-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2015; 4(2): 31-34
doi:10.5923/j.medicine.20150402.03
Effect of Smoking on Pulmonary Functions among Male Saudi Adolescents
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAhmed Sayed Khashaba
Assistant Professor- Physiology Medicine, Riyadh Colleges of Dentistry and Pharmacy
Correspondence to: Ahmed Sayed Khashaba, Assistant Professor- Physiology Medicine, Riyadh Colleges of Dentistry and Pharmacy.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
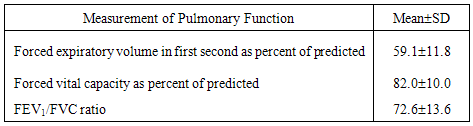
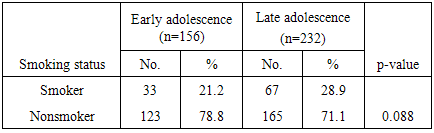
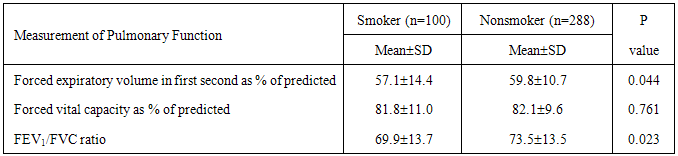
Objective: To estimate the current prevalence of cigarette smoking among Saudi male adolescents attending primary health care centers in Riyadh City, Saudi Arabia and its possible impact on their pulmonary function. Methods: The study followed a cross sectional design. Following a consecutive sample, a total of 388 Saudi male adolescents attending primary health care centers in Riyadh City, Saudi Arabia were included in this study. Spirometry was applied to all participants. Pulmonary function testing was performed. Common measurements included: forced expiratory volume for the 1st second (FEV1); forced vital capacity (FVC) and the ratio between FEV1 and FVC (FEV1/FVC). Pulmonary function tests were performed three times for each subject. The average for the three readings was calculated. The percentages of predicted values for FVC and FEV1 were calculated. Results:More than half of participants were overweight/ obese (56.7%). About one fourth of adolescents (25.8%) were smokers. Percent of predicted forced expiratory volume in first second (MeanSD) was 59.1±11.8%. Percent of predicted forced vital capacity (MeanSD) was 82.010.0 while the FEV1/FVC ratio (MeanSD) was 72.613.6. Prevalence of smoking was higher among older adolescents (28.9%) than younger adolescents (21.2%). Forced expiratory volume in first second (as % of predicted), forced vital capacity (as a percent of predicted) and FEV1/FVC ratio were lower among smoker adolescent participants (p=0.044, p=0.761 and p=0.023, respectively). Conclusions: Prevalence of smoking among Saudi male adolescents is high. It starts mainly during early adolescence. There is a significant rapid decline in lung function among adolescent smokers as compared to non-smokers. Interventions to prevent tobacco use among adolescents are highly needed.
Keywords: Smoking Pulmonary Physiology
Cite this paper: Ahmed Sayed Khashaba, Effect of Smoking on Pulmonary Functions among Male Saudi Adolescents, Basic Sciences of Medicine , Vol. 4 No. 2, 2015, pp. 31-34. doi: 10.5923/j.medicine.20150402.03.
1. Background
- Cigarette smoking has been known to cause significant adverse effects on various organ systems, e.g., severe cardiovascular, cerebrovascular and pulmonary adverse effects. When a person smokes, the tobacco smoke passes through the nasal passage and reaches the alveoli. The tobacco particles get absorbed with other gases and diffuse in the respiratory passage and the alveoli. Various tobacco toxins spread to every site of the respiratory tract [1]. Cigarette smoking and its health consequences represents one of the most serious public health problems and represents an important health challenge worldwide [1]. Evidence is accumulating that smoking increases the risk of nearly all types of cancers and cardiovascular diseases [2]. In the last two decades, adolescents have become more exposed to tobacco promotion and marketing at early ages [3], and most smokers have reported that they began smoking before the age of 18 years [4-6].Al-Rukban [7] stated that obesity constitutes an important public health problem among male adolescents in Riyadh. He reported that almost half of Saudi male adolescents have high body mass index. Al-Shehri et al. [8] demonstrated that overweight and obesity in Saudi Arabia is a serious public health problem, especially among adolescents. The prevalence is on the rise, and the need for interventions is becoming urgent.Among the population aged 15 years or more in Saudi Arabia, approximately 37.6% of males are current smokers [3]. According to Bassiony [9], the prevalence of cigarette smoking among secondary school students is 12-29.8%, and among university students, it is 2.4-37%. Nevertheless, despite several published studies on smoking among Saudi adolescents, there is still a wide gap in literature about Saudi adolescent smoking [10]. Gold et al. [11] noted that, even in teenagers who have been smoking for few years, there is a measurable airway obstruction. It is believed that decline in pulmonary function tests is irreversible [12].Canoy et al. [13] stated that obesity significantly impairs respiratory function. Al-Makadma and Moynihan [14] added that the initiation of smoking behavior during adolescence is associated with significantly negative effects on the respiratory system. Therefore, in a potentially obese population of Saudi adolescents, it is a pressing necessity to assess the impact of early smoking initiation on their respiratory function.The present study aimed to estimate the current prevalence of cigarette smoking among male adolescents attending primary health care centers in Riyadh City, Saudi Arabia and its possible impact on their pulmonary function.
2. Methodology
- The study followed a cross sectional design. Following a consecutive sample, a total of 388 Saudi male adolescents attending primary health care centers in Riyadh City, Saudi Arabia were included in this study. Collected data included personal characteristics (i.e., age and smoking status) and measures of pulmonary function tests (i.e., FEV1 and FVC as percentages of predicted values and FEV1/FVC ratio). The duration of the study was 3 months i.e. from September to November 2014. The inclusion criteria were being Saudi, male adolescent (i.e., aged 10-19 years) [15]. Female adolescents were excluded from the study sample since prevalence of smoking among female adolescents has been reported to be negligible, i.e., 0.7% [16]. Moreover, patients with chronic diseases (e.g., diabetes, bronchial asthma) were excluded in the study.Participants' height and weight were measured without shoes and wearing light clothes using digital scales and a portable stadiometer. Height and weight were measured to the nearest 1 cm and 0.1 kg, respectively. The body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). According to the World Health Organization [17], participants aged 18 years and older, overweight and obesity were considered if BMI ≥25 kg/m2). For participants aged under 18 years, BMI cut-offs for overweight and obesity were used, as defined by Cole et al. [18]. For the purpose of this study, participants' BMI classification was dichotomized into non-overweight or overweight/obese.Spirometry was applied to all participants using the Spirolab III machine. Before testing, the required maneuvers were demonstrated by the researcher. Pulmonary function testing was performed using the acceptability standards outlined by the American Thoracic Society [19] with subjects in a standing position and wearing nose clips. Common measurements included: forced expiratory volume for the 1st second (FEV1); forced vital capacity (FVC) and the ratio between FEV1 and FVC (FEV1/FVC). Pulmonary function tests were performed three times for each subject. The average for the three readings was calculated. The percentages of predicted values for FVC and FEV1 were calculated..The statistical analysis for collected data was carried out using the Statistical Package of Social Sciences (SPSS) version 21. Descriptive statistics (i.e., frequency and percentage) were calculated. Tests of statistical significance were applied (i.e., chi square and independent sample t-test). P-values less than 0.05 were considered as statistically significant.
3. Results
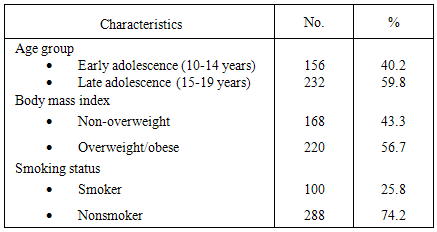
- Table (1) shows that 40.2% of participants adolescents aged 10-14 years, while 59.8% aged 15-19 years. More than half of participants were overweight/ obese (56.7%). About one fourth of adolescents (25.8%) were smokers.
|
|
|
|
4. Discussion
- Adolescence is a critical period in the formation of smoking habits, with most smokers starting during their teenage years. Most persons who have smoked cigarettes on a daily basis reported having smoked their first cigarette before the age of 15 years [16]. The high prevalence of obesity among Saudi adolescents provides a baseline significant negative effect on their respiratory function. Therefore, this study aimed to assess the impact of early smoking initiation on respiratory function of male Saudi adolescents.More than half of adolescent participants in this study were overweight/obese (56.7%). This high prevalence of obesity among male adolescents is in agreement with that of Al-Rukban [7], who reported that the prevalence of overweight among male adolescents in Riyadh City was 13.8% and obesity was 20.5%. El-Mouzan et al. [20] reported that the prevalence rates for overweight and obesity among a national sample of 19,317 healthy adolescents in Saudi Arabia was 23.1%, and 11.3%, respectively. Results of this study showed that prevalence of smoking among Saudi male adolescents was as high as 25.8%. A similar high prevalence of adolescents’ cigarette smoking was also reported in recent Saudi studies. In Riyadh, Saudi Arabia, Al-Ghobain et al. [2] and Al-Nohair [21] reported that prevalence of adolescent smoking was 31% and 29%, respectively.This study showed that percent of predicted forced expiratory volume in first second (MeanSD) was quite low (59.111.8%). This low value may be explained by the expected negative impact of overweight/obesity on respiratory function of adolescents. Canoy et al. [13] stated that FEV1 is linearly and inversely related across the entire range of waist: hip ratio, as an index of obesity. Moreover, Jones et al. [22] reported significant inverse relationships between BMI and FEV1. Joshi et al. [23] stated that, in males, the percentage of body fat showed negative correlation with FEV1. Overweight and obese children showed 20% to 46% reduction in FEV1 depending upon their degree of obesity. Results of the present study showed that prevalence of smoking among adolescents did not differ significantly according to stage of adolescence. This finding indicates that smoking mainly starts at early adolescence. Studies report different ages at which children start smoking. Elders et al. [24] stated that the average trial for smoking is at the age of 14.5 years. Breslau and Peterson [25] found that 34% of children had their first cigarette at or before the age of 13 years, and another 43% initiated smoking between 14-16 years old. Jackson and Henriksen [26] reported that 21% of adolescents started smoking at the age of 10-11 years. The Centers for Disease Control and Prevention [27] indicated that only 8% had initiated use before the age of 11 years. Park [28] stated that many adolescents start smoking at a young age, out of curiosity and a spirit of adventure, only to become addicted to it.This study showed that all measures of pulmonary function were lower among smoker adolescent participants. This finding is in agreement with those of reported by several studies. Abdalla et al. [16] noted that adolescents who smoke are more likely to have a variety of health problem, including upper respiratory tract infections, reduced lung growth and retardation of lung function. Respiratory function tests indicate deterioration of respiratory function prior to the appearance of clinical symptoms, and their results can be used to prevent or reduce the incidence of respiratory diseases [29-30]. The rate of decline in lung function of smokers is rapid as compared to non-smokers [31]. In conclusion, the prevalence of smoking among Saudi male adolescents is high. It starts mainly during early adolescence. There is a significant rapid decline in lung function among adolescent smokers as compared to non-smokers. Interventions to prevent tobacco use among adolescents are highly needed.