-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2020; 9(1): 8-9
doi:10.5923/j.medicine.20200901.02

Morphometry and Morphology of Foramen Petrosum in Indian Population
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh1, Nand Kishore Gupta1, Raj Kumar2
1Department of Anatomy, Uttar Pradesh University of Medical Sciences Saifai 206130 Etawah UP India
2Department of Neurosugery Uttar Pradesh University of Medical Sciences Saifai 206130 Etawah UP India
Correspondence to: Rajani Singh, Department of Anatomy, Uttar Pradesh University of Medical Sciences Saifai 206130 Etawah UP India.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Greater wing of sphenoid contains three constant foramina, Foramen ovale, foramen rotundum and foramen spinosum. The presence of foramen Vesalius and foramen petrosum are inconsistent. Normally foramen ovale transmits mandibular nerve, accessory meningeal artery, lesser petrosal nerve and emissary vein. When foramen petrosum is present, lesser petrosal nerve passes through petrosal foramen instead of foramen ovale. Lesser petrosal nerve distribute postganglionic fibers from otic ganglion to parotid gland. In absence of knowledge of petrosal foramen transmitting lesser petrosal nerve, the clinician may damage the nerve during skull base surgery creating complications like hyperemia of face and profuse salivation from the parotid gland (following atropine administration), lacrimation (crocodile tears syndrome) and mucus nasal secretion. Considering clinical implications associated with petrosal foramen, the study was carried out. The aim of the study is to determine the prevalence of petrosal foramen in Indian Population and to bring out associated clinical significance. The study was conducted in the department of Anatomy UPUMS Saifai Etawah Indian. 30 half skulls were observed for the presence of petrosal foramina and morphometry was also done. Literature search was carried out, our findings were compared with previous work and associated clinical implications were bought out.
Keywords: Petrosal foramen, Lesser petrosal nerve, Foramen ovale
Cite this paper: Rajani Singh, Nand Kishore Gupta, Raj Kumar, Morphometry and Morphology of Foramen Petrosum in Indian Population, Basic Sciences of Medicine , Vol. 9 No. 1, 2020, pp. 8-9. doi: 10.5923/j.medicine.20200901.02.
1. Introduction
- Greater wing of sphenoid (GWS) forms part of middle cranial fossa. Multitude of regular and irregular foramina are found in GWS. Consistant foramina in this area are foramen rotundum, foramen ovale and foramen spinosum. Inconsistent foramen are foramen Vesalius also known as Sphenoidal emissary foramen, Canaliculus innominatus also known as Arnold’s foramen or petrosal foramen or foramen petrosum. Petrosal foramen is located between foramen ovale and spinosum [1]. Lesser petrosal nerve normally passes through foramen ovale along with mandibular nerve, accessory meningeal artery and emissary vein [2] in absence of petrosal foramen but if petrosal foramen is present, it forms conduit for lesser petrosal nerve. Foramen ovale and spinosum are well documented in literature but petrosal foramen has received less attention in literature especially in Indian scenario. Presence of petrosal foramen may affect the course of lesser petrosal nerve and may be damaged during skull base surgery creating multiple discomforts to the patients. So knowledge of presence of this foramen carries immense value. Therefor the study was carried out. The aim of the study is to bring out prevalence in Indian population and clinical significance of this foramen.
2. Material and Methods
- The study was conducted in the department of anatomy UPUMS saifai Etawah UP India. For this study 30 half skulls (60 sides) were observed for the presence of this foramen. The morphometry of these foramina was also done. Age and sex of the skulls were not known but all the skulls were of adults. Literature search was conducted and our findings were compared with the previous investigators and associated clinical significance was brought out.
3. Results
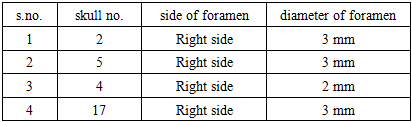
- Out of total 30 half skulls (60 sides) observed, petrosal foramen was detected in 4 skulls constituting 13.3%. All these foramina observed were located on right side between foramen ovale and spinosum (Fig.1).
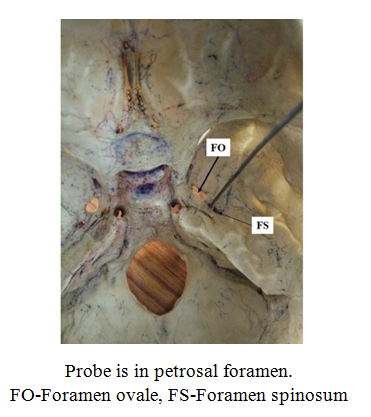 | Figure 1. Showing petrosal foramen on right side |
|
4. Discussion
- There is paucity of literature describing petrosal foramen. Various shapes such as slit like opening, ovale shaped or rounded shapes were detected. Slit like/ rounded opening of Arnold’s foramen between spheno-petrosal fissure was observed by Sondheimer in 20% of 50 base view skulls [1]. Incidence of this foramen in our study (13.3%) was lower than that of above study. This structure, when medial to line drawn along the long axis of foramen ovale through foramen spinosum was found in 20 patients constituting 16.3% [1]. We did not find such location of foramen of Arnold in any of the observed skulls.This foramen was observed in 20 patients out of 123 patients constituting 16.3% [3] in CT scans done for temporal bone disorders. The incidence of petrosal foramen of our study was lower than this work also. These scientists observed this foramen bilaterally in one case. We did not observed this foramen bilaterally in any of the skulls. All petrosal foramina in our study were on right side.Lesser petrosal nerve was observed to pass through canaliculus innominatus in 70% cases [2] indicating presence of this foramen in 70% cases. In literature we did not find any description of morphometry of foramen petrosal so it cannot be compared here.Petrosal foramen when present transmits lesser petrosal nerve originating from tympanic plexus also contain the fibers of facial nerve. In absence of canaliculus innominatus the lesser petrosal nerve passes through foramen ovale [4]. This nerve contains pre-ganglionic parasympathetic fibers which synape in otic ganglion. Post ganglionic fibers then passes in auriculotemporal nerve innervating parotid gland. Damage to the greater petrosal nerve and the lesser petrosal nerve produces face hyperemia and profuse salivation from the parotid gland (following atropine administration), lacrimation (crocodile tears syndrome) and mucus nasal secretion [5]. Proper comprehension of lesser petrosal nerve and its passage may reduce the complications arising due to its damage in surgical approaches to the middle cranial fossa [5]. Lesser petrosal nerve is to be sectioned for treating migrainous neuralgia in cases where medicinal treatment does not provide relief or where trigeminal rhizotomy is ineffective [6]. The importance of defining this structure (petrosal foramen) is to avoid overlooking lesions (tumor or vascular) developing in its vicinity [7].
5. Conclusions
- Foramen petrosum is an important landmark in skull base injury especially in the middle cranial fossa and infratemporal fossa related surgeries. Lesser petrosal nerve may be damaged if its point of exit is not known to neurosuegeons during skull base surgery. In absence of knowledge of petrosal foramen, confusion may be created as it may be considered to be passing through foramen ovale during skull base surgeries.