-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Virology and Molecular Biology
p-ISSN: 2163-2219 e-ISSN: 2163-2227
2020; 9(1): 1-5
doi:10.5923/j.ijvmb.20200901.01

Prevalence of HIV among Patients Patronizing a Private Laboratory in Port Harcourt Metropolis, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOkonko Iheanyi Omezuruike1, Nwoke Chibuzor Mabel1, Cookey Tochi Ifeoma1, Stanley Catherine Nonyelum2
1Virus Research Unit, Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Pharmaceutical Microbiology & Biotechnology, University of Port Harcourt, Port Harcourt, Nigeria
Correspondence to: Okonko Iheanyi Omezuruike, Virus Research Unit, Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study was carried out to detect the presence of HIV-1/2 antibodies among patients patronizing Healthwise laboratories in Port Harcourt, Nigeria. Two hundred subjects (74 males and 126 females) were used in this study. Samples of blood were collected randomly from Healthwise Laboratories Limited, Port-Harcourt, Nigeria. The samples were collected and processed using standard laboratories procedures. Determine® HIV-1/2 Test cards, Global® HIV-1/2 kits and fourth-generation ELISA-based kits were used in a stepwise order for the detection of HIV-1 and HIV-2 in the blood. The overall prevalence rate of HIV-1/2 was 6.5%. Higher prevalence of HIV was found in the age group 10 years and above (6.6%) and in males (8.1%). Two risk factors (age and gender) relevant to the transmission of HIV were considered. None of the two risk factors seemed to be significantly associated (P > 0.05) with the prevalence of HIV-1/2 antibodies amongst the study population. The present study however, long-established the occurrence of HIV-1 and 2 antibodies in Port Harcourt, Nigeria. HIV can affect all age groups, both males and females. This calls for more concerted HIV prevention and awareness efforts in the state. Intensive health education campaigns and training on HIV prevention and control are advocated.
Keywords: Antibody, Patients, HIV, Seropositivity, Risk factors
Cite this paper: Okonko Iheanyi Omezuruike, Nwoke Chibuzor Mabel, Cookey Tochi Ifeoma, Stanley Catherine Nonyelum, Prevalence of HIV among Patients Patronizing a Private Laboratory in Port Harcourt Metropolis, Nigeria, International Journal of Virology and Molecular Biology, Vol. 9 No. 1, 2020, pp. 1-5. doi: 10.5923/j.ijvmb.20200901.01.
1. Introduction
- Human Immunodeficiency Virus (HIV) is still a major public health challenge, especially in resource-limited settings (Oleribe et al., 2018). Since 1981 when HIV was first identified and characterized, HIV has remained an infection of public health importance (UNAIDS, 2004, 2017; Oleribe et al., 2018). HIV infection has continued to spread in the last 39 years and has had a great impact on all sectors such as health, welfare, employment and criminal justice; thus, touching all socio-ethnic groups all over the world (Awofala and Ogundele, 2018). Nigeria as a country grasps the overwhelming effects of HIV/AIDS on its populace, social, economic, and health progress fairly recently (Awofala and Ogundele, 2018). To date, HIV has taken more than 35 million lives with over a million people dying from HIV-related causes globally (UNAIDS, 2016a,b; Oleribe et al., 2018). Since the beginning of the epidemic, 75 million people have been infected with the HIV and about 35 million people have died globally with 37.9 million individuals living with HIV at the end of 2018 (WHO, 2019). Although the burden of the epidemic continues to vary considerably between countries and regions, an estimated 0.8% of adults aged 15–49 years worldwide lived with the virus (WHO, 2019). However, Africa remains most severely affected by HIV, with closely 1 in every 25 adults (3.9%) living with the virus and that accounts for more than two-thirds of the individuals living with the virus globally (WHO, 2019). Key vulnerable populations at a higher risk of acquiring HIV and thus developing AIDS continued to be pregnant women, infants, prison inmates, injecting drug users (IDU) and men who have sex with men (MSM) (Oleribe et al., 2018). In Nigeria, the national HIV prevalence among adults aged 15–49 years stood at 1.4% with 1.9 million people living with HIV in Nigeria as recently released by the Federal Government of Nigeria on March 14, 2019 (UNAIDS/NACA, 2019). Previous estimates of national HIV prevalence had indicated different rates, following sentinel surveys conducted in Nigeria indicated 1.8% in 1991, 3.8% in 1993, 4.5% in 1996, 5.4% in 1999 and a peak (5.8%) in 2001. However, somewhat decline in HIV trends were noted after 2001, preliminary with 5.0% in 2003, 4.4% in 2005, 4.6% in 2008, 4.1% in 2010, 3.4% in 2013, 3.0% in 2014, 2.9% in 2016 and 1.4% in 2018 (FMoH, 2013, NACA, 2017; AVERT, 2018; UNAIDS/NACA, 2019; NAIIS, 2019). Clearly, the trends of HIV prevalence in the country is comparatively stable and this positive change in HIV trend in Nigeria is largely credited to an efficient operative reporting and intervention system in place (UNAIDS, 2014b; Awofala and Ogundele, 2018).Furthermore, individuals practising low-risk sexual activities are the driving force in the trends of the HIV epidemic in Nigeria. Conversely, the high-risk groups (MSM, female sex workers, and IDU) contribute significantly to new HIV infections in the country (Awofala and Ogundele, 2018). Thus, the reported 1.4% adult HIV prevalence in Nigeria is comparatively low, hitherto Nigeria is a huge country where HIV infection had remained a problem that requires a regular systematic and extremely tailored interventions (Awofala and Ogundele, 2018). While national HIV prevalence seems stabilizing in the country, to reason that the trend cannot reverse in an upwards manner will amount to an underestimation and equally an understatement (Awofala and Ogundele, 2018). Indeed, ‘the prevalence of HIV disease will upsurge, while the future occurrence of new HIV infections is uncertain’ (Nikolopoulos et al., 2008; Awofala and Ogundele, 2018). Thus, the present study was designed to determine the seroprevalence of HIV infection among people in Port Harcourt metropolis, Nigeria.
2. Materials and Methods
- Study AreaThe present study was done among people living in Port Harcourt metropolis, Nigeria. Port Harcourt is the capital of Rivers State, Nigeria which lies along the Bonny River, and it is located in the Niger Delta. According to the 2006 Nigerian census Port Harcourt has a population of 1,382,592. Its heaviest rainfall happens throughout September with an average of 370mm of rain. December on average is the driest month of the year, with an average rainfall of 20mm. Temperatures all over the year are comparatively constant, showing slight variation through the sequence of the year. Average temperatures are typically between 25°C -28°C in the city (Ogbonna, 2007; Mbakwem-Aniebo et al., 2012).Study PopulationThere was a cross-sectional seroanalysis to determine the seroprevalence of HIV infection among people in Port Harcourt metropolis. A total number of two hundred (200) patients of different ages and socioeconomic status were tested. There were 74 males and 126 females in this study. Serological Analysis The serological analysis of HIV infection was established by standard ELISA-based kits (manufactured by Dia.Pro Diagnostic Bioprobes Srl, Italy). Alongside the DETERMINE(R) HIV-1/2 Test cards (manufactured by Abbott Laboratories, Japan) and Global® HIV-1/2 Kit (manufactured by Global Diagnostics, the USA were used. All test and interpretations of test results were carried out according to the manufacturer’s specifications.
3. Result
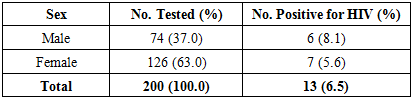
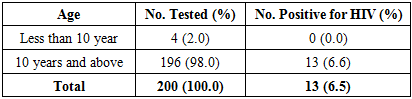
- Patients Characteristics A total number of two hundred (200) people were used in this study (Table 1 and 2). There were 74 (37.0%) males and 126 (63.0%) females (Table 1). Age ranges from 4 years to 50 years. One hundred and ninety-six of them (98.0%) were in age groups 10 years and above while 4 (2.0%) belong to less than 10 years of age (Table 2). The overall prevalence of HIVAn overall HIV prevalence of (6.5%, n = 13) was observed in this study (Table 1 and 2). Prevalence of HIV in relation to sex Higher prevalence of HIV was recorded in males (8.1%, n=6) than females (5.6%, n = 7) as shown (Table 1).
|
|
4. Discussion
- This study investigated the prevalence of HIV-1 and HIV-2 antibodies among people in Port Harcourt metropolis, Nigeria. This was necessitated by the fact that the South-South geopolitical region of Nigeria is one of the areas with the highest HIV prevalence in the country (NAIIS, 2019). According to the new data from the Nigeria National HIV/AIDS Indicator and Impact Survey (NAIIS, 2019) which differentiated HIV prevalence in relation to States, the present HIV trend indicated an epidemic that has a greater impact in certain regions and states of the country. This NAIIS (2019) puts the South-South region of the country as having the highest HIV prevalence (3.1%). It also indicated that two South-South States are among the three States with the highest prevalence of HIV in Nigeria (NAISS, 2019), which include Akwa Ibom State on top with 5.5% of its inhabitants living with HIV and Rivers State as the third with 3.8% prevalence. In this study, a total of 200 subjects were used and the majority were females (63.0%) and age group 10 years and above (98.0%). This collaborated with previous studies on HIV, Awofala and Ogundele (2018) showed that females were more prone to acquire HIV and less probably to be enrolled in treatment. In the same report, although fewer men were tested, a higher proportion of males who were HIV positive actually enrolled into treatment than their female counterparts (Awofala and Ogundele (2018).Of the 200 subjects residing in Port Harcourt metropolis tested, 13 representing 6.5% were positive for HIV-1 and HIV-2 antibodies. As the world arrives the fourth decade of the HIV/AIDS epidemic, the indication of its impact is undeniable, robbing countries of both human and natural resources. The observed 6.5% is higher than what was observed elsewhere in Nigeria and abroad. In the United State of America, the prevalence of HIV among male and female premarital couples was found to be 0.0 to 1.1% and 0.0 to 0.4% respectively (Peterson and Waite 1990; Mbakwem et al., 2012). It was also more than the prevalence of HIV of 0.2% reported by Gayle (1990) among University Students in the USA. In addition, the 6.5% prevalence obtained in this present study is more than the 3.8% reported for Rivers State, Nigeria in the last sentinel survey (NAIIS, 2019). However, it is lower than the 31.0% prevalence reported in a tertiary health institution in the Niger Delta region of Nigeria (Alikor and Erhabor, 2005).According to our study, it was discovered that the males had a higher prevalence of HIV (8.1%) than the female subjects (5.6%) and this association of HIV prevalence with the sex of the subjects was found to be significant. A higher prevalence of HIV/AIDS among males than in females have been documented in a few studies (Mbakwem et al.,2012), which is in line with what was reported in this study. However, this finding deviated from what was reported in the last sentinel study in Nigeria. Nigeria National HIV/AIDS Indicator and Impact Survey (NAIIS, 2019) puts HIV prevalence to be higher in females (1.9%) than males (0.9%). In addition, Laah and Ayiwulu (2010) observed that females had a higher seroprevalence rate of HIV than in males in Nasarawa State, Nigeria.While the national prevalence rate of HIV in Nigeria in 2019 is 1.4% among the adult populace aged 15 – 49 years, women in the same age group are more than twice as likely (1.9%) to be living with the HIV when compared to the men (0.9%). This difference is greater among the younger adults, with the females aged 20 – 24 years more than thrice as likely to be living with the virus when compared to the men in the same age group (NACA/UNAIDS, 2019). Higher prevalence of HIV reported in males in this study supports the claims that high-risk sexual behaviour is much more common among young men (Bremner et al., 2009; Laah and Ayiwulu, 2010). However, data from previous studies in Nigeria and elsewhere have indicated that females are disproportionately affected by HIV. In many countries like in Nigeria, young women are about two to five times more probable to be infected than young men (Laah, 2003; Mamman, 2003, 2006; Panchabadeswaran et al., 2006; Rosen et al., 2008; Bremner et al., 2009; National Population Commission and ICF Macro, 2009; Hedden et al., 2009; Adebayo et al., 2009; Laah and Ayiwulu, 2010). This contrasts with a few previous studies which documented a higher prevalence of HIV/AIDS among males than females (Celikbas et al., 2008; Avert, 2010), which are in consonance with the findings of this study. Two categories of age structure were adopted by the study. These are adults and adolescent ranging from 10 years and above and children ranging below 10 years old. The sex-specific HIV prevalence shows that HIV antibody was recorded only in age groups 10 years and above (6.6%, n=13) while age groups less than 10 years had a zero prevalence. It also showed that children below 10 years tested negative to compare to those ranging from 10 years and above. This agrees with the National HIV prevalence pattern in Nigeria (NAIIS, 2019). According to the new data, HIV prevalence among children aged 0 – 14 years is 0.2%. In recent years, new strategies have been adopted to stop new HIV infections among children (NACA/UNAIDS, 2019). These findings were consistent with other findings in Nigeria where most of the people infected with the HIV were young people within the productive and reproductive age groups (Laah, 2003; NYSC/UNICEF, 2007; National Population Commission and ICF Macro, 2009; Laah and Ayiwulu, 2010).This difference in parameters calls for further investigation to identify the factors responsible for this (Awofala and Ogundele, 2018). In fact, the key factor contributing to the continuous spread of HIV/AIDS could be attributed to pre-marital and extra-marital sexual contact which were very common in Port Harcourt, Nigeria. HIV prevalence in Port Harcourt could be fueled by low levels of male and female condom use, high rates of casual and transactional unprotected sex among young people, poverty, low literacy levels, cultural and religious factors, as well as stigma and discrimination. However, HIV testing can serve as a link for offering early treatment and encouraging behavioural change among people already living with HIV or at risk of getting infected. One of the drawbacks of this study is its small sample size however, the findings are valid, informative, may reflect the true prevalence of the actual population of people in Port Harcourt metropolis, Nigeria. From this study, it could be inferred that HIV is prevalent in Port Harcourt metropolis at a high rate.
5. Conclusions
- The high prevalence of HIV in Port Harcourt, Nigeria, has been further reinforced in this study. This calls for more concerted HIV prevention and awareness efforts in the state. The fact remains that when total abstinence or safer sex especially sexual fidelity among the adolescent and adults and accessibility of male and female condoms are promoted, people will be protected against the infection.