-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Materials Science
p-ISSN: 2162-9382 e-ISSN: 2162-8424
2020; 10(1): 9-14
doi:10.5923/j.materials.20201001.02

Use of EDTA Improves the Quality of Root Canal Filling in Artificial Lateral Canals
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLStephanie Quadros Tonelli1, Janir Alves Soares2, Eduardo Nunes1, Juliana Francisca Grossi Heleno1, Marcelo Garcia de Carvalho1, Frank Ferreira Silveira1, 3
1Department of Dentistry, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil
2Department of Dentistry, Federal University of Vales do Jequitinhonha e Mucuri, Diamantina, MG, Brazil
3Department of Dentistry, University of Itaúna, Itaúna, MG, Brazil
Correspondence to: Frank Ferreira Silveira, Department of Dentistry, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study aimed to evaluate the influence of Ca(OH)2 intracanal and irrigation protocol on posterior filling in artificial lateral root canal. Thirty unirradicular extracted human teeth were selected and amplified apically to #45 K file under abundant irrigation with 5.25% NaOCl. NiTi K3 15.02 was used to construct artificial lateral canals on each third of the proximal surfaces (n=180). The root canals of group A (n=60) were filled with gutta-percha and Pulp Canal Sealer by the technique of System B + Obtura II. In group B (n=60), before filling, calcium hydroxide intracanal was applied over a period of seven days, and posterior removed with apical file # 45 and the patented file # 15, with smooth rotary movements, aided by 10mL 5.25% NaOCl at 5-minute intervals. In group C (n=60), procedures were similar to those in group B, except irrigation was performed with 5.25% NaOCl, alternating with 3mL of 17% EDTA, with subsequent filling and evaluation by using digital imaging system. The percentage of completely filled simulated root canals in groups A, B and C was 83.3%, 43.3% and 80.0%, respectively. Regardless of the root segment, a similar filling was obtained in groups A and C (p> 0.05), which were statistically superior to group B (p < 0.05). Intracanal calcium hydroxide interfered negatively in artificial lateral root canal filling. However, this drawback was completely reversed by the association of irrigators with a main apical rotatory endodontic file.
Keywords: Calcium hydroxide, EDTA, Root Canal Filling, Root Canal Irrigants
Cite this paper: Stephanie Quadros Tonelli, Janir Alves Soares, Eduardo Nunes, Juliana Francisca Grossi Heleno, Marcelo Garcia de Carvalho, Frank Ferreira Silveira, Use of EDTA Improves the Quality of Root Canal Filling in Artificial Lateral Canals, American Journal of Materials Science, Vol. 10 No. 1, 2020, pp. 9-14. doi: 10.5923/j.materials.20201001.02.
Article Outline
1. Introduction
- The complex anatomy of root canal system, including curvatures, atresia and many other ramifications, such as lateral canals presents challenge to endodontic treatment. Ramifications present a high occurrence in all dental groups and are more common in apical thirds [1-4]. To ensure successful endodontic treatment, this link between endodontics and periodontics need to be cleaned, disinfected, as well filled [3,4]. The incapacity of mechanical archives to access these areas, makes imperative the use of irrigation solution and dressing intracanal before hermetic filling of these sites [4,5]. Calcium hydroxide - Ca(OH)2 - is steel the dressing intracanal more commonly recommended, because its potential of disinfecting the dentinal tubule system [4]. Satisfactory clinical, radiographic, microbiological and histopathological results have been obtained in periods ranging from one week to several months [3,5-7]. Nonetheless, Goldberg et al. [8] reported a negative influence on simulated lateral root canal fillings. Indicating that Ca(OH)2 must be completely removed from the root canal walls to allow a satisfactory root canal filling. In addition, another problem with intracanal calcium hydroxide impregnation is that it can affect the accuracy and precision of apical locators [9]. In this sense, cleaning strategies should be employed to maximize the removal of Ca(OH)2 intracanal [4,5]. Furthermore, to ensure adequate obturation, the thermoplastic gutta-percha has been reported as a technique capable of better perspectives regarding the complete and three-dimensional filling of the entire root canal system [4,5,10,11].Understanding the importance of dressing in diverse clinical-pathological situations and the necessity of fillings in the ramifications of the radicular root canal system, the present study aims to verify whether or not the irrigation regime for the removal of Ca(OH)2 is capable of influencing the posterior filling of the simulated lateral root canal.
2. Experimental Procedure
- The present study protocol was reviewed and approved by the Institutional Review Board of Pontifical Catholic University of Minas Gerais (approval No. 0292.0.213.000-10).
2.1. Teeth selection
- Thirty human extracted premolars uniradicular were selected by means of periapical digital radiography (Shick Elite®, Sirona, New York, United States), in order to exclude teeth with previous endodontic treatments, abrupt curvatures, incomplete rhizogenesis and calcifications. The specimens were previously maintained in a 0.5% thymol solution for 30 days.
2.2. Artificial Root Canals and Endodontic Treatment
- After coronary access using diamond bur #1015 and #3195 (KG Sorensen, Barueri, São Paulo, Brazil), the canals were pre-enlarged with K-files and Gates-glidden drills #1, #2, and #3 (Pulpdent Corporation, Watertown, MA). Later, apical patency and the length of the root canal patency were obtained with a K-file #15. The work length (WL) was established at 1mm beyond the root apex. The canals were prepared with Step-back method, with 5.25% NaOCl irrigation by means of a disposable syringe attached to a thin needle, gauge #30. Two mL of irrigation were used after using each steel file. Subsequently, with a NiTi K3 steel file (Sybron Dental Specialties-Kerr, Mexico) with tip size #15 and taper .02, one artificial lateral root canal was constructed in each third of the proximal surfaces, totalling 180 simulated root canals.
2.3. Radicular Root Canal Filling
- Preceding the obturation, the radicular root canals were dried with absorbent paper cones and divided equally in three experimental groups (A, B and C).
2.3.1. Group A
- In the obturation of these radicular root canals, the gutta-percha Medium cone was used (Odous, Belo Horizonte, Brazil) through the calibration of the its Do point on a millimetric ruler (Maillefer/Dentsply, RJ, Rio de Janeiro, Brazil), equivalent to the diameter of #45, followed by a cut made by a scalpel #15 blade. After radiographic confirmation of its adaptation, the master cones were dipped in Pulp Canal Sealer cement (Kerr Sybron Dental Specialties, Romulus, USA) and fitted to the working length. The System B (Analytic Technology, Redmond, Washington, USA) heat source was activated and a preheated MF Buchanan plug was inserted into the root canal to thermoplastic and compact the gutta-percha at the apical third. The middle and coronal thirds were backfilled using Obtura II (Spartan, Fenton, USA). The coronary sealing consisted of the placing of a cotton ball in the pulp chamber, followed by provisional sealing with zinc oxide-eugenol cement (S.S. White, Rio de Janeiro, RJ, Brazil), in an area of 3mm.
2.3.2. Group B
- Before obturation, the radicular root canals were dressed with a Ca(OH)2 paste (Labsynth Ltda, São Paulo, SP, Brazil) mixed with distilled water in a tooth paste consistency of approximately 0.9g/mL. With the aid of a spiral Lentulo #2, the radicular root canals were completely filled and confirmed radiographically. After coronary sealing, the specimens were stored in an incubator at 37°C in 100% humidity. After a 7-day period, the calcium hydroxide paste was removed from the canal using 10 mL of 5.25% NaOCl, aided by a K file #45, alternating with the use of a steel file of apical patency #15, executing 10 rotatory movements at an amplitude of ¼ and ½ of a rotation. This operatory stage was concluded in 5 minutes. In sequence, after drying, the radicular root canals were filled in a similar manner.
2.3.3. Group C
- Similar to Group B, a calcium hydroxide dressing intracanal was used for one week. However, for its removal, an irrigation protocol was used: (1) irrigation using 5mL 5.25% NaOCl, (2) alternating with 3mL of a 17% EDTA aqueous solution (Biodinâmica Laboratórios, São Paulo, Brazil), pH 7.2, for a 5-minute period, activated by a K-file #15, and (3) last irrigation using 5mL 5.25% NaOCl. Then drying and filling were performed as described in previous group.
2.4. Radiographic Analysis of the Simulated Root Canal Fillings
- In sequence, the teeth were radiographed by the digital system in the ortho-radial angle (AcuRay Digital X-Ray System, Digora, USA) and simulated root canal obturations analysed by three endodontists, who were blind about the technical phase of the endodontic treatments and who knew nothing about the methodology used. All the analyses were directed by the three trained observers together and reached a consensus diagnosis. For evaluation, only simulated root canals which showed filling material in more than 2/3 of the area in the radiographic image were considered "filled". The others were classified as "unfilled".
2.5. Statistical Analyses
- In this evaluation, the prevalence of "filled"/"unfilled" simulated lateral canals in each group was considered. The differences in the results between groups (A, B and C) were analysed using the Kruskal Wallis test. To compare inter and intragroup differences in relation to root canal third, Wilcoxon test were applied. The statistical calculations were performed by SPSS software (19.0, IBM, Armonk, NY, USA). All statistical calculations were performed by SPSS software (19.0, IBM, Armonk, NY, USA) and P-values <0.05 were considered as statistically significant.
3. Results
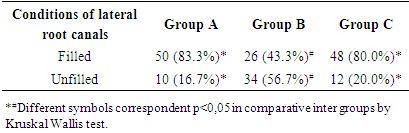
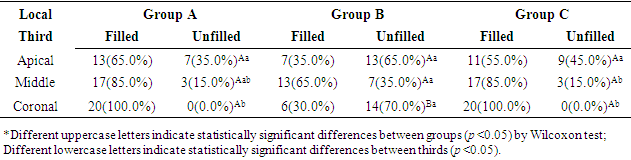
- The radiographic filling pattern of the major root canals and artificial root canals of groups A, B and C is showed in figures 1, 2 and 3, respectively. The prevalence of simulated lateral root canals filled in groups A, B and C was 83.3%, 43.3% and 80.0%, respectively (Table 1). Comparatively, irrigation regimes used in Groups A and C provided similar filling patterns in the artificial lateral root canals (p> 0.05), while those used in group B provided statistically lower results (p <0.05).
|
 | Figure 1. Radiographic image of the radiographic pattern of root canal filling of the artificial canals in a sample from group A |
 | Figure 2. Radiographic image of the radiographic pattern of root canal filling of the artificial canals in a sample from group B |
 | Figure 3. Radiographic image of the radiographic pattern of root canal filling of the artificial canals in a sample from group C |
|
4. Discussion
- The use of intracanal calcium hydroxide improves the prognosis of endodontic treatment due to several biological properties, such as the anti-septic and periapical regeneration inductor, under specific clinical-pathological conditions [5,7]. Nevertheless, before filling the radicular root canals, the need for removal has been argued based on its possible interference on the filling and sealing of the radicular root canal system, as well as the possibility of residual medication being progressively solubilized by the periodontal fluids resulting in the appearance of empty spaces in the interfaces of the obturated tooth. In fact, it has been reported that calcium hydroxide may have the capacity to physically block the dentinal tubules [12] as well as to obstruct the opening of lateral root canals which could impede the complete filling of the radicular root canal system [8]. In contrast with this classical study and our results, Moinzadeh et al. [13] in recent study did not observed the intracanal calcium hydroxide in the quality in the filling root canals. This fact may be occurred because were not considered accessory canal, which presents more difficult to be access by the irrigation solution. In addition, the potential interaction with zinc oxide eugenol sealers could present a potential clinical problem [13,14]. In this way, a complete removal of calcium hydroxide from the root canal before obturation becomes mandatory [15]; however, this represent a challenge in endodontic practice [16,17]. The action of filling lateral root canals is quite complex and can be influenced by a several factors, among which are the prior use of calcium hydroxide [8], the technique of endodontic sealer management [18], diameter of the main cone [19], and the filling technique [8]. In this study, as all radicular root canals received a similar instrumentation pattern, as well as protocol irrigation and filling technique, the differences observed regarding the filling of the artificial root canals can be interpreted in terms of the analysis of the radicular segment, of the chemical nature of irrigators, of the presence of the smear layer, and of the interference of calcium hydroxide in this process.Initially, in this study, the simulated lateral root canals presented diameters compatible with those observed microscopically [20] as well as those from previous in vitro studies [8,10,18,19-23], whose values are approximately 150µm. As regards the radicular segment, it could be observed that of the 56 (93.3%) unfilled artificial root canals, 29 (51.8%) were located in the apical third. Silva and Moraes [24] also reported difficulty in the filling of canals in this critic third. Analysing each group specifically, it could be observed for group A that the permanence of the smear layer may have been the core responsible factor for the block of 10 (16.7%) of the unfilled simulated root canals. Interestingly enough, identical results were obtained in prior study under these same circumstances [11].In accordance with another studies [8,25,26], in group B, it could be observed that the relevant obstructive capacity of the calcium hydroxide reduced or prevented the penetration of the sealer or the gutta-percha into the lateral canals and at a greater magnitude than that presented by the smear layer in group A. Thus, in 34 [56.7%) of the unfilled artificial root canals, as compared to group A, calcium hydroxide was supposedly responsible for the differential in 24 (40.0%) unfilled artificial root canals. Also, in this group, the relative difficult of 5.25% NaOCl was verified upon its removal. Nevertheless, much worse results were reported in a previous study [11]. The results of this study indicate that the use of EDTA as an irrigant in association with NaOCl improves the filling pattern in simulated lateral canals. The superiority of group B, in comparison with the other groups, was due to the higher prevalence of simulated lateral canals filled.In contrast, with the irrigation regime with 5.25% NaOCl solution alternating with 17% EDTA solution and associated with the use of apical final files, it can be observed the same action proportioned a significant removal of calcium hydroxide since 80.0% of the simulated lateral root canals were completely filled. From the chemical point of view, the adopted irrigation regime is similar to that used against the smear layer and, considering the results obtained, the mechanisms must involve: (1) chelating of the calcium ion (17% EDTA chemical action), (2) disorganization of the deposits which adhere to the dentinal walls through the dissolution of the interspersed organic residues (5.25% NaOCl chemical action), (3) dispersion of residues from the paste through the rotation of steel files (mechanical action of the instruments), and (4) the carrying of residues through the soft intracanal flow (physical action of irrigation and suction). Consequently, the irrigation with a 5.25% NaOCl solution, alternating with the irrigation with a 17% EDTA solution, aided by the master apical file and the patency files, with smooth rotating movements over the dentinal walls over a 5-minute period, followed by filling with thermally plasticized gutta-percha, will not cause any damage to the obturation of the endodontic ramifications, as evidenced by the lateral canals. Alternatively, upon focusing on the magnification of the removal of calcium hydroxide using NaOCl and EDTA solutions, we are in fact assessing the energization of the steel files through ultra-sound used at a low potency and at a reduced time interval, like using the passive ultrasonic vibration. Our results are in agreement with a previous study in which it was proven difficult to remove intracanal calcium hydroxide, which, however, was overcome by the use of chelating substances in intracanal irrigation [16].Further highlighting the efficiency of the association used in the present study (EDTA and NaOCl), the same performance was not obtained from the use of other irrigating agents. When comparing the influence of 2.5% NaOCl and 2% chlorhexidine gel on the filling of artificial lateral canals both irrigants had no influence on the filling of artificial lateral canals while Ca(OH)2 dressing influenced negative this filling [27].In contrast, in a recent study, it was shown that despite the negative effect of Ca(OH)2 on obturation, bioceramic repair cements do not change their properties by this intracanal medication [25]. It is important to emphasize that irrigation solution activation devices, such as ultrasonic and laser, have also been recommended to maximize the activity of irrigating substances, especially in order to aid their penetration in the critical areas of the root canal [22,26]. Its use, as well as the use of EDTA, is associated with a greater effectiveness in the removal of intracanal Ca(OH)2 and, consequently, better filling [26-28]. Considering the limitations of this ex vivo study, further researches are required to evaluate other protocols to Ca(OH)2 removal to better filing root canals.
5. Conclusions
- The intracanal Ca(OH)2 interfered in the obturation of artificial lateral root canals at a higher scale than that of the smear layer. Nevertheless, this effect was completely overcome by means of the association of 5.25% NaOCl and 17% EDTA in final irrigation of root canal system, maximizing the use of the master apical and patency files in rotatory instrumentation.
ACKNOWLEDGEMENTS
- The authors would like to thank the financial support given by CAPES for the scholarships granted to the post-graduate students participating in the study.