-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2015; 4(3): 35-37
doi:10.5923/j.medicine.20150403.01
High Origin of Left Testicular Artery with Bifid Ureter
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLArvind Kumar Pankaj1, Rajani Singh2
1Department of Anatomy, KG Medical University, Lucknow, India
2Department of Anatomy, AIIMS Rishikesh, Rishikesh, India
Correspondence to: Rajani Singh, Department of Anatomy, AIIMS Rishikesh, Rishikesh, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Gonadal arteries arise from anterior surface of the aorta below the renal vein at the level of L2 vertebra, 2.5-5 cm below the renal artery. The testicular artery supplies the perirenal fat, ureter and the cremaster muscle. Variations associated with testicular arteries are reported for rare occurrence. During routine anatomical dissection of abdominal region of a middle aged male cadaver in the department of anatomy, KG Medical University, high origin of left testicular artery was encountered. The left testicular artery arose from anterolateral aspect of abdominal aorta above the left renal artery. The artery arched over ipsilateral left renal vein. Near the hilum of left kidney, left testicular artery gave rise to two accessory renal arteries which entered the left kidney near the hilum. Variations in the origin, course and branches of the testicular arteries are attributed to their embryology. The anomalies of testicular arteries are clinically important in surgical procedures like renal transplantation, ureter surgery, vascular pedicles of kidney and in angiographic interventions.
Keywords: Testicular artery, Abdominal aorta, Renal vein, Accessory renal arteries
Cite this paper: Arvind Kumar Pankaj, Rajani Singh, High Origin of Left Testicular Artery with Bifid Ureter, Basic Sciences of Medicine , Vol. 4 No. 3, 2015, pp. 35-37. doi: 10.5923/j.medicine.20150403.01.
1. Introduction
- Gonadal arteries arise from anterior surface of the abdominal aorta below the renal vein at the level of L2 vertebra, 2.5-5 cm below the renal artery [1]. In the abdomen, the testicular artery supplies the perirenal fat, ureter. In the inguinal canal, it supplies the cremaster muscle [2]. Variations relating to origin, course and number of these arteries have been reported in a number of studies [1, 2, 3, 4]. Notkovich (1956) [5] classified the gonadal arteries into three categories based on their relationship with the renal vein. In type I, the gonadal arteries arise from the anterolateral aspect of the abdominal aorta caudal to renal veins [6]. In type II, the gonadal arteries arise cranial to the renal veins. In type III the gonadal arteries emerge caudal to renal veins and arch around them and right gonadal artery was retrocaval.In the present case, we discuss the occurrence of testicular artery arising from abdominal aorta not reported in literature.
2. Case Report
- During routine anatomical dissection of a middle aged male cadaver, left testicular artery arose from anterolateral aspect of abdominal artery above the renal artery (figure-1).
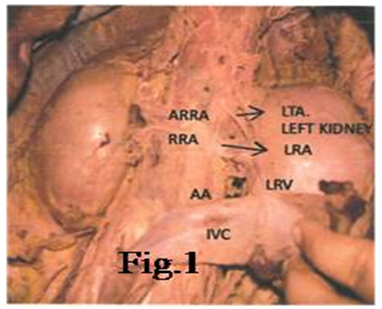 | Figure 1. Shows high origin of testicular artery |
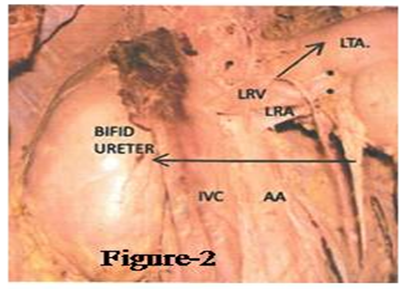 | Figure 2. Showing bifid ureter |
3. Discussion
- Variations in the origin, course and branches of the testicular arteries are attributed to their embryology. Shinohara et al. described the left testicular artery originating from the aorta as high as one cm cranial to the origin of the left inferior phrenic artery [7]. High origin of testicular artery arching in front of renal vein has been described by various authors [8, 9]. Notkovich (1956) classified variations in the origin of testicular artery into three types [5]. In the present case, testicular artery arose from abdominal aorta above the renal vein which is equated with type II of the Notkovich series on the left side. But the difference is that, in the current study, artery arose above the renal vein and artery both and it is associated with bifid left ureter and lobulated left kidey not reported so far. Also it gave rise to two accessory renal arteries. All these variations occurring simultaneously in a single cadaver is a rare phenomenon. The developmental origin of testicular blood vessels is very complex [10]. The first description on the embryological origin of the gonadal artery was given by Felix in 1912 [11]. Nine lateral mesonephric arteries are divided into cranial, middle and caudal groups. One of the caudal arteries persists and differentiates into definitive gonadal artery. The persistence of a cranial lateral mesonephric artery results in high origin of gonadal artery [11]. High origin of testicular artery observed in present case may be due to persistence of cranial lateral mesonephric artery.Genetics, various chemical agents, growth/transcription factors may take part in the selection and persistence of a congenital vascular channel [12, 13]. Surgeons should take into account the aberrant origin and course of gonadal arteries when operating near a renal pedicle or in the retroperitoneum. Precise knowledge of these variations and their relations to the adjacent structures is important in avoiding the complications in operative surgery. Moreover, arched gonadal artery may compress the renal vein leading to varicocele and may also be a possible aetiological factor in orthostatic albuminuria and may also influence the direction of blood flow from kidneys and gonads [5, 14].
4. Conclusions
- Variations in the origin, course and branches of the testicular arteries are attributed to their embryology. The anomalies of testicular arteries are clinically important in surgical procedures like renal transplantation, ureter surgery, vascular pedicles of kidney and in angiographic interventions.