-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2019; 8(1): 18-21
doi:10.5923/j.medicine.20190801.03

Morphometry of Ulnar Collateral Ligament and Its Role in Kinematics of Elbow
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh, Karishma Sharma, Mukesh Singla
Department of Anatomy, AIIMS Rishikesh, Veerbhadra Marg Rishikesh, India
Correspondence to: Rajani Singh, Department of Anatomy, AIIMS Rishikesh, Veerbhadra Marg Rishikesh, India.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

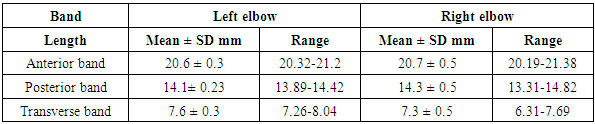
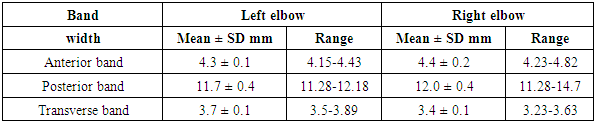
Ulnar collateral ligament comprised of anterior, posterior and transverse bands. The ulnar collateral ligament maintains valgus stability of the elbow. It may lead to valgus instability, pain, reduced accuracy and decreased velocity in overhead throwing sports. In many patients medical treatment fails to relieve the symptoms due to injury to ulnar collateral ligament so in these patients surgical repair or reconstruction of this ligament is done to restore elbow function and stability. Thus anatomy and biomechanics of this ligament is essential to carry out surgical intervention. Hence the study has been carried out in elbows of North Indian Population. Aim of the study to perform the morphometry of various components of ulnar collateral ligament of elbow joint of cadavers of North Indian origin. The study was conducted in the Department of Anatomy. 12 upper limbs from 6 cadavers of mean age of 74.8 years of North Indian origin fixed in 10% formalin were dissected. The ulnar collateral ligaments of the elbows were exposed and morphometry was done using digital Vernier callipers. Mean lengths of of anterior, posterior and transverse bands were 20.6, 14.2 and 7.4 mm respectively. Mean width of anterior band, posterior band and transverse band was 4.3, 11.9 and 3.6 mm respectively. This morphometric data will be of immense use in repairing and reconstructing ulnar collateral ligament in patients of North Indian population.
Keywords: Ulnar Collateral Ligament, Surgery, Medial Collateral Ligament, Elbow Joint, Elbow
Cite this paper: Rajani Singh, Karishma Sharma, Mukesh Singla, Morphometry of Ulnar Collateral Ligament and Its Role in Kinematics of Elbow, Basic Sciences of Medicine , Vol. 8 No. 1, 2019, pp. 18-21. doi: 10.5923/j.medicine.20190801.03.
Article Outline
1. Introduction
- Elbow joint is reinforced by various ligaments. One of them is ulnar collateral ligament. It is triangular in shape and consists of anterior band, posterior band and transverse band. The anterior band is strongest and stiffest, attached by its apex to the front of medial epicondyle and by distal base to the sublime tubercle on the medial coronoid margin. Posterior band extends from back of medial epicondyle to the medial margin of olecranon process. Between these two bands, intermediate fibers descend from medial epicondyle to transverse band [1].Anterior band remains tight throughout the flexion but posterior band becomes taut between half and full flexion [1]. Function of transverse band is not clearly defined.Ulnar collateral ligament of the elbow maintains valgus stability of the elbow and is the principal elbow stabilizer [2,3]. Ulnar collateral ligament is crucial for throwing sports like baseball and javelin including racquet and ice hockey. Repetitive overhead throwing activities in young athletes may cause injuries to elbow and its ligaments leading to constant pain and instability. In athletes elbow dislocation may also lead to ligamentous injury resulting into chronic pain and valgus instability. Thus the knowledge of ligamentous anatomy and biomechanics of elbow in throwing sports is of utmost use for proper management of potentially disabling ligamentous injury to elbow [4]. To the best of knowledge of authors, no data describing the morphometry of ulnar collateral ligament in North Indian Population is available in literature. Hence the study has been carried out. Objective of the study is to provide morphometric data of ulnar collateral ligament to repair and reconstruct this ligament in patients of north Indian origin.
2. Methods
- The study was conducted in the Department of Anatomy AIIMS Rishikesh. 12 upper limbs (6 left and 6 right) from six cadavers of mean age of 74.8 years of North Indian origin fixed in 10% formalin were dissected in the laboratory. After clearing all the tissues around the elbow, the ulnar collateral ligament was exposed and photographs were taken. Measurements of lengths of ligaments from the centre of origin to the centre of sublime tubercle and maximum width of these ligaments were observed with Vernier callipers. Width was taken without considering the length of tendon. Measurements were taken by two persons separately. Single measurement for each ligament was performed.Donated cadavers were used for this study so no ethical clearance is required.
3. Results
- Ulnar collateral ligament was found to consist of anterior, posterior and transverse bands (Figure 1).
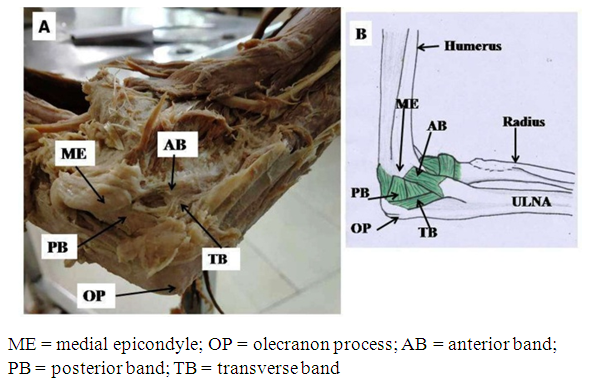 | Figure 1. (A) showing ulnar collateral ligament and its three components. (B) showing schematic diagram of ulnar collateral ligament and its components |
|
|
4. Discussion
- Stability of the elbow joint depends on passive and active stabilization. Capsule of joint and bony structure particularly radial head are primary stabilizers of elbow. However ligaments especially the ulnar collateral ligament provide passive stabilisation to this joint. Of various ligaments of elbow, it is ulnar collateral ligament particulary its anterior band , resists valgus stress during flexion of elbow [5,6]. Few authors are of view that anterior band is the principal ligament stabilising the elbow in valgus stress along with radial head and dynamic stabilizers of the elbow [7,8]. Fifty percent of the elbow joint stability is maintained by ulnar collateral ligament at 20-70 degrees of flexion [5,6] but it (ulnar collateral ligament) bestows only 33% joint stability in full extension. Rest 67% of joint stability is provided equally by capsule and bone [9,10]. When elbow is flexed at 90º, 55% of the resistance to valgus stress at the elbow is contributed by ulnar collateral ligament. According to Alcid et al, valgus stability is perpetuated by ulnar collateral ligament, bony structures and capsule equally. However anterior band is the main structure preventing valgus instability [9].
4.1. Importance of Morphometry of Ulnar Collateral Ligament
- Length: Anterior band is the largest ligament of the medial elbow extending from medial epicondyle up to sublime tubercle and may reach up to ulnar ridge. The mean length of anterior band as reported in literature ranges between 21.1 mm and 31.4 mm [8,9,11,12]. These lengths were measured from the center of the origin to center of sublime tubercle. Mean length of anterior band in our study is 20.6 mm which is slightly lower than reported by above authors. This discrepancy observed in lengths may be due to difference in sample size and also may be due to ethnicity related factors. Recently Farrow et al. reported mean anterior band length to be 53.9 mm and 51.7 mm measured from center of the humeral origin to the most distal point of tapered insertion [13]. The information related to the length of ulnar collateral ligament particularly, that of anterior band band is important for its reconstruction [14].Some scientists are of view that the anterior band is not an isometric soft tissue stabilizer and its length changes throughout flexion. These studies have revealed that length of anterior band changes by 18% ranging from 2.8 mm to 4.8 mm on flexing the elbow from extension [7,8,15]. Thus dynamic length of anterior band is very crucial for biomechanics involving elbow. This fact should be kept in mind during reconstruction of the ligament. The mean width of anterior band increases and becomes maximum when it reaches sublime tubercle and then it tapers to the point of insertion on the ulnar ridge. Reported mean width of anterior band ranges between 4.0-7.6 mm [8,9,11,16]. In the present study the mean width of anterior band, posterior band and transverse band was 4.3 mm, 11.9 mm and 3.6 mm respectively. Mean width of anterior band lies within the reported range. Width of posterior band and transverse band is not reported in literature. The posterior band stabilizes the elbow but it bestows maximum stability during flexion [11]. Morrey and An expressed that transverse band does not play any role in providing stability to elbow [8]. But Camp et al. are of view that since transverse band is inserted directly into anterior band so it plays a crucial role in elbow stability [17]. Ulnar collateral ligament is the principal stabilizer of elbow during valgus stress followed by radial head and flexor-pronator muscles [7]. Ulnar collateral ligament is likely to be injured in overhead throwing athletes during late cocking and early acceleration phases while valgus moment is forced upon elbow [18].Partial or full damage to this ligament causes valgus instability along with pain, reduced accuracy and decreased velocity in overhead throwing sports. Most of these cases require surgical manipulation with ligament reconstruction by placing appropriate graft at both the humeral origin and the ulnar insertion. Thus to restore stability and function of elbow it is essential for the surgeon to comprehend the in depth anatomy of ulnar collateral ligament [14]. First quantitative analysis of the medial ulnar collateral ligament elaborating the dimensions of anterior band and posterior band at various degrees of elbow flexion in ten fresh frozen cadavers was done by Morrey and An in 1985 [8]. Since then several studies elucidating the anatomy and biomechanics of the anterior band has been carried out [7]. Earlier it was thought that anterior band inserts solely and directly onto the sublime tubercle. But recent view is that anterior band insertion is broader, tapered and has larger surface area. Maximum valgus stress develops on elbow during acceleration phase of the overhead throw [19]. During acceleration phase, the valgus stress can surpass the sixty Newton meters limit which is much larger than measured strength of the ulnar collateral ligament in cadavers. Thus valgus stress can surpass the tensile strength of ulnar collateral ligament causing chronic microscopic tears or acute rupture.Bushnell et al. investigated relationship between maximum pitch velocity and elbow injury in twenty three professional baseball pitchers during four seasons. The result established statistically significant association (P = .0354). [20] Four pitchers complained of muscle strain and/or joint inflammation out of nine with elbow injuries. Rest five of nine developed ulnar collateral ligament sprain or tear. Three of the five player entailed surgery for repairing ulnar collateral ligament. These pitchers also had the highest maximum ball velocity [20]. Another study by De Froda et al. supported the findings of Bushnell et al. The authors [21] also found statistically significant association between ball velocity and injury to ulnar collateral ligament. In this study also players with higher ball velocities had ulnar collateral ligament injuries. In addition to this, these authors asserted that frequency of ulnar collateral ligament injury is more common during first three months of the season and ulnar collateral ligament injury is more observed in relief pitchers than in beginners [21]. Bushnell et al. investigated relationship between maximum pitch velocity and elbow injury in twenty three professional baseball pitchers during four seasons. The result established statistically significant association (P = .0354) [20]. Four pitchers complained of muscle strain and/or joint inflammation out of nine with elbow injuries. Rest five of nine developed ulnar collateral ligament sprain or tear. Three of the five player entailed surgery for repairing ulnar collateral ligament. These pitchers also had the highest maximum ball velocity [20]. Another study by De Froda et al. supported the findings of Bushnell et al. The authors [21] also found statistically significant association between ball velocity and injury to ulnar collateral ligament. In this study also players with higher ball velocities had ulnar collateral ligament injuries. In addition to this, these authors asserted that frequency of ulnar collateral ligament injury is more common during first three months of the season and ulnar collateral ligament injury is more observed in relief pitchers than in beginners [21]. The sample size is small so more study with bigger sample size is recommended.
5. Conclusions
- Anterior band of ulnar collateral ligament is very crucial in maintaining the valgus stability of elbow. Data on length and width of ulnar collateral ligament may be of utmost use in graft selection and reconstruction of this ligament in North Indian Population. To comprehend the morphometry and biomechanics is essential clinically to repair the ulnar collateral ligament injuries.