Vakhidova A. M.1, Khudoyarova G. N.1, Khudzhanova M. A.2, Mamedov A. I.1
1Department of Microbiology, Virology and Immunology, Samarkand State Medical Institute, Samarkand, Uzbekistan
2Assistant of the Department of Normal Physiology, Samarkand State Medical Institute, Samarkand, Uzbekistan
Correspondence to: Vakhidova A. M., Department of Microbiology, Virology and Immunology, Samarkand State Medical Institute, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The purpose of the work. To determine the frequency of complications in immune disorders in patients with echinococcosis, and to study immunocorrective and biostimulating therapeutic measures. Materials and methods of research. Parasitological, histological, biochemical, immunological, serological, ultrasound and X-ray examinations were used. Results. In the early stages of the disease, when clinical manifestations are absent or insignificant, the diagnosis of echinococcosis is particularly difficult. Therefore, uncomplicated echinococcosis is often detected accidentally during preventive examinations. We observed 72 patients with echinococcosis of the lung at the age of 2 to 16 years. Depending on the period of the disease, they were divided into 3 groups: in the initial stage - 3 patients, in the midst of the disease - 36, in the stage of complications - 33 patients. As is known, the most informative method of diagnosing echinococcosis of the lungs is radiography, while a typical picture is observed depending on the stage of the disease and the size of the cyst. Echinococcosis of the lungs is often difficult to differentiate from an abscess and a lung tumor, as well as from pyopneumothorax, pyothorax. Therefore, chest X-ray examination is an important and valuable method for diagnosing lung echinococcosis, but it is not without drawbacks: its use does not allow to detect lung echinococcosis with a 100% guarantee. In 5.8% of the observations, diagnostic errors were made. But the most reliable methods of diagnosing echinococcosis, or rather the presence of echinococcus in the body, are immunological. In the experiment, the sensitivity and specificity of RLA, RNGA, ELISA, TIM, and PCR were tested on a sufficient number of animals of different species. However, the specificity of these reactions did not exceed 82%, with the exception of RSKP (accuracy of readings up to 94.5%), which corresponds to the materials of our publications. Conclusions. We noted that the detection and complete recovery from the main disease, complete recovery of working capacity, the absence of any complaints, with X-ray examination-the absence or insignificant area of pneumofibrosis in the lung; in some periods, negative serological reactions (RLA, RNGA, RDDH), as well as long- tomography, ultrasound scanning, radiography) and serological methods is used.
Keywords:
Serological reactions, Echinococcosis, Radiography, Lung, Immune disorders
Cite this paper: Vakhidova A. M., Khudoyarova G. N., Khudzhanova M. A., Mamedov A. I., Immunorehabilitation of Patients with Echinococcosis, Complicated by the Satellites of Echinococcal Cysts-Bacteria, International Journal of Virology and Molecular Biology, Vol. 11 No. 1, 2022, pp. 3-8. doi: 10.5923/j.ijvmb.20221101.02.
1. Introduction
For the diagnosis of echinococcosis, a complex of clinical, instrumental (computed term results were obtained after 1.5-2 years, which indicates that ventilation is being restored in the operated lung. However, it is not easy to identify the pathology. Diagnostic errors occur in 4-8% of cases when abscesses and tumors of the liver, lungs, pleural empyema, etc. are detected during surgery. Since the 70s of the XX century, much attention has been paid to specific methods of immune diagnosis of echinococcosis. However, the analysis of the literature data showed an ambiguous assessment of their diagnostic capabilities. Thus, false-positive and negative results in the reaction of indirect hemagglutination (RNGA) were observed in 17-45% of cases. Thus, the development of new approaches to the immunodiagnostics of echinococcosis in children and adults remains an urgent problem. The influence of morphological modifications of the exciter on the clinical course and outcome of the disease has been poorly studied.The purpose of the work: The goal of surgical intervention is not only to remove the echinococcal cyst in the most gentle way, but also to prevent complications of the disease — residual cavities in the operated organs and relapses of echinococcosis. Despite the large number of options for surgical approaches to the treatment of echinococcosis, the complication rate remains quite high (21%), and the mortality rate among children ranges from 7 to 16%. Given the deep immune disorders in patients with echinococcosis, treatment should be comprehensive and, along with surgical removal of the echinococcal cyst, it should include immunocorrective and biostimulating therapeutic measures. The latter require further development.
2. Materials and Methods of Research
The section is based on the analysis of the treatment results of 287 adult patients with pulmonary echinococcosis and 178 children aged 1 to 16 years with echinococcosis of various localization.Of the 178 children ‒ boys (62%) and 68 girls (38%) ‒ 72 patients (40%) had lung echinococcosis, 67 (38%) ‒ liver, 34 (19%) ‒ combined echinococcosis and 5 (3%) ‒ rare localization of the process. Among 34 patients with combined forms, 28 (82%) were diagnosed with liver and lung damage, in half of the cases ‒ the right lobe of the liver and the right lung.Clinical, radiological, ultrasound, laboratory, parasitological, bacteriological, biochemical, and immunological studies were conducted to diagnose echinococcosis and examine patients. X-ray examination was used mainly for echinococcosis of the lungs, ultrasound - for the diagnosis of echinococcosis of the abdominal cavity and retroperitoneal space (on the device "A1osa-500"). Laboratory tests blood included a general blood and urine test, and a biochemical blood test. To assess the hemostatic system, the clotting time and the number of platelets in the peripheral blood were examined.Serological reactions of latexagglutination, indirect hemagglutination, or double diffusion in agar gel were used to confirm and clarify the diagnosis before surgery and in the long-term period to establish a relapse of the disease. The reaction of latexagglutination, the reaction of indirect hemagglutination was carried out according to the known method.The double diffusion reaction in agar gel was carried out as follows: agar (2-3 ml) was poured on the slide glasses after their thorough treatment with alcohol and the flame of an alcohol lamp. The standard stamp was used to make holes in 30-40 minutes. An echinococcal antigen taken from the bladder was placed in the central well, and the patient's serum was poured into the rest. After filling the wells, the glasses were placed in a desiccator (the reaction took place at room temperature). The result was evaluated visually. With a positive reaction, clear precipitation lines appeared between the wells; with a negative reaction, no such lines were observed. Determination of immunoregulatory subpopulations of T-lymphocytes (T-suppressors, T-helpers) and B-rosette-forming lymphocytes in combination with mouse erythrocytes was carried out according to K. A. Lebedev and I. D. Ponyakina (1990). Immunoglobulins A, M, and G in blood serum were determined by polymerase chain reaction. CEC was detected by the method of precipitation using a 3.5% solution of polyethylene glycol and the results were recorded on a photoelectrocolorimeter.Ultrasound examination of the liver was performed to detect combined lung and liver damage, taking into account the frequency of the latter (the first place among the injuries of all organs and tissues in echinococcosis). The study was performed on an empty stomach after preliminary preparation of the intestine (cleansing enema on the day before and on the day of the study).The effectiveness of scolexoprecipitation (RSCP), latex agglutination (RLA), indirect hemagglutination (RNGA), enzyme immunoassay (ELISA), and point immunological method (TIM) was tested on 98 Karakul sheep, 86 heads of cattle, and 59 pigs spontaneously infected with echinococcosis.
3. The Results of the Study
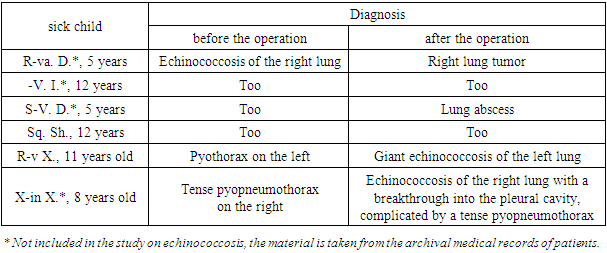
However, each method has both advantages and limitations in its application. Often, the use of classical methods for diagnosing echinococcosis of the lungs, liver and other organs does not allow us to identify echinococcal cysts with complete confidence, since, according to the literature, there are many diseases that radiologically manifest as round-oval shadows in the lungs.There are 3 groups of diagnostic methods: clinical, instrumental, and immunological.It is clear that in the early stages of the disease, when clinical manifestations are absent or insignificant, the diagnosis of echinococcosis is particularly difficult. Therefore, uncomplicated echinococcosis is often detected accidentally during preventive examinations.We observed 72 patients with echinococcosis of the lung at the age of 2 to 16 years. Depending on the period of the disease, they were divided into 3 groups: in the initial stage ‒ 3 patients, in the midst of the disease ‒ 36, in the stage of complications ‒ 33 patients.The analysis of the clinical picture showed that specific symptoms are also observed in other (Table 1) respiratory diseases ‒ tuberculosis, abscesses, lung tumors, complications of destructive pneumonia, etc.Domestic and foreign studies contain information about the state of immunity, which allows us to judge the main link of the body's immune defense against various external and internal agents, in particular, during bacterial infestations.As is known, the most informative method of diagnosing echinococcosis of the lungs is radiography, while a typical picture is observed depending on the stage of the disease and the size of the cyst. For example, on a survey radiograph of a pile of cells in two projections with small and medium echinococcal cysts, a rounded darkening with equal borders is detected. The sharpness of the contours and the uniformity of the shadows may be disturbed in the central localization of the echinococcal cyst due to the layering of the shadows of the vascular-bronchial trunk. In large and giant echinococcal cysts, there was a diffuse darkening of the pulmonary field, merging with the shadow of the chest for a significant length or completely filling the entire pulmonary field, and a characteristic contraction of the mediastinal and diaphragm organs (in giant cysts). When an echinococcal cyst broke through into the bronchus, symptoms of a floating membrane and a crescent were revealed, i.e., a crescent-shaped lumen in the upper pole of the cyst. However, these symptoms are not always detected, which creates difficulties in differential diagnosis with a draining lung abscess.When an echinococcal cyst breaks into the pleural cavity, a characteristic radiographic picture appears — the presence of gas and fluid in the pleural cavity; the lung is compressed to the root, the shadow of the mediastinum is shifted to the opposite side. In rare cases, when the chitinous shell enters the pleural cavity, the horizontal fluid level is not even, but wavy.Thus, echinococcosis of the lungs is often difficult to differentiate from an abscess and a lung tumor, as well as from pyopneumothorax, pyothorax. An analysis of 104 X-ray grams of children with suspected lung echinococcosis showed an erroneous interpretation of the results in 6 cases: 4 children at the time of surgery had a lung abscess (and a lung tumor) instead of the expected lung echinococcosis. At the same time, when pyothorax and pyopneumothorax were suspected during surgery, echinococcosis was detected in 2 cases (Table 1).Table 1. Cases of erroneous diagnosis in echinococcosis of the lung in children
 |
| |
|
Therefore, chest X-ray examination is an important and valuable method for diagnosing lung echinococcosis, but it is not without drawbacks: its use does not allow to detect lung echinococcosis with a 100% guarantee. In 5.8% of the observations, diagnostic errors were made.It could be assumed that the most reliable methods of diagnosing echinococcosis, more precisely the presence of echinococcus in the body, are immunological. In the experiment, the sensitivity and specificity of RLA, RNGA, ELISA, TIM, and PCR were tested on a sufficient number of animals of different species. However, the specificity of these reactions did not exceed 82%, with the exception of RSKP (accuracy of indications up to 94.5%), which corresponds to the materials of our publications.In a study of 498 patients with echinococcosis (mostly adults), it was found that the toxicity of RSCP is close to 95.5%. The big disadvantage of RSCP is that it requires live proto-complexes, and this limits its use.Serological studies (RNGA) of the blood of 28 patients with lung echinococcosis showed a positive reaction in most cases (86%). However, even when using RNGA, diagnostic errors were made, for example, this reaction was positive in patients with an abscess and a lung tumor. As already mentioned, uncomplicated echinococcosis of the lung, in contrast to complicated, as a rule, does not present difficulties for diagnosis. Suppurated echinococcus is difficult to differentiate from a lung abscess; echinococcus that has broken into the bronchus ‒ from a draining lung abscess; complicated echinococcosis with a breakthrough in the pleural cavity-from purulent pleurisy, pyopneumothorax. In these cases, ultrasound helps: when detecting echinococcal cysts in other organs, it can be assumed that this is a complicated echinococcosis. In some cases, it is possible to see the chitinous membrane during ultrasound of the lung. With broncho-and thoracoscopy, sometimes a chitinous shell or its fragments are detected, but these manipulations are not safe for the child. Thus, the use of a complex of clinical, instrumental and laboratory methods makes it possible to diagnose echinococcosis of the lung in children with a sufficiently high probability. However, the set of methods does not guarantee against diagnostic errors (see Table 2). Obviously, clinical practice needs to develop new highly sensitive methods for the diagnosis of echinococcosis, which, in combination with the already known ones, will significantly improve the timely detection of lung echinococcosis in children.It is clear that the introduction of the pathogen into the body should lead to the appearance of a specific immune reaction, which must be recorded not only at the humoral, but also at the cellular level. For the serological diagnosis of echinococcosis in adults and children, RNGA is more often used. The postponement of this reaction has proven itself well in clinical practice, but in some cases false-positive results are obtained, which is associated with the presence of cross-reactions with antigens of pathogens of other diseases, as well as with the relatively late appearance of high levels of antibodies in the blood of patients.Our research was aimed at developing an alternative method for detecting the sensitization of patients with echinococcosis to the echinococcal antigen. Studies of domestic and foreign scientists show that cellular immune responses are formed early, since the implementation of humoral immune antibody formation requires intercellular interactions involving cells that already have receptors for this antigen. We assumed that the methods of detecting antigen-binding lymphocytes in the blood of patients, i.e. lymphocytes carrying receptors for a particular antigen may be more sensitive, which will serve as a way to indicate the introduction of various pathogenic agents into the body, such as viruses, bacteria, protozoa and parasites.Over the past few years, we have used the method of determining antigen-binding lymphocytes (ASL) to register bacterial and parasitic agents of the disease, in particular, in osteomyelitis and destructive pneumonia, we were able to determine the type of pathogen.These preliminary data served as the basis for the development of ASL as a diagnostic test for echinococcosis in children.We examined 82 children aged 3 to 16 years, who were divided into groups depending on the localization of echinococcus and the presence of complications. Echinococcosis of the liver was detected in 30 children, lung ‒ in 30, combined echinococcosis in 15 and complicated ‒ in 7 children. The results of the studies showed that up to 12% of ASL circulates in the blood of patients with echinococcosis (on average, the indicator in the group is 5.6 ± 0.2%). The indicated average value in patients was 14 times higher than in healthy patients (0.4 ±0.1%). It was interesting to determine the content of ASL depending on the localization of the pathological process. In the table 2 shows the results of the detection of ASL in the blood of children with echinococcosis of the lungs.Table 2. The content of ASL in the blood of children with echinococcosis of the lungs
 |
| |
|
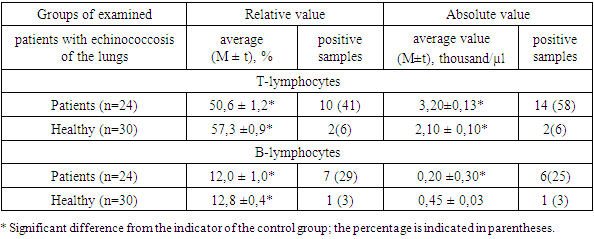
Of the 30 children with echinococcosis of the lungs, ASL was detected in the blood of 26 patients (87%). In combined and complicated echinococcosis, this indicator, according to our data, reaches 100%.These results allowed us to suggest that the determination of ASL in reaction with an echinococcal antigen may have important diagnostic significance in echinococcosis of the liver, lung and other localities of the disease in children. However, to determine the informativeness of the developed method, it was necessary to compare the results obtained with the data of generally accepted tests. For this purpose, in parallel studies with ASL, a serological antigen-specific test — RNGA was performed, which confirmed the advantage of the new test.In domestic and foreign studies, there is information about the state of immunity, which allows us to judge the main link of the body's immune defense against various external and internal agents, in particular, in bacterial infestations, viral infections, tumors, pregnancy, as well as in other diseases and conditions. In these cases, immune disorders were found, which are mainly manifested by secondary immunodeficiency. Immunodeficiency syndrome includes a decrease in the number of T-lymphocytes (immunoregulatory units — T-helpers and T-suppressors), a decrease in the total number of phagocytes. In the B-system of lymphocytes, large changes usually do not occur. However, lymphocytes often appear in the blood of patients that react with their own tissues (autoimmune reactions). Up to a certain point, autoimmune reactions are physiological, i.e. they are necessary to maintain the functional activity of a particular organ, but when crossing a certain border, they can play a pathogenetic role. Based on this, it becomes clear that the assessment of the immune status can carry important information not only about the state of the protective link, but also about the development of possible immunopathological reactions directed against one's own body. According to WHO recommendations, the assessment of the immune status should be carried out on the most important links: the state of the T-and B-systems of lymphocytes, the phagocytic system of leukocytes, as well as immunoglobulins. Our experience shows that in order to obtain additional and important information about the state of the human immune system, data on specific immune responses are needed. Usually, these methods determine the content of antibodies directed against the pathogen of the disease. At the same time, it should be taken into account that the appearance of antibodies is preceded by cellular immune reactions. In particular, the development of the humoral immune response involves several types of cells that carry specific receptors for this antigen — such as antigen-specific T-helpers, T-suppressors, T-lymphocytes and other lymphocytes. All these cells carry receptors on the surface that are designed to interact with this antigen. It can be assumed that in the body of patients with some infective or parasitic disease, ASL will first appear and only then there will be an accumulation of antibodies to the diagnostic titer and higher. In clinical studies, the method of T-rosette formation has been recognized, which allows us to determine with sufficient accuracy in vitro the content of T-lymphocytes in the blood. T-lymphocytes were determined in 97 patients with echinococcosis aged from 1 to 16 years (with liver echinococcosis-34 children, with lung echinococcosis — 24, with combined and complicated echinococcosis-22 and 17, respectively). Complications include cyst rupture and suppuration. This course of the disease was detected in 17 children. The control group consisted of 30 practically healthy children aged 3 to 15 years. It was found that their blood contained an average of 57.3 ± 0.9% T-lymphocytes and 12 ± 1% B-lymphocytes (Table 3). In children with echinococcosis, the number of T-lymphocytes in the blood was statistically significantly increased.Table 3. The content of T-and B-lymphocytes in the blood of children with echinococcosis of the lungs
 |
| |
|
It is known that T-lymphocytes mainly consist of T-cells and T-suppressors. It was important to determine which immunoregulatory subpopulations of T-lymphocytes are most affected by lung and liver echinococcosis. The content of T-helper cells in the blood of healthy children is on average 43.9 ± 0.9% (from 39 to 51%). In children with echinococcal lung disease, the number of T-helpers in the blood was statistically significantly increased.The integral indicator of the B-system of lymphocytes is the content of immunoglobulins in the blood. As already mentioned, the absolute content of B-lymphocytes was low. Nevertheless, there was an increased content of IgA and IgM in the bloodstream. So, if in practically healthy children the blood contained 0.8 ± 0.03 g/l of IgA, then in patients their level was increased by 2.3 times (on average 2.3 ± 0.03 g / l).The level of circulating immune complexes (CIC) in the group of patients with echinococcosis was 1.6 times higher than normal.Thus, an increase in humoral immunity was noted. One of the most important indicators of organ resistance (factors of non-specific protection) is the phagocytic activity of neutrophils, estimated by two indicators: the relative content of cells capable of phagocytosis and their absolute content in 1 ml of blood. Studies have shown that in practically healthy children, the blood contains an average of 55.8±0.6% of phagocytic neutrophil cells. In patients with echinococcosis, this indicator was reduced by 1.4 times.By the nature and depth of the violation of the immune system, echinococcosis of the lungs in children can be interpreted as a secondary immunodeficiency.When comparing the clinical manifestations of the disease, the following was noted: in patients receiving immunocorrective treatment, the postoperative period was usually calm.
4. Discussion of the Results and Conclusions
In the long-term period after the operation, patients were examined at the control time (1, 3, 6 months, 1, 1.5—2, 3 years), a month later, patients were examined in the polyclinic by interviewing, examining, and performing radioscopy and radiography of the chest in two projections. After 3 months or more, the patients were admitted to the hospital for 3-5 days.When studying the long-term results, we took into account:* presence or absence of complaints;* the presence or absence of a relapse of the disease;• chest X-ray results in two projections;• ability to work;* data on serological reactions;* results of radionuclide studies.Criteria for evaluating the effectiveness of treatment:1) detection - complete recovery from the main disease, complete restoration of working capacity, absence of any complaints, during X-ray examination-absence or insignificant area of pneumofibrosis in the lung; in a separate period-negative serological reactions (RLA, RNGA, RDDH); after 1.5-2 years - restoration of ventilation in the operated lung (for example, a slight perfusion effect in the area of the former localization of the parasitic cyst);2) a good result - complete recovery from the underlying disease, restoration of working capacity, absence of any complaints; in X-ray examination-a site of more severe pneumofibrosis compared to that of the group identified by radionuclide methods of research;3) a satisfactory result — recovery from the main disease in the presence of complications not related to the use of a new technique (suppuration of the wound, etc.), the presence of any complaints, the site of gross pneumofibrosis, ventilation and perfusion defects;4) unsatisfactory result - dry periodic cough, some disability, X-ray examination-identification of the failure of the proposed method in the form of a false pneumocyst, dry cavity or exudate at the site of the bed. Defect of perfusion and ventilation, identical to the preoperative one. Reduced work capacity.
References
| [1] | Azizzoda Z. A., Kurbonov K. M., Ruziboyzoda K. R., Rasulov N. A., Ali-Zade S. G. (2019). The importance of laboratory parameters in the diagnosis of complicated liver echinococcosis. Avicenna Bulletin, vol. 21, no. 4, pp. 655-660. |
| [2] | Akimniyazova B. B., Kausova G. K., Eshmuratov T. Sh., Eleusizov A.M., Enin E. A. (2019). On the difficulties of diagnosing combined complicated multiple echinococcosis of the lungs. Medicine (Almaty). No. 4 (202). pp. 69-74. |
| [3] | Vakhidova A.M., Muradova E. V., Nurimov P. (2020). To study the pathogenesis of echinococcosis. Avicenna. No. 71. pp. 27-32. |
| [4] | Vakhidova A.M., Khudayarova G. N., Boltaev K. S. (2020). Echinococcosis of the lungs, complicated by pecilomycosis. Monograph, Global Publishing House. |
| [5] | Vakhidova A.M., Khudayarova G. N., Boltaev K. S. (2019). Study of the microflora of the contents of echinococcal bladders by morphological ratio and determination of its sensitivity to antibiotics. Academy. 7 (58), 8-10. |
| [6] | O. Yu., Ataeva F. M. (2019). Informative value of magnetic resonance imaging in the recognition of hydatidous echinococcosis of the liver. Bulletin of medical Internet conferences. Vol. 9. No. 8. p. 327. |
| [7] | Ermakova L. A., Golovchenko N. V., Tverdokhlebova T. N., Bolatchiev K. Kh., Shishkanova L. V. (2017). The relevance of seroepidemiological studies in hydatidous echinococcosis. Theory and practice of combating parasitic diseases. No. 18. p. 15. |
| [8] | Kastarnova E. S., Orobets V. A. (2017). Exosomal dosage form as a way to provide radical chemotherapy for echinococcosis. Theory and practice of combating parasitic diseases. No. 18. pp. 194-196. |
| [9] | Kenzhetai Zh., Allabergenova A., Aitzhanova T., Romashev K. M., Rozhaev B. G., Dosanov K. Sh. (2019). Amino acid composition of slaughter products of healthy and sick animals with echinococcosis in a comparative aspect. Kazakhstan Science News, 2 (140), 139-146. |
| [10] | Krasnoselsky N. V., Krutko E. N., Shulga N. V., Shulga E. V. (2018). Correction of the enzymatic state and lipid peroxidation in cancer patients with multi-organ surgical interventions. Emergency Medicine, 5 (92), 135-140. |
| [11] | Minaev S. V., Razin M. P., Grigorova A. N., Gerasimenko I. N., Sirak A. G., Orujev M. T., Timofeev S. I. (2019). Morphological picture of liver echinococcosis, depending on the type of parasitic cyst. Vyatka Medical Bulletin. No. 4 (64). pp. 4-8. |
| [12] | Mirkhodzhaev I. A. (2020). The role of cytokines in the development and course of liver echinococcus. Biology and integrative medicine, 2 (42), 62-74. |
| [13] | Pisanova L. A., Berezhko V. K., Sivkova T. N. (2015). The effectiveness of the point enzyme immunoassay (dot-elisa) in the diagnosis of trichinosis and echinococcosis. Vyatka Medical Bulletin. No. 4 (48). pp. 18-21. |
| [14] | Nakhodkin S. S., Pshennikova V. G., Dyachkovskaya P. S., Nikanorova A. A., Teryutin F. M., Barashkov N. A., Melnichuk O. A., Manyaval Zh. F., Fedorova S. A. (2019). The prevalence of enzyme immunoassay markers of echinococcosis, trichinosis, and toxocarosis in the rural population of central Yakutia. Bulletin of the North-Eastern Federal University named after M. K. Ammosov. No. 4 (72). pp. 24-33. |
| [15] | Raimkulov K. M., Usubalieva Zh. M., Toigombayeva V. S., Kuttubaev O. T. (2018). Clinical and laboratory examination to detect echinococcosis infestation in residents of the Alai district of the Osh region. Proceedings of the Academy of Sciences of the Republic of Tajikistan. Department of Biological and Medical Sciences. No. 2 (201). pp. 74-78. |
| [16] | Samotrueva M. A., Yasenyavskaya A. L., Murtalieva V. Kh., Shpagina M. Yu. (2020). Effect of ACTH (6-9)-pro-gly-pro peptide on the intensity of lipid peroxidation in immunocompetent organs under conditions of "social" stress. In the collection: Fundamental and Applied Science: New Challenges and Breakthroughs. collection of articles of the International Scientific and Practical Conference, 276-279. |
| [17] | Tkhakakhova A.A., Andreyanov O. N., Timofeeva O. G. (2017). Sensitivity of protoscolexes of echinococcus multilocularis to antibiotics. Theory and practice of control of parasitic diseases, 18 (3), 486-488. |
| [18] | Udilov V.S., Sabitov A. U. (2018). Efficacy and safety of long-term therapy courses in human echinococcosis. Population health and habitat. No. 12 (309). pp. 53-56. |
| [19] | Khatsko V.V., Vakulenko I. P., Shatalov A.D., Fominov V. M., Voityuk V. N. (2018).Comprehensive diagnosis of hydatidous echinococcosis of the liver. Bulletin of Hygiene and Epidemiology, vol. 22, no. 1, pp. 60-63. |
| [20] | Shishkina L.N., Menshov V. A., Shubina O. G., Idrisova E. V., Sluyanova N. V., Samoylenko I. I. (2007). The role of parameters of the system of regulation of lipid peroxidation in the toxigenization of the environment by conditionally pathogenic microflora. Advances in Modern Biology, vol. 127, 1 (1), 50-57. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML