-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Tumor Therapy
p-ISSN: 2163-2189 e-ISSN: 2163-2197
2014; 3(1): 17-19
doi:10.5923/j.ijtt.20140301.03
Aggressive Anal Squamous Cell Carcinoma with Vertebral and Cardiac Metastasis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAvantika Chenna MD, Punita Kaveti MD, Ujwala Gunnal MD, Kelly Schrapp MD, Chinedu Ivonye MD
Department of Internal Medicine, Morehouse School of Medicine, Atlanta, GA 30310-1495
Correspondence to: Avantika Chenna MD, Department of Internal Medicine, Morehouse School of Medicine, Atlanta, GA 30310-1495.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Anal squamous cell carcinoma (SCC) is a rare tumor of gastrointestinal tract. Incidence of anal SCC in the general population has increased lately due to changes in sexual practices, incidence of Human immunodeficiency virus (HIV) and Human papilloma virus (HPV). It is a loco-regional disease but can have distant metastasis if not treated early. We present a case of a 35 year old man with Acquired immunodeficiency syndrome (AIDS) who had a fatal outcome from aggressive anal squamous cell carcinoma which widely metastasized to lungs, liver, spine and heart. Anal SCC can be aggressive in HIV and HPV coinfected patients. We need research studies to see if early anal cancer screening is beneficial in these patients.
Keywords: Anal squamous cell carcinoma, HIV, HPV
Cite this paper: Avantika Chenna MD, Punita Kaveti MD, Ujwala Gunnal MD, Kelly Schrapp MD, Chinedu Ivonye MD, Aggressive Anal Squamous Cell Carcinoma with Vertebral and Cardiac Metastasis, International Journal of Tumor Therapy, Vol. 3 No. 1, 2014, pp. 17-19. doi: 10.5923/j.ijtt.20140301.03.
1. Introduction
- Anal cell cancer (ACC) accounts for about 1.5% of all digestive system cancers in the United States with Squamous Cell Carcinoma (SCC) being the most common histological type (1). Over 90% of the patients present with loco-regional disease and less than 20% of the cases will have distant metastasis (2). Most common sites of metastasis are to the liver and lungs (3-4). As per our literature search, only 1 case of vertebral metastasis has been reported so far and there has been no reported case of cardiac metastasis. We discuss a case of 35 year old man with AIDS who was diagnosed with aggressive anal SCC who had vertebral and cardiac metastasis.
2. Case Report
- A 35 year old African American man with 10 year old history of genital warts and recently diagnosed with AIDS and anal SCC presented with four days history of back pain and bilateral lower extremity weakness with decreased sensation. He was diagnosed with anal SCC 8 months prior to presentation and had loop colostomy, anal mass (Figure 1) resection including shaft of penis and had interrupted 5 Fluorouracil and Mitomycin based chemoradiation and radiation treatments. He was on antiretrovirals with undetected viral load. He was homosexual, nonsmoker and nonalcoholic with no history of illicit drug use.
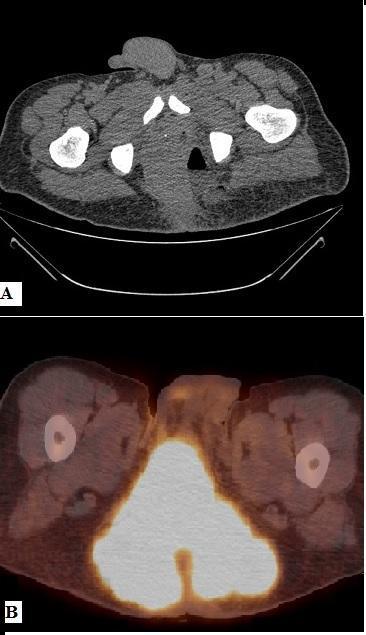 | Figure 1. A-CT Pelvis with contrast showing perianal mass. B- PET CT of Primary anal tumor |
 | Figure 2. A & B: T1 and T2 weighted images of sagittal section of spinal cord showing metastases |
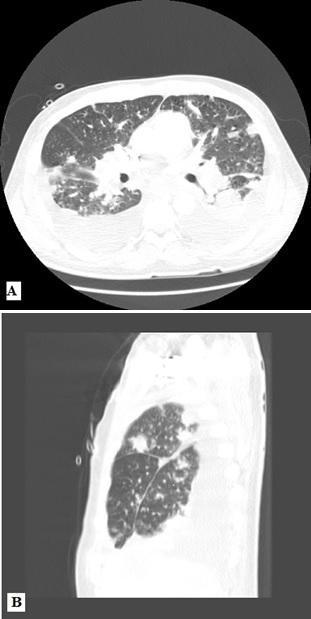 | Figure 3. A & B: Lung findings showing lymphangiticcarcinomatosis, bilateral pleural effusions with pleural thickening-metastatic pleural disease |
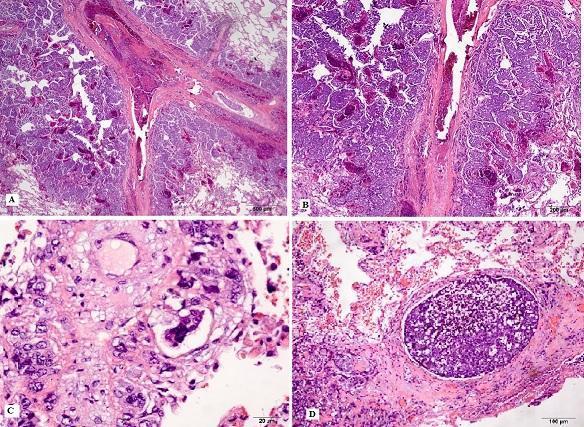 | Figure 4. A-Low power view of lung with tumor involvement and intra-vascular tumor emboli. HE stain, 2x. B-Medium power view of lung with tumor involvement by metastatic squamous cell carcinoma. Benign lung is visible in the lower outer corner. HE stain, 4x. C- High power view of tumor embolus. HE stain, 40x. Seen in heart, lung and vertebrae. D- Medium power view of sub pleural metastasis. A large tumor embolus dominates the image. HE stain, 10x |
3. Discussion
- Anal cancer comprises principally of two major morphologic variants: squamous cell carcinoma (SCC) and adenocarcinoma. In most settings, SCC compromises more than 70% of cases. Anal SCC is strongly associated with human papilloma virus (HPV, types 16-18) infection with 90%, 100%, and 58% among women, homosexual men, and heterosexual men, respectively (5). HPV can cause premalignant anal squamous intraepithelial lesions (ASIL) which can be low grade (LSIL) or high grade (HSIL). Progression of ASIL to invasive carcinoma is affected by HIV status, HPV subtype and titers, CD 4 count (6).Anal SCC usually spreads in a loco-regional manner within and outside the anal canal. Lymph node involvement at diagnosis is observed in 30-40% of cases while systemic spread is uncommon with distant extrapelvic metastases recorded in 5-8% at onset, and rates of metastatic progression after primary treatment between 10% and 20% (7). Metastasis occurs by lymphatic spread and local invasion into contiguous structures like rectum and bladder most of the time. Distant metastasis via hematogenous spread occurs in less than 2% cases (8). Hematogenous metastasis is very uncommon even in advanced stages of Anal SCC. Most common sites of distant metastasis when it occurs are to the liver or lungs. However, vertebral system may be involved in extremely rare situations via vertebral venous system (9). Only 1 case of vertebral metastasis (10) and no case cases of cardiac metastasis have been reported so far to the best of our knowledge.Incidence of anal SCC in the general population has increased lately which has been attributed to changes in sexual practices, incidence of HIV and HPV. Patients with HIV are more likely to have HPV infection and the risk of HPV infection evolving to HSIL and invasive anal cancer is also greater among these patients. As HPV vaccination cannot be given in immunocompromised HIV patients for primary prevention, we need to start early screening in HPV and HIV coinfected patients for anal cancer by doing regular anal pap smears. In early diagnosed cancers, cure can be achieved with loco-regional control. Our patient had genital warts for 10 years which progressed to aggressive anal carcinoma. Even with surgery and chemoradiation, the disease progressed to involve multiple organs causing fatal outcome. With this case, we want to highlight the importance of early detection of anal cancer in coinfected HIV and HPV patients.
4. Conclusions
- Anal SCC can be aggressive in HIV and HPV coinfected patients. We need research studies to see if early anal cancer screening is beneficial in these patients.