Rahul Kumar1, Neha Khambete2
1Dept. of Conservative Dentistry & Endodontics, M.G.M. Dental College & Hospital, Navi Mumbai
2Department of Oral Medicine, Diagnosis and Radiology. CSMSS Dental College &Hospital, Aurangabad
Correspondence to: Rahul Kumar, Dept. of Conservative Dentistry & Endodontics, M.G.M. Dental College & Hospital, Navi Mumbai.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Abstract
The most important development in surgical endodontics has been introduction of the surgical operating microscope. The use of magnification in endodontics is not an isolated development. It is part of trend in medicine and dentistry toward a quest for perfection and application of minimally invasive technique for procedures that previously required extensive surgery. But now microscopic endodontics has totally changed the way endodontics and endodntic surgery are practiced. Operating microscopes are also useful right from diagnosis, trying to locate extra canals or missed canals, assessing efficacy of newer systems for cleaning and shaping, to prevent / or manage endodontic mishaps.
Keywords:
Surgical Operating Microscope, Endodontics, Operative Dentistry
Cite this paper: Rahul Kumar, Neha Khambete, Surgical Operating Microscopes in Endodontics: Enlarged Vision and Possibility, International Journal of Stomatological Research, Vol. 2 No. 1, 2013, pp. 11-15. doi: 10.5923/j.ijsr.20130201.03.
1. Introduction
With the development of clinical techniques that require high levels of manual dexterity and involve fine detail, there is increasing interest in the use of magnification for dental procedures .Endodontic procedures were performed using tactile sensation and the only way to see inside a root canal was to take radiographs. Radiographs are inaccurate in that they are two-dimensional. In addition to radiographs, various magnification systems such as magnification loupes / telescopes have been used to perform conventional endodontics[1].However the introduction of surgical operating microscope has heralded a new era in endodontics. Operating microscopes are useful right from diagnosis, trying to locate extra canals or missed canals, assessing efficacy of newer systems for cleaning and shaping, to prevent / or manage endodontic mishaps[2]. According to the Zeiss company ,the microscope was first introduced to otolaryngology around 1950,then to neurosurgery in the 1960s,and to the endodontics in the early 1990s.With increasing failures in conventional endodontic therapy, microsurgery, which is based on the premise that light + magnification = excellence, has indeed come as a boon to endodontists[2].
1.1. How does the Surgical Operating Microscope Work ?[1, 2]
There has always been a doubt as to how, a microscope differs from a loupe. The dental microscopes uses the parallel beam path better known as “the Telescope system” which follows galilean optics wherein focus is at infinity and parallel beams of light are send to each eye thereby reducing strain on clinicians eye. Also, illumination with operating microscope is co-axial with line of sight. From the light source light is reflected through condensing lens to an array of prisms to the objective lens. From the objective lens the light is focused to the surgical field. From the surgical site the light is reflected back to the objective lens and then passes through the magnification changers. From magnification changers the light reaches the binoculars wherein the beam is split and the surgical field is seen through the eye piece. The telesocpic loupes follow the convergent beam path that is the Greenough system. To appreciate what a surgical microscope can do, it is vital to understand how it works. The main parts can be divided into 3 groups. 1) Magnification 2) Illumination3) AccessoriesI. Magnification is determined by : a) Eye pieces which are available in powers of 6.3X, 10X, 12.5X, 16X, 20X. It consist of 1) A viewing side with rubber cup2) Adjustable diopter setting (-5 to +5). 3) Binoculars which is used to hold eye piece which may be straight, inclined or inclinable and again of shorter or longer focal length. b) Magnification changer which may be a 3/5 step manual changer or power zoom charger. c) Objective lenses whose focal length (which ranges from 100 mm to 400 mm) determines the operating distance between lens and surgical field.II. Illumination : Is mainly by means of a 100 watt Xenon halogen bulb, where intensity is controlled by a rheostat and cooled by a fan. Illumination is mainly co-axial with line of sight, which means that light is focussed between the eye pieces so that no shadows will be visible. This is possible due to the usage of Galilean optics. III. Accessories:1) Pistol or bicycle grips2) Liquid crystal display (LCD) and high resolution monitors which receives video signals from cameras. 3) Integrated video camera4) Eye piece with rectile field: used for aligning during video taping and 35 mm photography. 5) Auxiliary monocular or articulating binocular for dental assistant.
1.2. Clinical Applications[3]
I. In Conventional Endodontics :An operating microscope aids for better performance; 1) By visualizing root canal system in finer detail, thus cleaning and shaping more efficiently[4]. 2) It is important that the root canal system is dry before obturation is done. It is only by examining the root canal with microscope that it is possible to determine if canal is dried sufficiently. 3) By means of adequate illumination and magnification access is enhanced; as subtle color change in floor of pulp chamber aid the operator in finding opening to sclerosed and fine root canals. 4) In cases where root end closure is to be undertaken, it is possible to view tissues beyond apex of root canal. 5) Examination of root canal under magnification ensures that air voids in canals are kept a minimum even for a base of coronal access sealing. 6) In cases of re treatment like post removal; the higher magnification and illumination helps in differentiating between tooth structure and various restorative cements. By this, there is more conservative post removal which gives better prognosis. 7) Retrieval of broken instruments like file and reamers is possible. Usually these instruments are manufactured round whereas the root canal systems are rarely perfectly round and thus the instruments binds in some irregular portion of the canal. The microscope provides invaluable light source and magnification to view the internal aspect of the root canal. 8) Microscopic management of endodontic procedural errors :eg. In perforation repair, the increased magnification and dual light source of the microscope is invaluable to diagnose and locate accurately the exact perforation site. Incremental placement of restorative material like the Mineral Trioxide Aggregate over the perforation site can be carried out successfully and precisely under a microscope.[5, 6]
1.3. Modern Microscopic Endodontic Procedure Sequence[2]
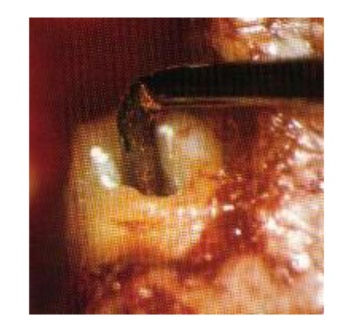
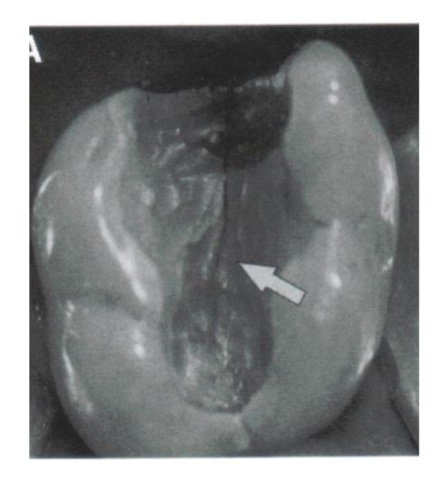
1) The diagnosis indicates that endodontic treatment is needed and tooth is anesthetized.2) Following placement of the rubber dam, access is made. The microscope is not needed for this step, although some clinicians may prefer to use it.3) Using the microscope at low to mid magnification, the pulp chamber is thoroughly prepared using a Buc tip size 2 for inspection.4) Under high magnification (16x-24x), the floor of the chamber is examined for additional canals because more than 50% of molar teeth have a forth canal. 5) After the canal entrance is identified, the microscope is not needed until a later stage. The apex is negotiated with a size 10 K file and is then enlarged with size 15 or 20 files.6) Gates –Glidden burs are used in reverse order to enlarge the coronal half or two thirds using the crown down techniques.7) An apex locater is used to determine the canal length at this stage.8) NiTi rotary instruments now employed to prepare the remaining one half or one third of the apical canal in the crown down technique. The final apical preparation of the master apical file is done by hand instruments and light Speed, depending on the orginal canal width or estimate of working width.9) The microscope is used to check the preparation and to check again for additional canals.10) A master gutta percha cone is selected,the canal length and solid “tug back” is assured.11) After obturation microscope is used again for final check. Finally, the canal is filled with temporary cements.I. In Surgical Endodontics[1,5,7]:The microscope and the new micro instruments, specific to needs of endodontic microsurgery have made the microsurgical approach a reality by meeting all the needs of a microsurgery triad i.e. 1) Magnification2) Illumination3) MicroinstrumentsMagnification: at 3 different levels1. 2.5 X to 8 X for orientation of operating field.2. 10 X to 16 X - midrange magnification, are best for performing root-end resections and root- end preparations.3. 18 X to 30 X to observe and evaluate fine details – micro fractures, isthmus etc.Illumination, which is simultaneous and focused, is an added benefit to magnification.Micro instruments such as ultrasonic instruments aid in root end preparation with greater accuracy and conservation of root.Now apical surgery can be performed with accuracy and predictability, eliminating the guess factor inherent in conventional endodontic surgery. 1) Conservative and Co-axial root end preparation: Microscope along with the micro instruments permit conservative, co-axial root end preparations and precise retrofills satisfying all the requirements for mechanical and biological success (Fig.3). The micro instruments include micro mirror, micro needles and blades with circular handles which makes the designing of the flap easier. 2) Identification of apex in intact buccal plate: Sometimes, identification of exact apex, especially of posterior teeth is difficult, necessitating unnecessary removal of cortical bone; making the osteotomy site excessively large. Using a microscope; early clear identification keeps the size of osteotomy and healthy bone removal to minimal. 3) Inspection of resected root surface: Using the microscope, the orifice, isthmus etc can be viewed more distinctly whereas in old methods there was more of assumption.4) Bevel angle: With conventional endodontic surgery, a bevel angle of 45o was suggested for better accessibility; though no bevel angle would be best. With the help of retrotips, micro mirrors etc., the ideal bevel angle of less than 10o can now be met, thus decreasing microleakage.[8]5) Retropreparation : Resection perpendicular to the long axis and confirming to the true anatomic configuration of the root canal system is possible. Also clean, parallel walls which are conservative can be prepared[9]. 6) Retrofilling : Precise retrofilling becomes possible[9]II. In Restorative dentistry:[10]1) Removal of caries most conservatively. Since the tooth can be seen magnified it is easy to view the extent of caries and thus there is no need to remove healthy tooth structure blindly. 2) Identification of crack lines, microgaps between the tooth and a filling becomes easier due to enlarged vision . III. In Dental Extractions:Magnification improves a dentist's ability to detect tooth particle perimeters and to determine if luxation forces applied using elevators result in microscopic incremental improvements in tooth particle luxation. Magnification also improves a dentist's ability to distinguish between tooth structure and alveolar bone, which is useful when sectioning teeth and removing intra-socket alveolar bone to facilitate forceps extraction. In dentistry, the use of microscopes may facilitate a dentist's ability to perform dentoalveolar extractions with more conservative removal of alveolar bone, potentially minimizing trauma to the extraction site.[11]IV. In Periodontal Therapy:In periodontal procedures surgical microscope can be used for, 1) Diagnostic procedures 2) Crown lengthening 3) Regenerative periodontal surgery 4) Root coverage procedures 5) Papilla reconstruction 6) Smile designing and 7) Implantology.[12]V. Use of fewer radiographs. For procedures like post space preparation etc, as its possible to see at least till middle third with the magnification rather than depend on radiograph. VI. Patient education through its integrated video. Adding color video prints of the procedure is welcome by the patients as this gives them a better idea of what treatment is being done or going to be done. This also allows the clinician to show them the astounding spectrum of modern dental practice available. VII. Documentation for dental legal purposes. In dentistry, documentation was mainly with the help of radiographs, but with the accessories of a surgical microscope important parts of a procedure, which, for instance, may illustrate why a previous treatment failed can be shown in a court of law or an insurance company. VIII. Management of procedural errors like crown and root perforations; overfilled and underfilled canals, loss of patency owing to blockade by ledge formation etc. is better due to better vision with the magnification and fiber-optic light. IX. Best cosmetic outcome and tissue conservation by use of the thinnest suture threads and flap designs like the papilla base incision which is otherwise never possible under the naked eye. X. Contrast: With the help of filters, we can enhance contrast with tissue and during bleeding. XI. Ergonomics With a capital “E” is possible due to the high mobility and ergonomic working position which reduces the occupational stresses.  | Figure 1. A typical surgical microscope |
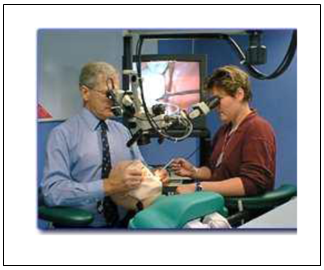 | Figure 2. Auxiliary monocular for dental assistant |
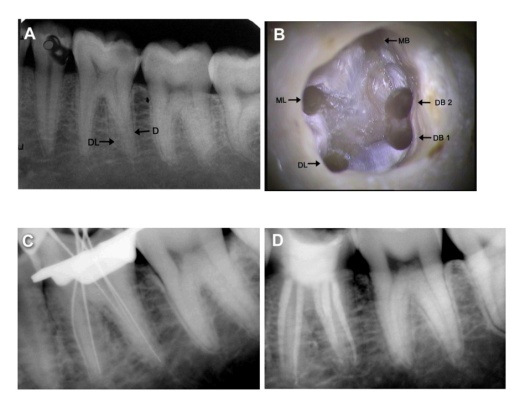 | Figure 3. Modern conventational endodontic procedure sequence |
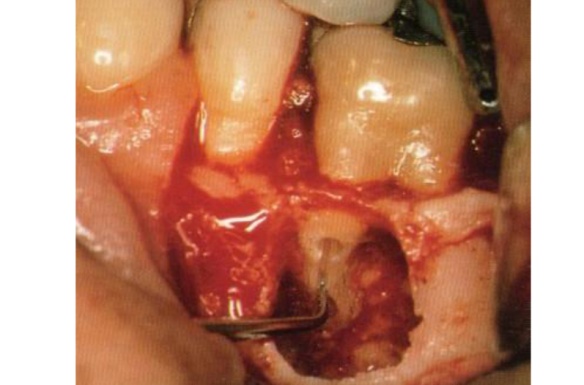 | Figure 4. Conservative and Co-axial root end preparation |
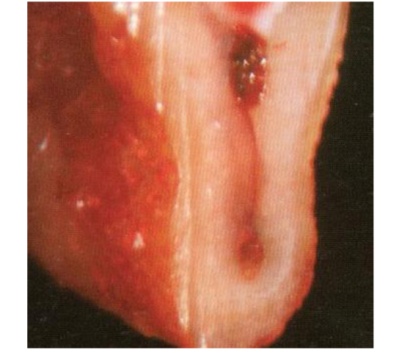 | Figure 5. Isthmus of root canal |
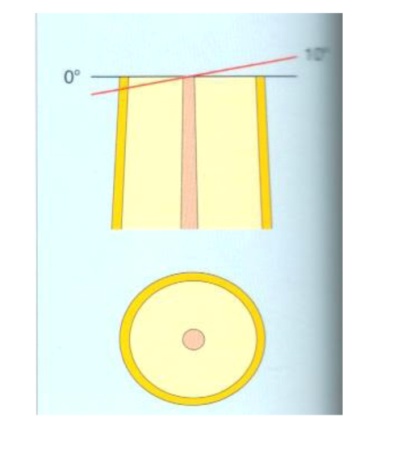 | Figure 6. Bevel angle |
 | Figure 7. Precise root end preparation |
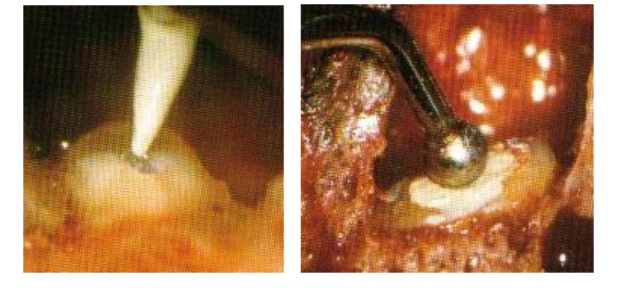 | Figure 8. Retrofills with IRM |
 | Figure 9. Identification of microgaps |
 | Figure 10. Ergonomic working position for operating microscope |
| Table 1. Comparison between conventional endodontic surgery and microsurgery[6,7] |
| | 1. | Osteotomy size | Approx. 8-0 mm | 3-4 mm | | 2. | Bevel angle degree | 45-65 degrees | 0-10 degrees | | 3. | Inspection of resected root surface | None | always | | 4. | Isthmus identification & treatment | Impossible | always | | 5. | Root-end preparation | seldom inside canal | always within canal | | 6. | Root-end preparation instrument | Bur | ultrasonic tips | | 7. | Root-end filling material | Amalgam | MTA* | | 8. | Sutures | 4 x 0 silk | 5 x 0, 6 x 0 monofilament | | 9. | Suture removal | 7 days post-op | 2-3 days post-op | | 10. | Healing Success (over 1 yr) | 40-90% | 85-96.8% |
|
|
1.4. Drawbacks
Some of the drawbacks of the operating microscope are[13,14,15]; 1) It’s expensive. 2) Its size which is difficult to fit in a small operatories. 3) It takes the operator some time to get used to the equipment. 4) Need for expertise by auxiliary staff5) Adaptation to indirect vision6) Narrower field7) Movement of the patient
2. Conclusions
Those who perform endodontic procedures without the microscope are still evaluating the benefits of its use. Practicality is the key concern. After the initial learning curve, endodontic procedures can be done in less time because of the greater visibility of the root canal anatomy and procedural errors can be reduced. The key to successful endodontic practice lies in the operator and his or her commitment. If sincere effort is made , one can be rejuvenated and endodontics will be more enjoyable.
References
| [1] | Microscopes in Endodontics. DCNA, July 1997; 41 (3) ; 391-619. |
| [2] | Modern endodontic practice DCNA JAN 2004 48(1), |
| [3] | Carr GB: Microscope in Endodontics, J Calif Dent Assoc. 1992, 20: 55. |
| [4] | De Carvalho, Zuolo: Orifice locating with a microscope. J Endod. Sept. 2000 ; 26 (9) ; 532-4. |
| [5] | Firas Daoudi: Microscopic management of endodontic procedural errors: perforation repair. Dent-Update. May 2001 ; 28 (4); 176-80. |
| [6] | Biswas M, Mazumdar D, Neyogi A.Non surgical perforation repair by mineral trioxide aggregate under dental operating microscope. J Conserv Dent. 2011 Jan;14(1):83-5. |
| [7] | Gartner AH, Dorn SO: Advances in endodontic surgery. DCNA. 1992, 36: 357-78. |
| [8] | Carr GB: Surgical Endodontics. In Cohen S, Burn RC, editors. Pathways of Pulp, Ed.7, St.Louis, 1998, Mosby. |
| [9] | Githeany PA, Figdor D, Tyas MI : Apical dentin permeability and microleakage associated with root end resection and retrograde filling. J Endod. 1994, 20 : 22-26. |
| [10] | Weller RN, Kim S: Incidence and position of canal isthmus-I. Mesiobuccal root of maxillary first molars. J Endod. 1995, 21: 380-383. |
| [11] | Mamoun J. Use of high-magnification loupes or surgical operating microscope when performing dental extractions. N Y State Dent J. 2013 Apr;79(3):28-33. |
| [12] | Hegde R, Sumanth S, Padhye A. Microscope-enhanced periodontal therapy: a review and report of four cases.J Contemp Dent Pract. 2009 Sep 1;10(5): E088-96. |
| [13] | Michaelides P.L. : Use of operating microscope in dentistry. J Calif Dent Assoc. Jun 1996 ; 24 (6) ; 45-50. |
| [14] | Pecora G., Andreana S. : Use of dental operating microscope in endodontic surgery. Oral Surg Oral Med Oral Pathol. Jun 1993 ; 75 (6); 751-8. |
| [15] | Kim S, Pecora G, Rubinstein RA: Colour atlas of microsurgery in endodontics. W.B. Saunders Company, 2001. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML