-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2016; 5(1): 5-7
doi:10.5923/j.medicine.20160501.02

Anomalous Configuration of Medial and Lateral Circumflex Femoral Arteries
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh
Department of Anatomy AIIMS Rishikesh, Rishikesh, India
Correspondence to: Rajani Singh, Department of Anatomy AIIMS Rishikesh, Rishikesh, India.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Normally profunda femoris artery arises from femoral artery below the inguinal ligament. Profunda femoris artery gives rise to lateral circumflex artery laterally and medial circumflex artery medially. But abnormal configuration of profunda femoris artery and its branches was observed in two cases in present study during dissection of lower limbs for teaching purpose in the department of Anatomy AIIMS Rishikesh, India. In one case, femoral artery trifurcated into medial circumflex, lateral circumflex and profunda femoris arteries. This finding is rare. In another case, common trunk arose from femoral artery which descended for 2.5 cm and gave medial circumflex artery. This common trunk descended further for 1 cm and bifurcated into lateral circumflex and profunda femoris arteries. This finding is new and unique and hence the case is reported. Knowledge of these variations will be of utmost importance to surgeons carrying out surgical procedures around the femoral triangle, to radiologists to avoid misinterpretation of radiographs and to anatomists for new and rare variants.
Keywords: Femoral artery, Profunda femoris artery, Lateral circumflex femoral artery, Medial circumflex artery, Femoral triangle
Cite this paper: Rajani Singh, Anomalous Configuration of Medial and Lateral Circumflex Femoral Arteries, Basic Sciences of Medicine , Vol. 5 No. 1, 2016, pp. 5-7. doi: 10.5923/j.medicine.20160501.02.
1. Introduction
- Femoral artery (FA) is continuation of external iliac artery. Profunda femoris artery (PFA) originates from posterolateral aspect of femoral artery about 3.5 cm below the inguinal ligament (IL) in femoral triangle [1]. Lateral, Medial circumflex femoral arteries (LCFA, MCFA) and perforating arteries originate from profunda femoris artery. The MCFA and LCFA anastomoses with the internal and external iliac arteries. Perforating arteries supply the muscles of thigh and anastomoses with popliteal artery [1, 2]. Interventional radiology is new technique to study the variations of the courses of the PFA. The anatomical knowledge of the site of origin of PFA is useful in avoiding iatrogenic femoral arterio-venous fistula formed during puncture of femoral artery [3]. Apart from this, PFA is used for haemodialysis, vascular reconstructive procedures and various Radio Imaging techniques like Ultrasound Doppler Imaging and MRI [4, 5]. We observed two cases of abnormal configuration and branching pattern of FA and PFA. As elaborated above, the variant courses of FA and PFA play crucial role in diagnosis and treatment of pathologies related to these arteries in addition to variant anatomy. Therefore the cases are reported.
2. Case Report
- Femoral triangles of two female cadavers embalmed in 10% formalin were dissected for teaching undergraduate medical students in the department of anatomy AIIMS Rishikesh. Abnormal configuration of FA, PFA and their branches were observed as illustrated below: Case-1: On right side of a female cadaver aged 75 years, a common stump separated from FA from its posterior aspect at a distance of 3cm from the inguinal ligament. This common stump instantly trifurcated into MCFA, PFA and LCFA (Fig.1).
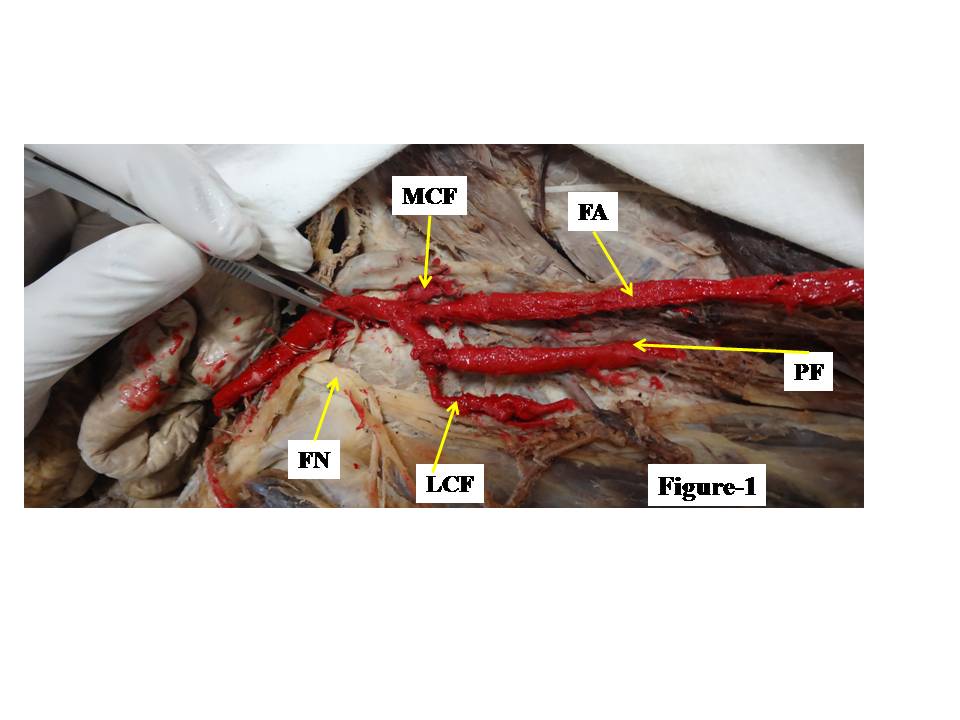 | Figure 1. Profunda femoris and two circumflex arteries arising as common stump from femoral artery (Trifurcation). FA- femoral artery, MCF- medial circumflex artery, LCF- lateral circumflex artery, PF- profunda femoris artery, FN- femoral nerve |
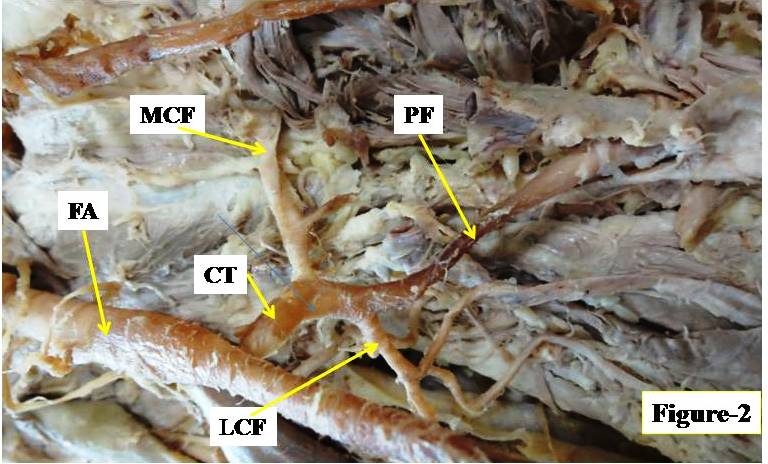 | Figure 2. Showing medial circumflex arising from common trunk which later bifurcated into profunda femoris and lateral circumflex arteries. FA- femoral artery, CT- common trunk, MCF- medial circumflex artery, LCF- lateral circumflex artery, PF- profunda femoris artery |
3. Discussion
- Variations in the branching pattern of FA, PFA are not uncommon and cause clinical complications during various therapeutic and surgical procedures around femoral triangle. We observed two cases with variations in the branching pattern of FA and PFA as described in case report section. Instant trifurcation of the common stump from FA into PFA, medial and lateral circumflex arteries was reported by Sangeeta et al. [6] similar to our first case. But there is variation in the origin of common stump from FA. The origin was observed in Sangeeta et al.’s cases, “either at a low origin (46 mm) or at a high origin (10 mm) from inguinal ligament” whereas it was detected at 3 cm below the inguinal ligament in present study which is neither at low origin nor at high origin. In our second case, common trunk arose from FA at 4.5 cm distal to inguinal ligament. This common trunk after descending for 2.5 cm gave rise to MCFA. Common trunk then travelling for 1 cm further bifurcated into LCFA and PFA. This is altogether different configuration of LCFA, PFA and MCFA not described in literature. Moreover profunda femoris artery arose about 8 cm below the inguinal ligament. Such low origin of PFA is not reported in literature and is new and unique finding having greater bearing on iatrogenic interventions. The knowledge of the site of origin of PFA is important while performing clinical procedures in the femoral region and in hip joint replacement and also for avoiding iatrogenic arterio venous fistula or severe secondary haemorrhage while performing femoral artery puncture [7]. The different anatomical relationships and lack of knowledge of variations of these vessels make the haemostasis difficult to manage [8]. Level of origin of PFA should be taken into account while performing femoral vessel puncture and femoral nerve block. Branching pattern of PFA is also essential while carrying out femoral vessel cannulation as it may cause pseudo-aneurysm. Study of variation in the origin of PFA, its configuration and branching pattern is essential for preventing flap necrosis, particularly tensor fascia latae, when used in plastic and reconstructive surgery and other vascular procedures [3, 9]. The knowledge of these variations is also essential in the surgical repair of femoral hernias, in vascular reconstructive procedures in the proximal leg. Plastic surgeons use the muscular branches while incorporating myocutaneous flaps. Thus the variations in branching pattern of PFA enhance importance.
4. Conclusions
- The surgeons must be aware of variations in level of origin and branching pattern of PFA to avoid iatrogenic complications. This knowledge is also useful to radiologists in interpreting radiographs and to anatomists for new and rare variations.