-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Stomatological Research
p-ISSN: 2326-1129 e-ISSN: 2326-1153
2013; 2(1): 1-4
doi:10.5923/j.ijsr.20130201.01
Mandibular Canine with Two Root Canals – An Unusual Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLVipin Arora, Vineeta Nikhil, Jatin Gupta
Department of Conservative Dentistry and Endodontics, Subharti Dental College & Hospital, Meerut,250005, India
Correspondence to: Vipin Arora, Department of Conservative Dentistry and Endodontics, Subharti Dental College & Hospital, Meerut,250005, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Mandibular canines present a complex internal anatomy. There are reported cases of canines with a single root and two canals, three canals, two roots or fused roots. The existence of mandibular canines with more than one root canal is a documented fact that clinicians should keep in mind, in order to avoid failure during endodontic treatment. In spite of the low incidence of lower canines with one root and two canals, this possibility should not be ignored, inasmuch as the presence of a second canal in these teeth leads to difficulties in endodontic treatment. The precise knowledge of the internal dental anatomy is essential for the success of the root canal therapy, because the failure to detect the extra canals and the incomplete radicular obturation leads to the infection of the periapical space, which ultimately results in the loss of the tooth. The long-term success of the restorative treatment depends directly on the quality of the endodontic treatment realized on the abutment teeth. The mandibular canine is very important as abutment for any type of restoration. This article presents a case of a patient with mandibular canine having two root canals ,which lead us to conclude that such anatomical variations also occur in india as much as described in the international literature and cannot be overlooked when treating the teeth.
Keywords: Mandibular, Canine, Two Root Canals
Cite this paper: Vipin Arora, Vineeta Nikhil, Jatin Gupta, Mandibular Canine with Two Root Canals – An Unusual Case Report, International Journal of Stomatological Research, Vol. 2 No. 1, 2013, pp. 1-4. doi: 10.5923/j.ijsr.20130201.01.
1. Introduction
- The anatomy of the root canal system determines the parameters under which the endodontic treatment is performed and directly affects the success of the root canal treatment. The majority of the problems that occur during the root canal treatment are due to the insufficient knowledge of the anatomy of the pulp space[1]. The main documented reason for failure of the endodontic treatment is the inability to obturate one of the root canal because of ignoring the variations of the internal and external dental anatomy of the tooth. In order to perform a quality endodontic treatment, which will ensure the tooth’s long term durability, it is imperative that the dentist takes into account the morphology of the radicular canals and the variations of the entire canalicular system before initiating the endodontic treatment.From a morphological standpoint, mandibular canine is usually a monoradicular tooth. The internal anatomy of the radicular canals doesnot always correlate with the outer shape of the tooth. The mandibular canines do not always display the basic anatomy that we expect with one root and one canal. The proof is given by the various studies in which research was done on both the morphology of the monoradicular canines and the presence of those, which can display two radicular canals. It is important that this fact be taken into account in order to prevent the failure of the endodontic treatment and the subsequent loss of the tooth. Generally, mandibular canines contain a single root and root canal[2-5]. The occurrence of two canals and even more two roots is rare, ranging from 1%[4] to 5%[5].Although the prevalence is low, but the clinicians should consider all the possible variations in the number of roots and pulp canals of mandibular canines. This paper reports a case of a patient with mandibular canine having two root canals
2. Case Report
- A healthy, 40 year old female was referred to the Department of Conservative Dentistry and Endodontics with a chief complaint of pain in lower left region. The pain lingered for several minutes even after removal of the stimulus and led to a disturbed sleep. Clinical examination revealed large carious lesions, associated with mandibular left canine and mandibular left premolar. Electric pulp test was done for both the teeth. Mandibular left canine gave an exaggerated response to the electric pulp test. It was tendor on percussion as well while mandibular left first premolar was not tendor.Initial periapical radiographic examination (Figure 1) revealed carious lesions approaching pulp in mandibular left canine and first premolar.
 | Figure 1. Photograph of Initial diagnostic intraoral periapical radiograph showing carious lesions approaching pulp in mandibular left canine and first premolar. Two roots are also evident in mandibular premolar |
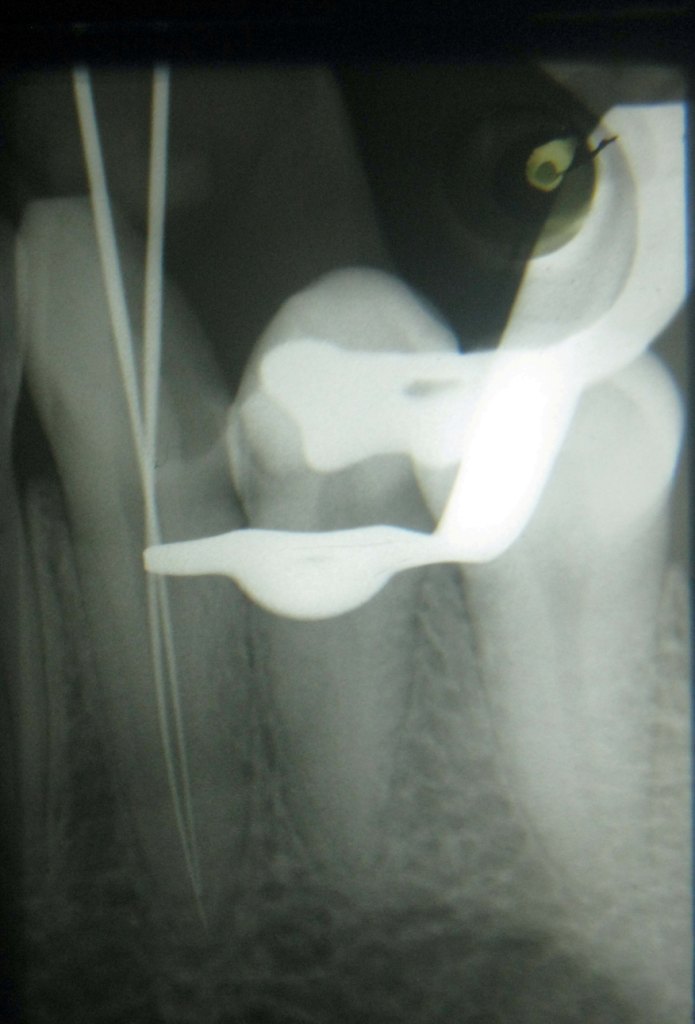 | Figure 2. Photograph of Intraoral periapical radiograph for working length determination showing two canals in mandibular left canine |
 | Figure 3. Photograph of Intraoral periapical radiograph of mandibular left canine with master cones |
 | Figure 4. Photograph of Intraoral periapical radiograph of mandibular left canine with obturation |
3. Discussion
- The mandibular canine is the second longest tooth in human dentition. It is only few millimeters shorter than the maxillary canine. There is usually one canal present which usually exits in a single foramen at the apex. At times, two root canals, rarely three root canals or two roots can be present. So, the complex nature of root canal morphology of mandibular canines should be thoroughly understood because additional root canals if not detected, can be a major reason for failure of root canal treatment. Care should be taken during initial radiographic examination as well as during access preparation because exploration and location of canal orifices act as a guide to navigate the canals [6]. We found two root canals in this case, one buccal and one lingual. Since it was clear clinically as well radiographically that two canals were present, so extra investigations such as CBCT were not planned because of concerns regarding radiation dosages.The root canals in mandibular canine are more flattened and less round than in the upper canine, but are quite large and usually does not cause much of technical problems during instrumentation. Mandibular canines presenting with two roots are more difficult to instrument and clean. The long axis of the canal meets the crown surface at the incisal edge or on the labial surface. If this is not taken into consideration, it may lead to a deviated preparation, the emphasis again being on the labial side of the canal. The lingual canal must always be searched for using a small file with a curved tip. The Mandibular canine is often quite straight, but sometimes the root tip and the canal curve distally or labiallyWe infer that the dentist should always search for two canals in mandibular canines during endodontic treatment. The published literature also supports our inference. Various studies have been carried out in different parts of the world on different races and used different methods. Genetic variations among populations also affect anatomy of tooth. Lambrianidis et al (2001)[7] also stated that variations could be due to the differences in genetics and racial variations in the population, sample size, techniques, classification systems and the researchers’ judgment and diagnosis..Pécora JD et al (1993)[8] studied the internal anatomy, the direction and the number of roots of the mandibular canines. The study was done on 830 mandibular canines, and the results showed that 98.3% had only one root and of these 97.2% had one canal and one opening orifice, 4.9% two canals and one orifice, 1.2% two canals and two orifices. Two canals and two roots were present in only 1.7% of the cases. In 2006, Bakianian V et al.[9] analyzed 100 canines after making transversal slices. They detected the presence of two canals in 12% of the cases. Similar results were obtained by Kaffe I et al (1985)[10], in a radiological study on 400 mandibular canines, in vivo, which showed a percentage of 13.75%. Without a significant departure from these percentages, Green D (1973)[11] also reported 13% after analysing 100 teeth. Hession R W(1977)[12] reported 11% in his study.Pineda F and Kuttler Y (1972)[2] reported 18.5% of the mandibular canines having two canals in a study on 187 radiological images. A very similar result was obtained by Calişkan MK et al (1995)[13], in a study of 100 mandibular canines, the actual number being 19.5%. Much greater percentages were observed by Sert S et al.(2004)[14], and by Vertucci FJ (1974)[15], with 24% and 22% respectively. On the other hand, the study of Bellizzi R and Hartwell G (1983)[16], which included examination of 195 mandibular canine X-rays showed a low percentage of 4.1%. In a rare case report, Orguneser A and Kartal N (1998)[17] reported mandibular canine with three root canals. Heling I et al (1995)[18]reported a case of mandibular canine with two roots and three root canals. D’Arcangelo C (2001)[19] carried out Root canal treatment in mandibular canines with two roots.The presence of such cases lead us to think that such examples could be encountered in the indian population as well and as evidenced by the case presented.It is very important to detect such anatomical variations in the permanent teeth, so that the endodontic treatment can be performed appropriately. The dental anatomical knowledge is an essential condition in the practice of endodontics. So, prior to the beginning of the treatment, a thorough knowledge of the root canal anatomy is important. A high prevelance of two canals and two roots have been reported by various authors so if extra canals are suspected then radiographs from several different angles should be taken and a careful endodontic exploration may lead to identification of additional canals and is certainly essential to give the highest possible chance for success.
4. Conclusions
- This case report describes a case of mandibular canine with two distinct canals. So, a clear understanding of pulp anatomy and the variations that occur in it are essential if effective cleaning, shaping and obturation of the pulp space are to be achieved. Generally mandibular canines have one root and one root canal, but some variations can occur which should be identified and managed. The radiographs and magnification devices can be very helpful in diagnosing and treating such complicated cases. The practitioner should be aware of how many canals to expect, their location, length and relationship to each other. The large number of atypical cases from a morphological standpoint that occur throughout the world along with the very important role that the canine plays as an abutment tooth in the future prosthetic restoration, fully justifies the importance of understanding the radicular anatomical variations.