-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Virology and Molecular Biology
p-ISSN: 2163-2219 e-ISSN: 2163-2227
2015; 4(2): 19-22
doi:10.5923/j.ijvmb.20150402.01
Sero-Epidemiology of Hepatitis B and C Virus in Rural Population of Tehsil Samundri, District Faisalabad, Pakistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAmmara Khalid1, Muhammad Zahid1, Zeeshan Aslam1, Muhammad Bilal1, Ali Haider2
1Institute of Microbiology, Faculty of Veterinary Sciences, University of Agriculture, Faisalabad, Punjab, Pakistan
2Department of Clinical Medicine and Surgery, University of Veterinary and Animal Sciences, Lahore, Punjab, Pakistan
Correspondence to: Muhammad Zahid, Institute of Microbiology, Faculty of Veterinary Sciences, University of Agriculture, Faisalabad, Punjab, Pakistan.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
In last few decades, infection of Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) has appeared as one of the major causes of acute and chronic liver diseases especially in Pakistan. The objective of the present study was to estimate the prevalence of hepatitis B and hepatitis C in rural population of Tehsil Samundri, District Faisalabad, Pakistan. This study was done on the basis of gender and area. A total of 1380 serum samples (138 each) were collected from both adult males and females of 10 randomly selected villages in different Union councils of Faisalabad. Primary screening was done by using chromatographic strip method. Positive cases for hepatitis B and hepatitis C were analyzed by a sensitive viral detection technique named, ELISA (G.D Germany).The results of the present study showed that 6.15% (n=85) candidates were found reactive with hepatitis B surface antigen and 22.68% (n=313) participants were found positive for anti HCV antibodies. In our study, area wise values of HBsAg and HCV fell between 2.1% - 10.86 and 20.2% - 26.8% respectively. Male with (6.21%) and females with (6.08%) values showed that there was non-significant difference (P>0.05) in HBV prevalence. Results were also non significant on the basis of HCV antibodies found in males (21.95%) and females (23.68%). Different corrective measures over and above awareness programs are the need of people especially belongs to rural areas.
Keywords: HBV, HCV, Village, Faisalabad, Pakistan
Cite this paper: Ammara Khalid, Muhammad Zahid, Zeeshan Aslam, Muhammad Bilal, Ali Haider, Sero-Epidemiology of Hepatitis B and C Virus in Rural Population of Tehsil Samundri, District Faisalabad, Pakistan, International Journal of Virology and Molecular Biology, Vol. 4 No. 2, 2015, pp. 19-22. doi: 10.5923/j.ijvmb.20150402.01.
1. Introduction
- Hepatitis is a highly contagious disease which is caused by viruses and some other infectious agents, able to infect the hepatocytes. Infection of hepatocytes leads to inflammation of the liver, chronic liver disease and jaundice. The major factors responsible for transfer of these viruses are blood and its products, intra-familial transmission and sexual acquaintance. According to an estimate the amount of infected persons by these viruses includes 350 million people with chronic HBV and 170 million people with chronic HCV infection around the globe [1].High prevalence rate of hepatitis B infection that is more than 8% is found in Africa, Asia and Alaskan populations. Moderate prevalence of HBV infection i.e. 2-7% exists in south east and central Europe region. While the very low prevalence of hepatitis B infection that is < 2% is present in western and Eastern Europe, America and Australia [2].Pakistan is also one of those countries which are badly affected with hepatitis B and hepatitis C infection. As compared to other Asian countries like India, Nepal, Myanmar, Iran and Afghanistan, the incidence of hepatitis C is much greater in Pakistan [3].HCV infection is mainly responsible for 60-70% of all liver malignancy cases and is the commonest reason of liver transplant all over the world. Liver cirrhosis is the 18th frequent cause of mortality [4].The objective of this study was to establish the sero-prevalence of Hepatitis B and Hepatitis C infection in rural population of Tehsil Samundri, District Faisalabad, Pakistan. So that proper awareness can be raised in the people of selected area.
2. Materials and Methods
- An epidemiological study was conducted to detect the sero-prevalence of hepatitis B and hepatitis C among apparently healthy males and females of the rural areas of Tehsil Samundri, District Faisalabad. This study was conducted from 2011 to 2012. For these purpose 10 union councils (UC) were randomly selected and from each UC one village was randomly chosen for sampling procedure. An informed consent was taken from studied population before sampling.The approximate sample size required to estimate the prevalence of HBV and HCV infection was determined through simple random sampling formula, using 95% confidence interval Thursfield (2007) with expected prevalence of 10%, Total 1380 samples were analyzed for hepatitis B and hepatitis C infection among the rural inhabitants of District Faisalabad [5].The relevant formula for a 95% confidence interval is:
 Where: n=required sample size, P=expected prevalence, D=desired absolute precisionAccording to above stated formula sample size of this research was equal to 1380.The HBsAg kit (DS-EIA-HBsAg, DSI G.D Germany) was used for detection of HBsAg in serum and Hepatitis C kit (EIA-ANTI-HCV G.D Germany) was used for detection of IgG and IgM antibodies that were present in human blood serum against viral hepatitis C.Blood was collected in vacutainer tubes containing no anticoagulant. Collected blood was approximately 2½ times more the volume needed for use e.g. 5 ml blood for 2 ml serum. Centrifuged for 15 min according to manufacturer’s recommended speed (usually 1000-2000 RCF). Serum was stored at -20°C after transfer it in labelled cryovial tubes.Primary screening was done by using chromatographic strip method, allowed to obtain the incidence of hepatitis B and C virus infection in the selected rural population. Positive cases for hepatitis B and hepatitis C were analyzed through a technique named; ELISA. The data thus obtained was tabulated and analyzed by Chi-square method.
Where: n=required sample size, P=expected prevalence, D=desired absolute precisionAccording to above stated formula sample size of this research was equal to 1380.The HBsAg kit (DS-EIA-HBsAg, DSI G.D Germany) was used for detection of HBsAg in serum and Hepatitis C kit (EIA-ANTI-HCV G.D Germany) was used for detection of IgG and IgM antibodies that were present in human blood serum against viral hepatitis C.Blood was collected in vacutainer tubes containing no anticoagulant. Collected blood was approximately 2½ times more the volume needed for use e.g. 5 ml blood for 2 ml serum. Centrifuged for 15 min according to manufacturer’s recommended speed (usually 1000-2000 RCF). Serum was stored at -20°C after transfer it in labelled cryovial tubes.Primary screening was done by using chromatographic strip method, allowed to obtain the incidence of hepatitis B and C virus infection in the selected rural population. Positive cases for hepatitis B and hepatitis C were analyzed through a technique named; ELISA. The data thus obtained was tabulated and analyzed by Chi-square method.3. Results
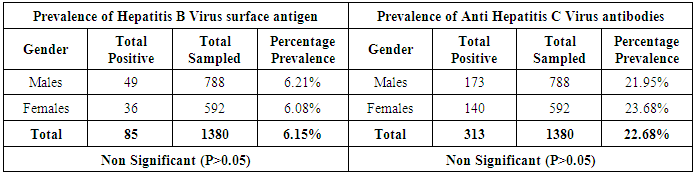
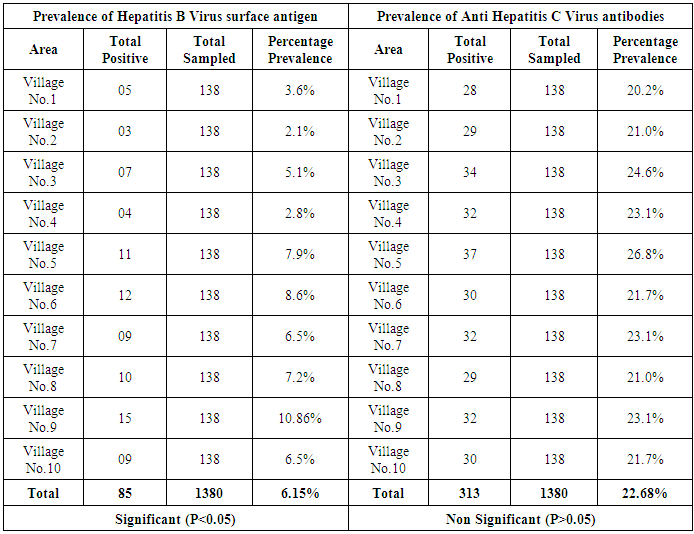
- The results of present study showed that out of 1380 samples, 85(6.15%) cases were found positive for HBsAg and 313(22.6%) for anti-HCV. Graphical representation of HBV and HCV infection prevalence in 10 villages of different union councils is given bellow.On the basis of gender non significant (P>0.05) difference in prevalence of HBV was present among males (6.21%) and females (6.08%), while similar non significant results were obtained in case of HCV antibodies that were 21.95% in males and 23.68% in females (Table 1).
|
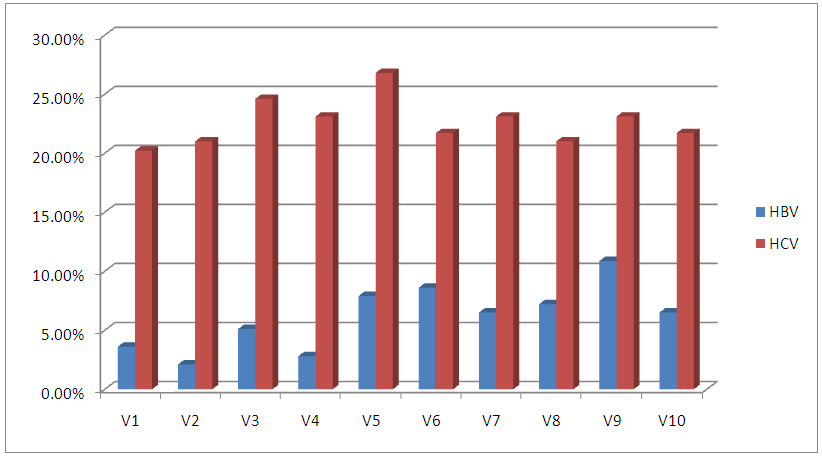 | Figure 1. Comparison in prevalence of HBV and HCV in Rural Population of Faisalabad |
|
4. Discussion
- Hepatitis caused by HBV and HCV is the main reason of liver diseases and ultimately death in acute cases. According to estimate approximately one third populations around the globe have been infected with HBV [6]. About 180 million inhabitants are infected with hepatitis C infection in whole the world .The prevalence of hepatitis C infection in Egypt has been determined to be highest among all countries [7].In our study, area wise values of HBsAg and HCV fell between 2.1% - 10.8% and 20.2% - 26.8% respectively. Different reasons were involved in the difference of results. Socioeconomic status i.e education and availability of basic facilities were prominent factors, responsible for difference in results. Prevalence rate of HBsAg and HCV was less among people having good socioeconomic status whereas on the other hand prevalence rate was high among people with low socioeconomic status.Zuure et al., (2010) documented that basic difference in the percentage of infected persons is the difference in their education [8]. Findings by Ahmad et al., (2007) in case of prevalence of hepatitis C infection is concordant to the present findings where the author has reported 20.6% prevalence of hepatitis C infection in general population [9]. Bhatti et al., (2007) results about 1.1% prevalence of HBV and 2.1% of HCV in students, belongs to higher socioeconomic status and was not in agreement to our present study [10]. The results of present study showed that out of 1380 samples, 85 (6.15%) cases were found positive for HBsAg and 313(22.6%) for anti-HCV. This study has been found in accordance with many previous studies, where different percentages of HBsAg and anti-HCV prevalence were reported. According to Moattar et al., (2002) and Ahmad (2006) 0.99%, 1.1%, 3.1%, 4%, 4.3%, 6.5%, 9.97%, 10%, for HBsAg prevalence and 2.2%, 3.3%,4%, 4.8%, 11.3%, 16% and 16.3%, for Anti-HCV prevalence were reported in past literature [11, 12]. Nafees et al., (2007) reported 17.7% prevalence of hepatitis C infection in District Faisalabad that coinciding with our present study which reports prevalence of HCV 22.6% [13].Gender base study was performed which reported a non-significant difference in prevalence of both HBV and HCV as mentioned in results and our results were also favoured by the findings of Daudpota and soomro (2008) who also found a non-significant difference in prevalence of hepatocytic infection in male and female [14]. Hence our findings found contradict to ones reported by Ali et al., (2009), whose findings suggest a higher ratio of prevalence among male members of population as compared to female members [15].Main threat which arising for health care professionals and society is the presence of asymptomatic infected persons among common population [16].
5. Conclusions
- Prevalence of HBsAg is 6.1% and anti Hepatitis C antibody is 22.6% in the studied rural population of District Faisalabad. These are possibly candidates for chronic liver disease as well as potential sources of spread of infections both horizontally and vertically. It is imperative to create mass awareness programs in the rural community on different aspects of these deadly infections. Mass screening program should be undertaken to define the infected population properly so that they may be managed as per guidelines to get results in lower infection rate.