distortion in morphology of SOS. Thus, root cause of disease is these distortions. These distortions not only create impairment of functions/activities of SOS but also it alters the kinematics of fluid, fluid content, excretion/secretion from glands, metabolic and other processes and activating the immune system to fight against the threat by brain. So, to understand normal/variant morphology consisting of shapes, sizes, locations, orientations, branching patterns, pathways and configuration of macro/microstructures forming organs, systems and limbs, to estimate dysfunction/impairment of SOS and corresponding signs and symptoms to comprehend diseases. But, HA of human body is very vast, rote and complex subject having enormous normal/variant macro / microstructures, configured in large numbers of organs and systems at gross and microanatomical levels. The identification of distorted structure with respect to landmarks on human body, their development from embryo to fully developed human body together with the SOS undergoing progressive changes during growth producing developmental anomalies/variations, many times, causing symptoms and many times asymptomatic and the configurations of structures in organs and systems are most essential to learn other medical subjects and clinical practice. Apart from this, the knowledge of shapes, sizes, locations, orientations, branching patterns, pathways and configuration of microstructures is also crucial in general but in nerves in particular. These variations are learned through histological slides. The changes are also taking place in RNA and DNA, from parents to the child, associated with many genetic diseases and other characters carried by these genetic structures. No two human bodies are alike in morphology so there are very huge numbers of variations from one body to another. These variations are not only present in morphology of structures alone, rather these variations are also present in configured organs and systems having bearing on the working and functioning of SOS. The accurate mapping of internal SOS from surface of the body also becomes doubtful during physical examination due to variations. These variations and/or distortions also produce alterations in irrigation pattern of blood supply, communication pattern of neural network, secretion and excretion pattern of organs and glands and functions of SOS and processes. These alterations in functions and metabolic and other processes produce changes in fluid contents/fluid dynamics crating many other problems. Due to these variations, the functions and working of SOS also changes along with creating many complications in human body. Thus, to understand human body in full, these anatomical SOS are to be mastered fully-well pertaining to morphology, morphometry and setting of the macro/microstructures in relation to functions/working and activities of SOS along with the impact of these variations on functions/activities there by discomforts in SOS of human Body. The need of HA to understand other medical subjects: Having studied HA, as explained in result section, the study of all the medical subjects directly or indirectly, depends on variant/normal morphology/morphometry, organization /setting or articulation of structures. As the SOS and their configuration completely, control the functions/ working and activities of SOS, limbs of human body. So, if there is any change in morphology of SOS in form of distortion / injury due to causatives of diseases like symptomatic developmental variation and anomalies of SOS as well as infections/trauma/injury, the functions/working and activities of SOS is altered/impaired producing signs and symptoms of discomforts of disease. So, comprehension of Physiology, Pathology solely depends on HA. As in patients, the disease detection is the chief tool of final diagnosis through imagery interpretation and lab. tests done by Biochemistry, Pathology and Microbiology can be comprehended only if the students/clinician possess sound knowledge of normal/variant morphology/morphometry of SOS in Gross and Microanatomy. The learning of medicine and surgery consisting of diagnosis and treatment which, as explained above completely, depend on knowledge of specialized application of HA to clinical practice. Before surgery, the decision on general/local anesthesia is to be taken by anesthetist in consultation with surgeon. Then, which nerve? at what location? is to be blocked for painless successful surgical intervention, depends on precise and meticulous knowledge of Neuroanatomy. After failure cases or accidents, the medicolegal aid is sought. The medicolegal aid as well as settlement of claim by insurance company demand anatomical explanations. So, HA is crucial in studying Forensic sciences. In the article of Singh et al. 2021 [13] the authors chalked out a scheme to train the upcoming anatomical faculties in such a way that they will ideally suit to deliver the needful Anatomy at different stages of medical education. Thus, the teaching/learning of HA is needed over the entire span of medical education and clinical practice. The need of HA to carryout safe and successful clinical practice: First of all, to understand diagnosis and treatment during clinical practice, the trainee/clinician needs the language of medical education/ practice to interact with patients/attendants, fellow colleagues, consultant/guides. The teaching of preclinical HA provides the foundation of medical education/clinical practice by cultivating the language of medical education/practice needed to interact with patients and colleagues [1,14].Diagnosis: The diagnosis depends on detection of morbid morphology of human body due to symptomatic developmental variation/anomalies or by trauma/injury or infection by pathogens. This morbidity is expressed by anatomical distortions which create impairment of functions and activities of SOS together with cascading effect of this distortion, it also deregulates the metabolic or other processes. These disturbances produce signs and symptoms of discomforts of disease. So, diagnosis starts with physical examination based on patient’s input locating probable distortion/injury on the surface of body observation, palpation, percussion and auscultation [7] Assessing the distortion in SOS, location and degree of injury/distortion in specific SOS its impact on function and activity of that SOS, the signs and symptoms of discomforts and disease, are correlated with one-another (Fig. 1). The location of SOS, distorted macro/microstructure are to be estimated from the surface of the body with respect to surface landmarks. This is only possible when internal arrangement or configuration of SOS in relation to surface Anatomy is known. This clearly, needs the sound knowledge of Surface and Gross Anatomy including Microanatomy through cadaveric dissection. Thus, it is a well-established fact that without HA even, preliminary diagnosis is impossible to be done. These facts together, lead to the analysis of imagery and lab. tests. Thereafter, the cascading effect of this distortion on metabolic and other processes is also analyzed. Inference of this analyses together, suitably, advise the imagery and lab. tests. This, certainly, involve complex anatomical relation of the SOS and processes. Thus, sound and analytic knowledge of HA to apply in primary diagnosis, is highly crucial. Thereafter, the imagery interpretation and lab. tests also need to be analyzed on the basis of one-to-one and interrelation with image and object and processes running in human body as explained in result sections. Story does not end here rather, when the clinician critically analyses the disease, he should also crosscheck these reports so, he too needs to know relation between the anatomical SOS and images and corresponding functional changes in processes. However, general perception is that clinician believes these reports and assesses the diagnosis. As all these things are directly and intimately related to HA and essential part of diagnosis of disease, so, knowledge of HA is very crucial in this process of diagnosis. To further elaborate use of HA, Description of following typical cases of diagnosis may be helpful to understand the need of HA.Anatomical basis of clinical examinations of the abdomen: Knowledge of Anatomy is required for clinical examination for making preliminary diagnosis. For example, if there is pain in right hypochondrium. Pain in right hypochondrium may be, due to, involvement of liver or gallbladder. If the medical trainees do not know the accurate location of liver, gall bladder, their shape, size and configuration of liver and gall bladder in relation to right hypochondrium and surface anatomical landmarks, they can’t proceed for examining these organs for anatomical distortions corresponding to pain. In case of thorough knowledge of surface Anatomy to the student/ clinician, they can proceed for palpating the right hypochondrium for investigating the hyper/hypotrophy of liver of and gallbladder. Thus, detailed morphometry and morphology of liver and gallbladder is prerequisite for preliminary investigation of these organs for pain in relation to diseases. Similarly, if the pain radiates to inferior angle of scapula (indicating pathology in gallbladder), the clinicians may misinterpret it for pathology of back or related to scapular bone. After making preliminary diagnosis imagery is advised for final diagnosis and deciding the line of treatment. This is a simple example which exhibits how HA is required for diagnosis and treatment. Comprehension of functional Anatomy in relation to Pathophysiology (Equilibrium Problem): Body equilibrium is maintained by maculae located in internal ear. Macula is sensory epithelium containing large number of hair cell responding to orientation of head with respect to gravity. If there is any alteration in the normal anatomical structure of sensory epithelium/hair cells, it leads to vertigo. If the trainee is unaware of normal anatomical structure of macula and its relations with other structures, the function of macula cannot be comprehended and also it will be difficult to diagnose the cause of vertigo. Thus Physiology (function), one of the subjects of medical education cannot be understood till HA is well understood. This is an example illustrating how anatomy is useful for comprehending Physiology and Pathology to carry out diagnosis and treatment. Similarly, comprehension of other medical subjects and management of diseases solely depends on HA.Treatment: Having diagnosed the disease, if the treatment by medicines has been decided. Then, it is analyzed and prescribed as explained in result section. As the medicinal molecules have been discovered as disease specific, location, organ and system specific so the correlation of disease with respect to anatomical parameters is essential indicating the need of anatomical knowledge. Such as, for antibiotic therapy, antibiotic medicine, for abdomen complication, is to be critically analyzed as what other useful bacterial are threatened. Similarly, throat specific antibiotic medicine may not be suitable for respiratory disease. So is the case with other antibiotics for use. If surgical intervention is the solution to manage the patients’ disease, the surgeon needs safe access via surgical path and accurate identification and repair/removal/grafting of morbid structure with the help of knowledge of morphology, morphometry from landmarks and configuration of surrounding structures for carrying out the safe procedure. Presently it is done through radiological images but in presence of new variations and configurations, there always remains a chance for unusual invasion. If this is done in association with an anatomist, it may improve the procedure. In this procedure, starting from the placing of incision and opening of the distorted structure through access path, the surgeon must be conversant with all the structures in access path and surrounding structure to avoid iatrogenic injury. Similarly, imagery guided surgery and laparoscopic procedures requires more meticulous and precise HA with mapping of all the structures for safe and successful procedures. This further demands detailed knowledge of HA. As regards microsurgery pertaining to neural complications, both at nerve-level and fascicular level there are many frontier areas completely dependent on HA such as, 1. Identification of injured nerve, 2. location and degree of injury and in case of neural disorders due to fascicular injury also needs 3. Identification of injured fascicle, location and degree of injury. It is pertinent to mention here that the imaging of injured fascicle is almost impossible by any imagery tool due to resolution limitation and image defects. However, renowned radiologists, namely, Bäumer et al., [2] and Chhabra et al., [3] claim that not only, fascicle but also, injury on fascicles can be imaged and interpreted through high resolution MRI. Although the fascicular dimensions are beyond the resolution limit, still they plead that with special technique of frequency color coding, the location of injury and fascicle can be interpreted with some element of subjectivity. The neurosurgical procedures need not only the location, identification and configuration of nerve through its morphology and morphometry with respect to landmarks in relation to other anatomical structures but also the shapes, sizes, locations, orientations, branching patterns, pathways and configuration of fascicles and their innervation pattern as required “to develop rational bases for repair and development of engineered constructs” [10]. As, in many cases, it is possible to replace specific injured fascicle for fascicular injuries in place of grafting the nerve so, very precise complete Fascicular Anatomy is required for such procedures. Full functional recovery is a day dream. [10] In such cases, however, maximum 50% recovery has been observed [15]. As per authors view, the low recovery is due to cross-sectional mismatch of two ends of fascicles being grafted. But there will be tremendous improvement in functional recovery through fascicular grafting procedures if the shape and size of fascicular ends’ cross-sections are matched. This can be achieved by the fascicular correlation and calibration if done in identified nerve with respect to established landmarks through histological studies [4,5,6]. Not only the injured fascicle can be identified but also their cross-sections can be matched by counting number of axons at the grafting ends through histological slides for better functional recovery as functional recovery is poor in fascicular grafting [10]. For more advanced techniques of Surgery like imagery-based surgery, laparoscopic surgery, angiography etc. need more anatomical backup to improve these procedures.In continuation, if the entire surgical procedure is carried out on a cadaver with an anatomist, it may produce very encouraging results and boost the confidence of the surgeon. Hubbell et al., [16] have written: “Feeling the need for more anatomy in surgical procedures, the University of South Florida developed a system of instruction in which regional anatomy is taught both before and during surgical procedures in the operating room.” An affiliation between surgery and anatomy has been combined with a reorganization of anatomy education, characterized by (1) long-term vertical integration (from first year of medical studies to final postgraduate clinical specialty examination), and (2) a core of anatomical knowledge defined by the needs of primary care physicians (first to third year) [17]. This compulsory common core is complemented by optional specialized teaching directed by students' individual interests and future career choices (fourth to sixth year). Various studies carried out seeking opinion of students, faculties and clinicians supported that more knowledge of HA is required at all stages of medical education [12]. This establishes the concept that HA should be regarded as a clinical subject. In the event of failure case, not only the defense by medicolegal process, completely, depends on precise anatomical input, be it, medicinal or surgical treatment, but also, the Forensic science analysis require the anatomical knowledge to supplement the concepts.Analysis as to ‘why HA should not be a clinical subjects’: The clinical subjects are perpetually and essentially used during learning of medical education in general and clinical practice in particular. Though the knowledge of all the medical subjects is applied in clinical practice, yet those subjects, which are actively and necessarily used in diagnosis and treatment are kept in the list of clinical subjects. The Clinical practice emanates from taking care of human health, chiefly related to morphology and its morbidity pertaining to HA so, diagnosis, treatment and recovery process directly and essentially, depends on HA right from patient’s feedback, physical examination, image analysis, lab. tests (Diagnosis) and analysis of treatment, be it by medicine or surgery as elaborated above. The more need of Anatomy has been felt both by student trainees and consultant clinicians [11,12]. It is pertinent to mention here that applied Anatomy (frequently termed Clinical Anatomy) is the most challenging part since it can neither be applied nor taught without thorough knowledge of basic anatomy together with ideally delivered by updated anatomical faculties developed as described by Kumar and Singh, 2019 including Singh et al., 2021 in their articles [13,18]. In the absence of above conditions there will be a lowering of the standard of medical education/practice as pointed out by Cornwall et al., [19] and Leveritt et al., [20]. Thus, as elaborated above, HA is not only highly useful in understanding the other related medical subjects but also it is applied at all stages of learning clinical practice. The knowledge of HA is also pivotal to complete medical examination through diagnosis and treatment and also to properly communicate with patients and colleagues [14]. Within clinical departments, the need for professionals in human gross anatomy is uncontested because the Anatomy remains a key discipline for safe and successful clinical practice [21]. Clinical practice, as illustrated above, cannot be carried out without an understanding of Human Anatomy as it is an integral part of clinical practice. That is why vertical integration of HA is vigorously followed in developed countries [22]. One phenomenon, that has to be avoided, is an increase in malpractice lawsuits pointing at anatomic shortcomings. In this instance, particularly surgeons and interventional radiologists will be at risk for having failed to meet standards of care pertaining to increase in malpractice lawsuits [23]. As the diagnosis and treatment of diseases depend on anatomical causatives spread over the entire body and integration of anatomy is recommended by renowned clinical and anatomical stalwarts so expertise of Human Anatomy needs to be added at all the stages of medical education in all clinical fields. Applied HA frequently, used as clinical HA in clinical practice so, it is a clinical subject. The model provided by Fasel [17] sketches out what a reorganized anatomical education can look like. Its characteristics of long-term vertical integration (from first year of medical studies to final postgraduate clinical specialty examination), and a core of anatomical knowledge defined by the needs of primary care physicians are worthy of further consideration. When augmented by optional specialized teaching directed by students' individual interests and future career choices later in the curriculum, it offers a way forward for our proposals. We therefore suggest that medical schools become aware of the fact that anatomy's affiliation to basic science departments is historically conditioned and needs to evolve, possibly by joining a clinical department [21] However, not only, the complete scheme of organization of syllabus, time schedule, teaching/integration of HA and continuous development of medically qualified competent faculties have been brought out [18,13] to facilitate the adoption of HA as a clinical subject.
5. Conclusions
- The ongoing need of Anatomy in clinical training during medical education and/or clinical practice has been examined. This demonstrated that students and clinicians feel anatomical knowledge as most essential at every stage of their training during medical education. This is supported by the current trend of horizontal/vertical integration of Anatomy throughout medical education. Clinicians, while practicing also need the knowledge of Anatomy to diagnose diseases and analyse the treatment. Better management of medicolegal cases may be accomplished by a synergistic approach by clinicians, radiologists and anatomists. Therefore, Human Anatomy has, almost, been established that it is a clinical subject.