-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Basic Sciences of Medicine
p-ISSN: 2167-7344 e-ISSN: 2167-7352
2015; 4(1): 1-4
doi:10.5923/j.medicine.20150401.01
Abnormal Superficial Radial Artery and Related Vessels
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajani Singh1, R. Shane Tubbs2
1Department of Anatomy, AIIMS, Rishikesh, India
2Department of Pediatric Neurosurgery, Childern’s of Alabama, Birmingham AL, USA
Correspondence to: Rajani Singh, Department of Anatomy, AIIMS, Rishikesh, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
The brachial artery is a continuation of the axillary artery. It terminates at the level of the neck of the radius by dividing into the radial and ulnar arteries. The radial artery courses deep to brachioradialis muscle and it becomes superficial in the lower part of forearm. Twenty six matched upper limbs were dissected in the Department of anatomy. In one of the upper limbs, the radial artery aberrantly arose from the 3rd part of the axillary artery. It coursed superficially through the arm and forearm. In the arm, it ran medial to the axillary artery and median nerve and anterior to the ulnar nerve. At the level of the elbow, it crossed to the lateral side superficial to the flexor muscles of the forearm. Throughout its course it gave no branches. The brachial artery aberrantly gave the radial recurrent artery 3.5 cm above the elbow and also terminated anomalously at the neck of the radius by dividing into the common interosseous and ulnar arteries. The simultaneous occurrence of all these variations has not been described previously as far as known to the author. Cause of such variation may be developmental and genetic. Superficial radial artery may be mistaken for veins and intended intravenous injection may lead to intrarterial injection. Further such variation may cause misinterpretation of radiographs. Therefore knowledge of such variation of superficial radial artery will be useful for vascular surgeons, radiologists and anatomists.
Keywords: Brachial artery, Radial artery, Superficial course, Common interosseous artery
Cite this paper: Rajani Singh, R. Shane Tubbs, Abnormal Superficial Radial Artery and Related Vessels, Basic Sciences of Medicine , Vol. 4 No. 1, 2015, pp. 1-4. doi: 10.5923/j.medicine.20150401.01.
1. Introduction
- The brachial artery (BA) is a continuation of the axillary artery (AA), which is an extension of the subclavian artery. The BA bifurcates into the radial and ulnar arteries at the neck of the radius. Radial recurrent artery arises from Radial artery (RA) in cubital fossa. In the upper part of the forearm, the RA lies under the cover of the brachioradialis muscle and in the lower part it becomes superficial under the cover of the skin and fascia. This is the normal configuration of RA. A rare variant bifurcation of AA into radial and brachial arteries at a new location, then anomalous course of RA and abnormal terminal bifurcation of BA into common interosseous and ulnar arteries at the neck of radius are rare variant configurations of these arteries. These variant configurations of arteries are very important for diagnosis and treatment of diseases of the upper limb, challenging the surgeons for surgical interventions and radiologists to interpret normal and contrast radiographs pertaining to these vessels. The superficial arteries of the upper extremity can be mistaken for veins, potentially leading to intraarterial injections instead of the intended intravenous injections [1, 2] causing injury to the artery.The multivariant case is reported here because of clinical significance elaborated above and rarity of the newly detected configuration of these arteries.
2. Case Report
- Twenty six upper limbs (13 left and 13 right) fixed in 10% formalin were dissected in the Department of Anatomy during teaching of undergraduate medical students. In one right upper limb from a 75 year old male cadaver, the following anomalies were detected-1. Abnormal origin and course of the radial artery,2. Anomalously originating radial recurrent artery,3. Aberrant branching pattern of the brachial artery into common interosseous and ulnar arteries at its termination point. Abnormal origin and course of the radial arteryThe radial artery, with a diameter of 4mm at the origin, arose from the 3rd part of the AA just below the lower border of the pectoralis minor measuring 2.5 cm above the point where the median nerve was formed (Fig.1). This artery was superficial throughout its course from its origin to the dorsum of the hand travelling under the cover of the skin and fascia only. It descended anterior to the ulnar nerve up to the cubital fossa and remained medial to the AA in the axilla, and the BA and median nerve in the arm (Fig.1 and 2). At the level of the elbow, it crossed the superficial flexor muscles from the medial to the lateral side (Fig.1 and 2) and passed deep to the abductor and extensor tendons of the thumb then entered the palm through the 1st intermetacarpal space. It gave no branch in either the arm or the forearm. Anomalously originating radial recurrent arteryNormally the radial recurrent artery arises from the radial artery, but in the present case it arose from the brachial artery 3.5 cm above its termination (Fig.1). This is a new variation in the origin of the radial recurrent artery. Aberrant branching pattern of the brachial artery at its termination pointNormally, the BA at its termination point branches into the radial and ulnar arteries, but in this case, it bifurcated into the ulnar and abnormal common interosseous arteries (Fig. 2). Normally, the common interosseous artery arises from the ulnar artery. In this case the ulnar artery was hypoplastic with a diameter of 3mm at the origin. The diameter of the common interosseous artery was 3mm and that of the BA was 6mm at its origin. The radial artery took an aberrant course in one of the 26 upper limbs (3.85%). There was no other abnormality in the limb on this (right) side. These arteries followed normal courses in the left upper limb.
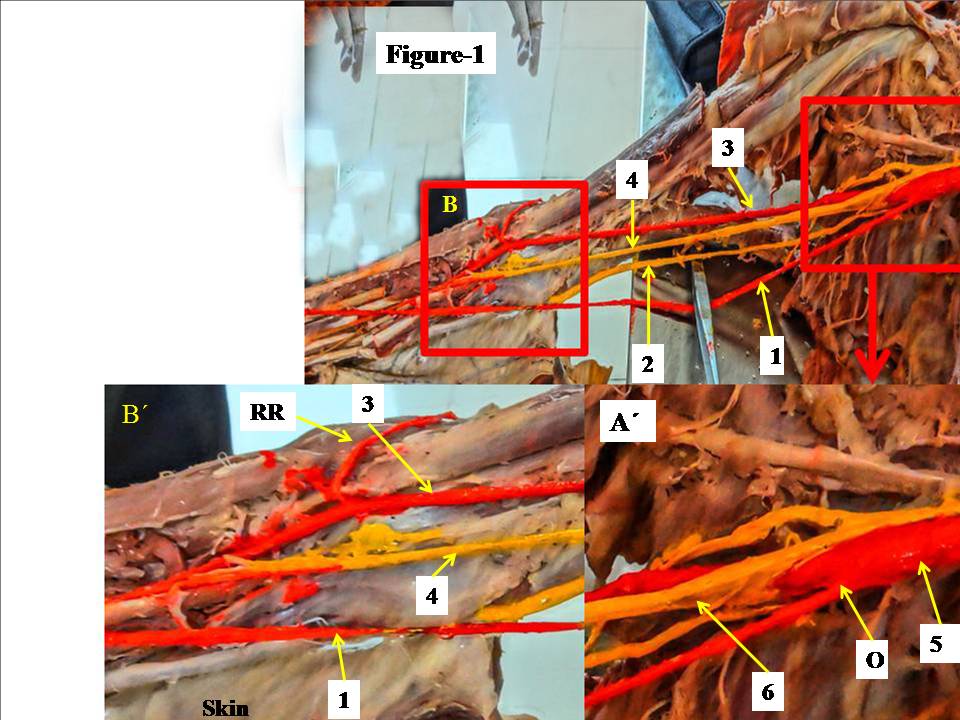 | Figure 1. Shows the origin and course of the superficial radial artery in the arm and forearm. The superficial radial artery is anterior to ulnar nerve and medial to median nerve. The structures are separated by forceps for better identification. Box A´ is magnified view of A showing origin of superficial radial artery and point of formation of median nerve. Box B´ is magnified view of B showing origin of radial recurrent artery from brachial artery. Superficial radial artery is also seen crossing from medial to lateral side at the elbow. 1-superficial radial artery, 2-ulnar nerve, 3- brachial artery, 4-median nerve, 5-axillary artery, O- origin of radial artery from axillary artery, 6- point of formation of median nerve |
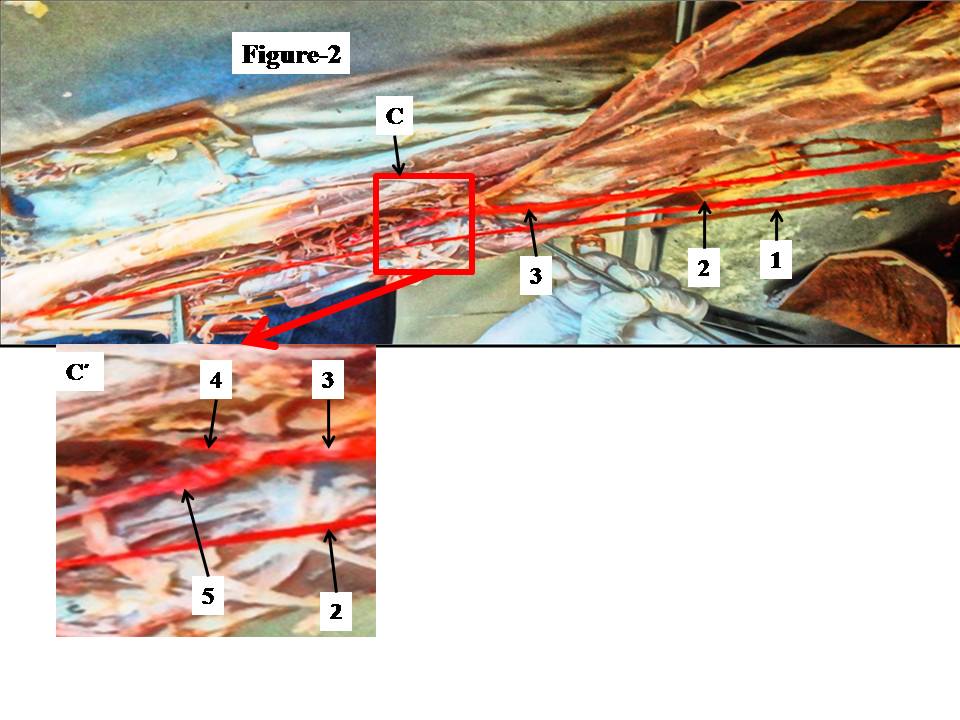 | Figure 2. Shows the course of superficial radial artery in arm and forearm. Box C´ is magnified view of C around cubital fossa showing origin of the common interosseous and ulnar arteries from brachial arterty in the cubital fossa. 1- ulnar nerve. 2- superficial radial artery, 3- brachial artery,4- common interosseous artery, 5-ulnar artery |
3. Discussion
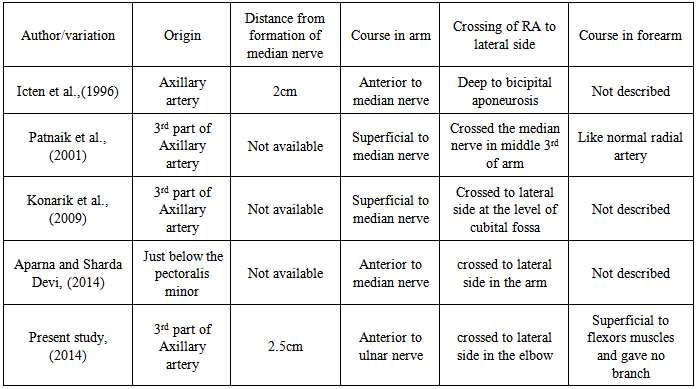
- The arm is supplied by brachial artery and forearm by radial and ulnar arteries and their branches. The RA is normally a terminal branch of the BA arising in the cubital fossa at the level of the neck of the radius. Although variations in the origin and configuration of the radial artery are not uncommon yet the present case is worth reporting as it exhibits new anatomical features in relation to its origin and superficial course.An origin of the RA from the AA was found in 2.13% [3], 12.5% [4] and 3.85% in the present study. This range of incidences could be attributable to differences in sample size or to studies of live patients versus cadavers.Variations in the origin of the RA from the AA and its pattern of course have been reported [5-8] (see Table-1).
|
4. Conclusions
- Simultaneous occurrence of variations in the origin and course of superficial radial artery along with origination of recurrent radial artery from brachial artery observed in present case are clinically significant for diagnostic, interventional and surgical procedures as described in clinical significance section. Thus knowledge of the variations of the radial artery is of paramount importance to vascular surgeons, radiologists and anatomists.